It’s been hot in London this week. Really hot. A dangerous heat wave has hit Western Europe. Yesterday, the UK recorded its highest ever June temperature at 36.1 °C (about 97 °F). But as the weather app on my phone confirmed, it felt like 39 °C.
It’s frightening that we are seeing such temperatures in the UK in June. According to the Met Office, the country’s national weather and climate service, June temperatures peaked at an average 19 °C (66 °F) in England between 1991 and 2020. Across Europe, the heat wave is likely to cause thousands of deaths. There will be other awful consequences for agriculture, infrastructure, and the health system.
But this week I want to look at what the heat does to our minds and brains. Personally, I’ve found it almost impossible to think straight. The heat is distracting and my mind is foggy. I dread to think about the conditions of people who work outdoors, in even hotter regions.
It’s not just exhaustion and confusion. The effects of heat on the brain can be deadly. And researchers are still trying to figure out why.
Studies have confirmed that as temperatures rise, people seem to get more irritable and more violent. Most of these studies are based on associations, though. It’s difficult to directly study how a heat wave might affect our thinking, says Catherine Thompson, a cognitive psychologist at Liverpool Hope University.
She has been studying the effects of extreme heat on firefighters instead. It’s easier to measure people’s cognitive skills before and after they undergo scheduled training that involves entering a burning building.
It’s early days, but the team found that firefighters found it harder to focus and control their attention immediately after heat exposure—something people in heat waves can empathize with, I’m sure.
The firefighters’ skills returned to normal after 20 minutes or so of cooling down. But they’d experienced just 15 minutes of intense heat exposure. Thompson doesn’t know what the effects of living through a days-long heat wave might be—or how long they’ll last. Figuring that out might involve shipping cognitive test kits to thousands of people during the few days’ notice of an impending heat wave. “My guess [is] that no one’s done it because it’s just so difficult to do,” says Thompson.
Still, researchers can learn about some of the impacts of heat waves through studies after the fact. And those studies suggest that the heat seems to have more disastrous outcomes for people with mental-health disorders.
Those outcomes become apparent when temperatures rise above what is considered typical for a given region. “There seems to be a correlation where the hotter it gets, especially during the hottest times of the year, the worse the mental-health outcomes,” says Joshua Wortzel, who directs the Heat-Mind Lab at Hartford HealthCare in Connecticut.
In a study published in 2023, Emma Lawrence at the University of Oxford, who studies the effect of climate change on mental health, and her colleagues reviewed the evidence linking mental-health outcomes to ambient outdoor temperatures. They found that during heat waves, there was a 9.7% increase in the rate of hospital admissions for people with such conditions.
“People who live with mental-health conditions are among the most susceptible to the physical impacts of heat,” says Lawrence. People with schizophrenia were found to have been three times more likely to die during the record-breaking heat wave that affected Canada in 2021, for example.
In order to protect people, we need a better understanding of the mechanisms underlying these effects. After all, a lot of things change when it’s very, very hot. Some people may end up stuck indoors, avoiding outdoor play and exercise, and it can be difficult to get a good night of sleep, for example. Sleep, socializing, and exercise are all really important for our mental health.
But whether unusual heat does something specific to our brains is, as Wortzel puts it, “the million-dollar question.”
Research in lab animals suggests that excessive heat can alter the way chemical signals work in our brain. The levels of neurotransmitters like serotonin, for example, seem to increase when rats and mice are exposed to high temperatures, according to multiple studies. The heat may also interfere with the way networks in our brains communicate with each other. It might affect the way oxygen reaches our brain cells.
“There are so many biological reasons why brains may be negatively affected by heat,” says Wortzel.
Emerging research suggests that for whatever reason, children and young people are among the most vulnerable. In research published earlier this week, Wortzel and his colleagues saw a 2.97% increase in the suicide rate among people in the US aged 15 to 24 for every 1 °C increase in average monthly temperature. That’s more than double the increase seen in people over the age of 24 (which is concerning in its own right).
Other work hints that heat exposure might have long-term consequences for children’s brain development. Babies who were exposed to either extreme heat or cold appeared to have altered white matter by the time they were nine to 12 years old—although it’s not clear how these impacts might affect an individual child.
“It seems that extreme temperature exposure for very young children may affect their brain development,” says Lawrence, who spoke to me from Oxford. She was meant to be in London for Climate Action Week, but her event, which focused on extreme heat, ended up being canceled … owing to the extreme heat.
We are living through the effects of climate change. And that brings a new urgency to the question of how heat affects our brains. Children born in 2020 are predicted to experience around seven times the number of heat waves their grandparents did, says Lawrance. “[We] need to be serious about adapting to a warming world.”
Khaleej Times reports that more than 100 people have died “following the intense heatwave” in the southern Indian states of Andhra Pradesh and Telangana. It adds that “[m]ore than a dozen districts saw temperatures above 45C” in Andhra Pradesh, with temperatures “soar[ing]” over 48C in its East and West Godavari regions. According to ETV Bharat, Telangana’s Warangal registered 23 heat deaths, the highest in the region. While national crime record data says Telangana recorded 116 heat deaths in 2024, the state’s 2026 heatwave action plan “places the deaths at just 10 for the same period”, according to the New Indian Express, sparking concern that “the true human cost of extreme heat may remain invisible in official records”. In the neighbouring eastern state of Odisha, the state government confirmed that three people died of sunstroke, reports the New Indian Express.
Meanwhile, doctors tell the Independent that health impacts are “getting worse” because of record night-time temperatures, with Delhi recording “its warmest May night in almost 14 years” this week. As temperatures approach 46C in the capital today, authorities warn that heatwave conditions will continue over large parts of central and north-western India, says the Indian Express. According to Down to Earth, the current heatwave is pushing India’s power grid into “uncharted territory”, with “residential cooling demand now overtaking industrial demand growth in several regions”. An opinion piece in the Hindustan Times by health researchers argues that heat mortality is not caused by “temperature alone”, but “infrastructure design failure” and “severely limited access to cooling”.
The UK and Europe have experienced “mind-boggling” new temperature records for May amid a deadly heatwave, reports the Financial Times. The extreme heat has been linked to “about a dozen” deaths across the region, the newspaper says, adding: “Temperatures hit 35.1C in London on Tuesday, breaching the record of 34.8C set the previous day, according to provisional readings from the UK’s Met Office. This was 2C higher than the previous May record set in 1944. A new record was also set in Ireland on Tuesday, and agencies said France could reach new highs under a so-called heat dome where warm air from northern Africa is trapped by a high-pressure system over western Europe.” The FT quotes Prof Peter Thorne, director ICARUS Climate Research Centre at Maynooth University, who calls the temperatures “mind-boggling crazy”.
The Associated Press reports that the UK “smashed a century-old temperature record for the second time in 24 hours on Tuesday”. It adds that London experienced a “rare ‘tropical night’, defined as one in which the temperature does not fall below 20C”. It adds: “Records also fell in France, where temperatures reached 36C on Monday in the country’s southwest and widely remained above 20C at night.” France’s national weather service, Météo-France, said that its “heat dome” was “producing temperatures more than 10C above what is usual for this time of year”, according to the newswire. ABC News says the heatwave has been linked to 11 deaths in the UK and France. This includes seven people in France, five of whom died by drowning and two who suffered heat-related deaths while competing in sporting events, says the Guardian. The Independent reports that four teenagers also drowned in the UK amid the record heat. France24 reports that “restrictions on outdoor work were imposed in parts of Italy”. CNN adds that, in the UK, “a wildfire broke out near Arthur’s Seat, a hill in Edinburgh, Scotland, and hundreds of properties in south-east England were left without water as demand spiked”.
Several publications look into why Europe is experiencing a record heatwave and the links to climate change. BBC News says: “The immediate cause of the heatwave is a ‘heat dome’ – where an area of high pressure gets ‘stuck’ over Europe, trapping warm air underneath. But scientists have little doubt that human-caused climate change – largely the result of the burning of coal, oil and gas – has supercharged the heat.” Richard Betts, head of climate impacts research at the Met Office and a professor at the University of Exeter, tells BBC News: “When we have a heatwave it’s happening more severely, because it’s on top of a warming climate. I’ve been a climate scientist for 33 years and we’re seeing exactly the kinds of things that we were warning back then… [although] these records are perhaps more extreme and coming sooner than we had expected.” The Independent reports that the heatwave “has the fingerprints of climate change all over it”. The Guardian examines why heat can be a “silent killer”. Sky News has a video on whether the UK can expect more record-smashing heat. Inside Climate News and Scientific American also cover the climate links.
Chennai was not on the list this time, but is no stranger to high temperatures. In the south-eastern coastal capital of Tamil Nadu, extreme humidity and heat are inescapable facts of life.
“The heat is by no means manageable, but we have no choice but to deal with it,” said Mohammed S, a 29-year-old grocery platform delivery worker, speaking to Carbon Brief.
Last year, Chennai became India’s first ever city to roll out air-conditioned lounges for millions of gig workers, like Mohammed, navigating India’s increasingly hotter cities.
Gig workers leave their slippers outside the lounge. Credit: Ishan Tankha / Scorched
Through the building’s tinted windows, workers wearing synthetic jerseys emblazoned with food delivery app logos are stretched out on wooden benches meant to seat 25 people.
The lounge has charging points for phones, a water cooler and a unisex toilet. It might not seem like much, but workers tell Carbon Brief that it has made a “huge difference” to their lives – even on a day when the air conditioner stopped working.
“Before this, life was very difficult,” said Mohammed. He continued:
“We would park our [electric] bikes and try to find a tree to sleep under, stop for tea and tea shop owners would tell us we couldn’t sit there for more than 10 minutes, try to rest in a building’s stairwell and be chased away, then try to find shade under a flyover. Now we can sit in the AC and avoid the worst of the heat.”
Dinesh, 27, said his day starts at dawn before the sun is up, picking up packages from companies in north Chennai – another critical heat hotspot.
For the next seven hours, there is no “off point” or breaks for Dinesh as apps rush deliveries.
Some of Chennai’s gig workers told Carbon Brief they try to avoid the worst of afternoon temperatures from noon to 3pm, but for many – especially migrant workers – sitting back in the lounge is not a choice they can afford. One of them explained:
“If you don’t have cash to cover your bills or have to send money back home, you head out into the heat for a 12-hour shift and hope for the best.”
Dinesh checks his orders in the gig worker’s lounge. Credit: Ishan Tankha / Scorched
Feeling ‘gear’
In Chennai, heat might be normalised, but it has its own vocabulary. Speaking to Carbon Brief, the city’s gig workers, auto rickshaw drivers and fish sellers used an all-encompassing term – “gear” – to describe their symptoms, including dizziness, exhaustion and nausea.
Last summer, researchers offered Delhi’s gig workers a Rs 200 (roughly £2) cash transfer on the first day of a heatwave, to provide them with a means to achieve “real-time” adaptation to heat risk. Workers who received a cash transfer reported fewer heat-related symptoms, according to the study.
Asked if they would accept similar incentives to stay home on 40C days, workers in the T Nagar lounge expressed disbelief. Dinesh – who also trains technicians on how to repair air conditioners to support his income – told Carbon Brief:
“They [the apps] offer us incentives to go out in the heat when there are fewer riders.”
Barring a few, none of the dozens of outdoor workers Carbon Brief spoke to had an air conditioner at home or in their hostels, making the lounge the only place they could cool down.
Anna Bawden Health and social affairs correspondent
Sat 16 May 2026 05.00 BST
The climate crisis should be declared a global public health emergency by the World Health Organization, or millions more people will die unnecessarily, leading international experts have said.
The international spread of vector-borne disease, such as dengue and chikungunya, as well as the health impacts of extreme weather events, global heating, food insecurity and air pollution make a Pheic necessary, said the commission’s report, which will be presented to European ministers on Sunday before the WHO’s world health assembly starts on Monday.
Pheics are the highest level of health alert. Previous declarations include infectious diseases such as Covid and Mpox. While declaring one would not on its own reverse climate change, it would trigger the kind of coordinated international response that the scale of the health crisis demands but has not yet materialised.
The 11-strong independent commission, which includes former health and climate ministers, said: “Far from being a fading priority or fake news, climate change poses an immediate and long-term threat to health, economic, food, water, environmental, personal, community and national security.”
Andrew Haines and Katrin Jakobsdóttir, the commission’s chief scientific adviser and chair respectively. Photograph: WHO/Hedinn Halldorsson
In an interview with the Guardian, Katrín Jakobsdóttir, a former prime minister of Iceland who chaired the commission, said: “The climate crisis may not be a pandemic, but it’s still a public health emergency that threatens humanity’s very health and survival. And if we don’t act more quickly and comprehensively, many millions more people could die or face life-changing illness.”
Sir Andrew Haines, a professor of environmental change and public health at the London School of Hygiene & Tropical Medicine, and the commission’s chief scientific adviser, said: “WHO has already recognised that climate change is a major threat to global health. What we’re asking for is a step further.”
He added: “If we carry on emitting at current rates, that will accelerate the risks to health for both current and future generations including: more people suffering and dying from excess heat, floods and infectious diseases, air pollution from wildfires, more preterm births and more food insecurity.”
The commission also urged governments to stop subsidising fossil fuels, which are directly responsible for 600,000 premature deaths a year in Europe alone. The region spends about €444bn (£387bn) a year on subsidies for oil and gas production, the report said. In 12 European countries, fossil fuel subsidies exceeded 10% of national health expenditure in 2023 and in four exceeded the entire health budget, the report observed.
“This is not a sustainable energy policy. It’s really more of a public health failure,” Jakobsdóttir said. “And it’s one that could get a lot worse. New subsidies for fossil fuels as well as countries considering redrilling in the wake of the Iran crisis would be catastrophic for health.
“European governments are subsidising the very industries responsible for their own citizens’ premature deaths. We need health leaders to really step into the climate debate and not just be on the receiving end of it.”
The commission urged governments to stop subsidising fossil fuels, which are responsible for 600,000 premature deaths a year in Europe. Photograph: Christopher Furlong/Getty Images
The report also called for measures to tackle disinformation, greater use of national climate health impact assessments, as well as recognition that climate change was also a mental health crisis.
Jakobsdóttir said: “The way to challenge climate scepticism and misinformation is simple: make it personal. Climate change is not happening somewhere else, to someone else, in the future. It is shortening lives in European cities right now. It is filling hospitals. It is driving anxiety and stress and other mental health issues. And the policies that would fix it – clean air, active travel, insulated homes, sustainable food – are exactly the policies that make people healthier and happier today.
“When the health argument and the climate argument are the same argument, it becomes very hard to oppose.”
The report also recommended that countries’ healthcare systems needed to become more resilient to the rapidly changing environment in order to try to adapt as much as possible.
“Every country needs to be aware of where its health facilities are situated, how likely it is to be flooded and how they would deal with an extreme and prolonged heatwave,” Haines said, pointing out that hospitals were often built on floodplains and frequently were not energy efficient.
“Even in the UK, which is a temperate country, we know that many hospitals struggle when it comes to extreme heat,” he added. “Many of the buildings were designed before climate change.”
The healthcare sector accounts for 5% of global emissions worldwide, so needs to prioritise adaptation to become more resilient, the report concluded.
Members of the emergency military unit try to extinguish a wildfire in Ourense province, Spain, in August 2025. Photograph: Pablo Blázquez Domínguez/Getty Images
Responding to the recommendations, Dr Hans Kluge, the WHO’s regional director for Europe, said: “The conflicts in Ukraine and the Middle East have clearly shown what fossil fuel dependency really means – not just higher bills, but strained or broken health systems, disrupted food and fuel supplies and societies under pressure.
“The case for acting on climate now is not just environmental. It is a security argument, a health argument and an economic argument, all at once. And it is a moral imperative.”
Kluge added: “The decisions taken by governments today will determine the disease burden carried by people who are currently in primary school. It now falls to the rest of us to act on their recommendations and protect future generations. I commit to ensuring that climate change is treated as the health emergency it is across the 53 member states of the WHO European region.”
Johan Rockström, the director of the Potsdam Institute for Climate Impact Research, welcomed the report. He said: “The current state of the planet, where we are breaching multiple planetary boundaries, and which manifests itself as public health threats impacting millions of people across the world, provides ample scientific evidence that climate change should be declared a public health emergency of international concern.”
The report by Dr. Vivek Murthy cited a “profound risk of harm” to adolescent mental health and urged families to set limits and governments to set tougher standards for use.
Dr. Murthy testifying before the Senate Finance Committee on Capitol Hill on youth mental health in 2022. Credit: Susan Walsh/Associated Press
The nation’s top health official issued an extraordinary public warning on Tuesday about the risks of social media to young people, urging a push to fully understand the possible “harm to the mental health and well-being of children and adolescents.”
In a 19-page advisory, the United States surgeon general, Dr. Vivek Murthy, noted that the effects of social media on adolescent mental health were not fully understood, and that social media can be beneficial to some users. Nonetheless, he wrote, “There are ample indicators that social media can also have a profound risk of harm to the mental health and well-being of children and adolescents.”
The report included practical recommendations to help families guide children’s social media use. It recommended that families keep mealtimes and in-person gatherings free of devices to help build social bonds and promote conversation. It suggested creating a “family media plan” to set expectations for social media use, including boundaries around content and keeping personal information private.
Dr. Murthy also called on tech companies to enforce minimum age limits and to create default settings for children with high safety and privacy standards. And he urged the government to create age-appropriate health and safety standards for technology platforms.
Adolescents “are not just smaller adults,” Dr. Murthy said in an interview on Monday. “They’re in a different phase of development, and they’re in a critical phase of brain development.”
The report, effectively elevating long-simmering concerns around social media in the national conversation, came as state and federal lawmakers, many of them raised in an era when social media barely existed or didn’t exist at all, have been struggling with how to set limits on its use.
Montana’s governor recently signed a bill banning TikTok from operating in the state, prompting the Chinese-owned app to file a lawsuit and young TikTok users to lament what one called a “kick in the face.” In March, Utah became the first state to prohibit social media services from allowing users under 18 to have accounts without the explicit consent of a parent or guardian. That law could dramatically curtail young people’s access to apps like Instagram and Facebook.
Survey results from Pew Research have found that up to 95 percent of teens reported using at least one social media platform, while more than one-third said they used social media “almost constantly.” As social media use has risen, so have self-reports and clinical diagnoses among adolescents of anxiety and depression, along with emergency room visits for self-harm and suicidal ideation.
The report could help encourage further research to understand whether these two trends are related. It joins a growing number of calls for action around adolescents and social media. Earlier this month, the American Psychological Association issued its first-ever social media guidance, recommending that parents closely monitor teens’ usage and that tech companies reconsider features like endless scrolling and the “like” button.
A large body of research has emerged in recent years on the potential connection between social media use and soaring rates of distress among adolescents. But the results have been consistent only in their nuance and complexity.
An analysis published last year, examining research from 2019 to 2021 on social media use and mental health, found that “most reviews interpreted the associations between social media use and mental health as ‘weak’ or ‘inconsistent,’ whereas a few qualified the same associations as ‘substantial’ and ‘deleterious.’”
At their clearest, the data indicate that social media can have both a positive and negative impact on the well-being of young people, and that heavy use of social media — and screen time generally — appears to displace activities like sleep and exercise that are considered vital to developing brains.
On the positive side, social media can help many young people by giving them a forum to connect with others, find community and express themselves.
At the same time, the surgeon general’s advisory noted, social media platforms brim with “extreme, inappropriate and harmful content,” including content that “can normalize” self-harm, eating disorders and other self-destructive behavior. Cyberbullying is rampant.
Moreover, social media spaces can be fraught for young people especially, the advisory added: “In early adolescence, when identities and sense of self-worth are forming, brain development is especially susceptible to social pressures, peer opinions and peer comparison.”
The advisory noted that technology companies have a vested interest in keeping users online, and that they use tactics that entice people to engage in addictive-like behaviors. “Our children have become unknowing participants in a decades-long experiment,” the advisory states.
A spokesperson for Meta, the owner of Instagram and Facebook, said that the advisory included recommendations that “are reasonable and, in large part, Meta has already implemented.” Those measures include automatically making the accounts of people under 16 private when they join Instagram and limiting the types of content teens can see on the app.
TikTok did not immediately respond to requests for comment on Tuesday afternoon.
The advisory did not provide guidance on what a healthy use of social media might look like, nor did it condemn social-media use for all young people. Rather, it concluded, “We do not yet have enough evidence to determine if social media is sufficiently safe for children and adolescents.”
The surgeon general’s position lacks any real power beyond its potential as a bully pulpit, and Dr. Murthy’s advisory does not carry the force of law or policy. It was intended, the report said, to call Americans’ attention to “an urgent public health issue” and to make recommendations for how it should be addressed.
In the interview on Monday, Dr. Murthy acknowledged that the lack of clarity around social media was a heavy burden for users and families to bear.
“That’s a lot to ask of parents, to take a new technology that’s rapidly evolving and that fundamentally changes how kids perceive themselves,” Dr. Murthy said. “So we’ve got to do what we do in other areas where we have product safety issues, which is to set in place safety standards that parents can rely on, that are actually enforced.”
Remy Tumin contributed reporting.
Matt Richtel is a best-selling author and Pulitzer Prize-winning reporter based in San Francisco. He joined The Times in 2000, and his work has focused on science, technology, business and narrative-driven storytelling around these issues. @mrichtel
Catherine Pearson is a reporter for the Well section of The Times, covering families and relationships.
Michael Levenson joined The Times in December 2019. He was previously a reporter at The Boston Globe, where he covered local, state and national politics and news.
A version of this article appears in print on May 24, 2023, Section A, Page 1 of the New York edition with the headline: Advisory Says Teens Face Risk On Social Sites.
Climate change is already killing people, but countries don’t have an easy way to count those deaths. A new project might change that.
Climate change can kill people in all kinds of ways. There are the obvious ones—wildfires, storms, and floods—yet rising temperatures may also lead to the increased spread of deadly diseases, make food harder to come by, and increase the risk of conflict.
Although we know about these wide-ranging but equally terrifying risks, attempts to pinpoint the number of deaths caused by climate change have been piecemeal. One recent study estimated that climate change was to blame for 37 percent of heat-related deaths over the past three decades. In 2021, Daniel Bressler, a PhD student at Columbia University in New York, estimated that every additional 4,400 metric tons of carbon dioxide emitted will cause one heat-related death later this century. He called this number the “mortality cost of carbon.”
Putting a number on climate deaths isn’t just an academic exercise. People are already dying because of extreme temperature and weather events, and we can expect this to become more common as the planet continues to heat up. If governments want to put in place policies to prevent these deaths, they need a way of accurately measuring the deaths and ill health linked to warming. The search is on for the true mortality cost of carbon.
As part of this search, the UK government has made its first attempt at putting a number on climate change deaths. The UK Office for National Statistics (ONS)—an independent government agency responsible for producing official data—has for the first time reported climate-related deaths and hospital admissions in England and Wales. The report covers the years 2001 to 2020, but future reports will be released annually, revealing for the first time detailed information about the impact that climate change is having on health in the two nations. (Statistics for Scotland and Northern Ireland are recorded separately.)
The main finding from this investigation is counterintuitive. The report found that the number of deaths associated with warm or cold temperatures actually decreased between 2001 and 2020. On average, 27,755 fewer people were dying each year due to unusually warm or cold temperatures. In other words, climate change might have actually prevented over half a million deaths in England and Wales over this period. In 2001 there were 993 climate-related deaths per 100,000 people in England and Wales. By 2019 that figure had fallen to 771.
But let’s not get ahead of ourselves. There are a number of reasons why the net number of temperature-related deaths appeared to decline over this period, says Myer Glickman, head of the epidemiological, climate, and global health team at the ONS. For a start, statisticians took a relatively narrow definition of climate-related deaths. They only included deaths from conditions where scientists had previously found a clear link between temperature and disease outcome, and they also excluded any health condition where their own analysis showed no link between temperature and outcome. This means that the mortality data doesn’t include deaths from violence or natural forces (such as storms, landslides, or flooding).
The analysis also excluded deaths from air pollution, which Public Health England estimates is equivalent to between 28,000 and 36,000 deaths each year in the UK. Glickman says that there is no accepted way to separate out the effect that temperature increases have on air pollution. Add all these caveats together and it’s likely that the ONS analysis is a little on the conservative side.
Then there is the big reason why climate change has not led to more deaths in England and Wales: the very mild climate. Although average temperatures in the UK have increased by 0.9 degrees compared to the period from 1961 to 1990, its residents are not some of the 3 billion people who face unlivable conditions if greenhouse gas emissions increase rapidly. And while deaths linked to cold weather were down in England and Wales, on warmer days there was a net increase in hospital admissions linked to warmer weather. This was particularly true when it comes to injuries, which may be because more people do outdoor activities when it’s warmer or might be linked to the increases in violence and mental health problems that are associated with warmer temperatures.
The lower rate of deaths might also be a sign that our attempts to fight back against cold weather are working. Widespread flu vaccinations, support for people to pay their heating bills, and increases in home insulation mean that the coldest days didn’t hit as hard as they might have without these mitigations in place, Glickman says. And warmer homes might be a good thing now, but as summers in the UK get hotter and air-conditioning remains rare, it may start to become a problem.
The ONS will now release this data on a yearly basis, but Glickman’s next project is to look more closely at how temperature changes affected different areas. “We’re going to drill down to a local level temperature,” he says. “That’s going to give us a lot more resolution on what’s happening and who it’s happening to.” The impact of climate change might depend on how wealthy an area is, for example, or whether its residents have easy access to health care or community support.
Glickman also wants to explore indirect impacts of climate on health. “What will be a big interest in the coming years is the lower-level health impacts of things like flooding,” he says. If someone’s home is flooded, it might increase their vulnerability to respiratory disease or worsen their mental health. Researchers from the UK have already found that people with mental illnesses are more at risk of death during hot weather. We don’t know why that is exactly, but researchers think it might be because people with mental illnesses are more likely to be socially isolated or already have poorer health, which makes them more vulnerable when temperatures rise.
The team behind the ONS report are also part of a wider effort to create a global system to count climate-related health impacts. “What we don’t have is a robust set of statistics to categorize the impact of climate on health,” says Bilal Mateen, a senior manager of digital technology at Wellcome Trust, the health charity funding the new climate change health impact initiative.
The first year of the project will be spent identifying countries to partner with before developing and testing different ways of measuring climate change deaths that work for specific countries, says Mateen. The idea is to use this data to help countries devise policies that lessen the health impact of climate change. “We can begin to tease out what works, what doesn’t, and what adaptation and mitigation interventions we should be supporting,” Mateen says.
If it’s true that warmer homes and flu vaccines helped reduce climate change deaths in England and Wales, it’s a sign that populations that are healthier on the whole might be better at surviving the ravages of a heating world. Other countries may want to take note. “All policies are health policies,” says Mateen. “There is a clear need to support job stability, to address fuel poverty and every other policy that’s outside of the mandate of the health minister, because we know that those social determinants of health have downstream impact.”
Last summer, a doctor wrote “climate change” in his patient’s chart. But is medicine really ready to address systemic health impacts?
Last June, a heat dome settled over British Columbia, shattering the region’s heat records for five consecutive days and hitting temperatures of over 120 degrees. The dome was responsible for at least 500 human deaths (and potentially a billion marine creature casualties) and stretched the health systems in the region to their breaking point.
And at one rural hospital in Nelson, British Columbia, doctor Kyle Merritt began to feel like there was more he should do than simply treat all the patients coming in with heat stroke and exhaustion. “I was upset with what I was seeing,” he says, “I felt like it should be documented in some way.” So when a 70-year-old woman arrived with heat stroke, he wrote “climate change” in her medical chart as the underlying reason she had to be admitted to the hospital.
It was the first and only time Merritt chose to include “climate change” as an underlying condition in a patient’s chart. “It was the first patient that I felt like it was really clear cut,” he says. Had the conditions outside not been so extreme, he might have been able to discharge her and let her recover at home. When we spoke, Merritt emphasized that it was a decision he made in the heat of the moment. He never expected it to become national news.
Months later, when speaking with the founders of a small organization called Doctors for Planetary Health, Merritt shared the story of his decision to write “climate change” in the patient’s chart. When they asked to use that story in a press release accompanying a planned climate rally, Merritt didn’t think anyone was going to read the press release about this little thing that happened.
But read it they did. Eventually, Merritt’s story was all over the news, often under erroneous headlines claiming he had “diagnosed” a patient with climate change (the phrase appears in her chart as an underlying cause, not a diagnosis). The story was covered by national publications like NBC News, The Hill, The Daily Mail, along with a host of right-wing news sites like GOP USA.
Some praised the decision for bringing necessary awareness to the connection between climate change and health. “When I saw this, I thought, ‘Yes, this is what we need. We need more attention to the social determinants of health,’” says Keisha Ray, an assistant professor at the McGovern Center for Humanities and Ethics at UTHealth. Others claimed this was “the latest example of team-left lunacy.” Some columnists argued, incorrectly, that the patient probably didn’t get proper treatment because her doctor “diagnosed her” with something incurable. (Merritt admitted the patient to the emergency room and she was treated for her condition.)
When I read the story, my question was less about Merritt and more about the patient herself. Did she know she was the center of this news blip? Had he talked to her about climate change, or the fact that he was writing it in her chart? Did she give permission to be in the press release? And what are the ethics of turning a patient into a public point?
Doctors use case studies all the time to communicate with one another, and with the press. And for good reason: People connect with and remember stories far better than generalized facts. But using a patient to explain a concept, or to help educate doctors on how to treat someone more effectively, is different from using a patient’s story to make this broader, public point about climate and health. Even Merritt admitted that writing “climate change” in this woman’s chart didn’t do much to help her or other patients suffering during the heat dome. “It’s not like some other doctor was going to look at it and make sure they were never exposed to climate change,” he says. “Practically speaking, it doesn’t really do that much.”
Medicine has a checkered history when it comes to using patient stories and protecting privacy. For decades, doctors paraded patients in front of the public without their consent. In 1906, for example, a famous doctor named Wilfred Grenfell published the story of a 9-year-old boy who had accidentally shot himself in the knee. Grenfell used the boy’s full name, image, and identity, telling the tale with gusto each time he spoke to the public and his colleagues—even distorting the facts of the case, turning “slight” bleeding in the original chart into “shocking” bleeding and a “heterogeneous mass of bloody rags”—in order to entertain donors, make himself seem more heroic, and maintain his status as a celebrity doctor. Fast forward to today, and issues of patient privacy are still very present. In 2012 the ABC show NY Med, which at the time starred celebrity doctor Mehmet Oz, broadcast the death of a patient without his family’s consent. His widow won $2.2 million in a suit against the hospital.
Given that history, the question of how much to anonymize a patient in these tales is well-trod territory for medical ethicists. “As long as the physician doesn’t give any kind of identifying information, then it would be ethical. You want to always maintain the patient’s privacy,” says Ray. “But you also have to think about how minor information can be pieced together, where someone can figure out who this patient is.”
In Merritt’s case, the details provided to the press go like this: We know the patient’s age, her background medical conditions, the type of home she lives in, and that she was admitted in June. Kootenay Medical Center, where Merritt works, serves less than 4,000 patients. “That’s a lot of identifying information,” Ray said, when I told her the facts that had been publicly confirmed. “Small towns don’t tend to have a lot of physicians, so you could very well be one of three physicians.”
This feels increasingly important when a story is used in a way that might be construed as political —calling for action on something like racism or climate change. In a world where private citizens can be outed and harassed for being associated with a cause or a side, doctors who want to use a patient’s sickness to make an activist point might need to be a little more cautious. “I worry that the sensationalism of this story may encourage people like journalists to go seek this patient out,” says Ray. “And I also worry that because climate change is still very political and it still is considered a left-leaning idea, that it may encourage conservative media to go and find this person and pit them against each other.”
That hasn’t happened in this case. But Merritt says that if he were to do it over, he might have done things differently. As it unfolded, he didn’t tell the patient he was writing “climate change” in her chart. In fact, they didn’t discuss climate change at all. “If I had known when I had written that in the chart that it was something that I was doing to try and tell the story, I don’t know. I may have talked to the patient more about it and asked their permission,” he says. “But of course, at that time when I did it, I had no idea that it would ever become a story of any kind.” To this day, Merritt believes that the patient has no idea she is the one in the story.
Beyond the specifics of Merritt and his patient, the story raises big questions about how medicine can and should handle systemic impacts on health.
Merritt wrote “climate change” in a bout of frustration, wanting to document what he was seeing in real time. Other doctors have taken different approaches. Nyasha Spears, a physician at St. Luke’s Hospital in Duluth, Minnesota, takes nearly the opposite tack that Merritt did—rather than quietly writing in a chart to make a broader point, she talks to her patients constantly about climate change and the environment. “As a family doctor, my jam is habit change. This is what I do,” she says. “So my thought with climate change is, can I start peppering my conversations with patients all the time with an argument that habit change is good for them on a personal level, but also good for the environment?”
In the case of Merritt’s patient, this talk might not have done much. There was nothing she could do about her conditions, no habit change she could make to avoid the scorching heat. Like many in her community, she likely couldn’t afford to install air-conditioning in her trailer, and beyond that there was little to be done. In cases like these, Ray says that maybe a climate change talk isn’t warranted. “They can feel helpless because there’s nothing that they can do,” she says. “They are literally living, and just living is making them sick.”
This reality can make things feel bleak for both doctors and patients. And to address these connections between health and structural conditions like climate change and racism, doctors will need to ask not simply what they can do for each individual patient, but also what they can change about medicine to account for and reckon with these links. Today, there is no diagnostic code for climate change, no way to link these cases up or track them in any way, but perhaps there should be.
“There’s all sorts of ICD-10 codes that are completely inane,” says Spears. “If you ever want to entertain yourself, you just start looking at ICD 10 codes. ‘Fall from a spacecraft’ is one. And so it would make perfect sense that there would be an ICD-10 code for climate change illness.” Being able to track these additional, systemic determinants of health could make it easier to prove the links, and do something about them.
Having more data doesn’t always mean making change—the impact that race and income have on health have been well proven for years, but still haven’t adequately been addressed. And Ray says that adding these codes shouldn’t stop with climate. “If you live in a poor area, then you are likely living with more environmental impacts. Are we going to start now having a code for low income? Is there going to be a code for: You don’t have enough money to live in a safe home and so you are experiencing environmental toxins? Is improper housing also going to be coded? So I just wonder how far we are willing to take it.”
This might be the silver lining in the story of Merritt’s patient. When we spoke, he told me he had recently gotten an email from Health Canada, asking to talk to him about creating a diagnostic code for climate change that doctors could use to track these impacts.
Writing “climate change” in one patient’s chart isn’t going to save the world, or even a single life—Merritt is the first to admit that—but it can start a conversation about how much the medical system is willing to adapt to the threats that its patients truly face. “I’ve learned a lot about how big of an impact a story can make,” he says.
Manaus Na aldeia Maimasi, em Roraima, uma criança yanomami jaz sobre a rede. Com as costelas expostas pela desnutrição, ela foi diagnosticada com malária e verminose. Mas a primeira equipe médica no local em seis meses não dispunha de medicamentos suficientes para tratar toda a aldeia.
A foto dessa criança e a história por trás dela foram obtidas pelo missionário católico Carlo Zacquini, 84, que atua entre os yanomamis desde 1968. Ele é cofundador da Comissão pela Criação do Parque Yanomami (CCPY), que deu visibilidade aos problemas causados pelos brancos, promoveu atendimento em saúde e lutou pela demarcação, concluída em 1992.
O território yanomami sofre com o aumento da malária e com a desnutrição infantil crônica, que atinge 80% das crianças até 5 anos, segundo estudo recente financiado pela Unicef e realizado em parceria com a Fiocruz e o Ministério da Saúde.
Os indígenas também enfrentam uma grande invasão de garimpeiros, incentivados por promessas do presidente Jair Bolsonaro de legalizá-los e pelo alto preço do minério. São cerca de 20 mil não indígenas morando ilegalmente na Terra Indígena Yanomami, contaminando os rios com mercúrio e contribuindo para espalhar Covid-19 e malária, além do álcool e da prostituição.
Procurado, o Distrito Sanitário Especial Indígena (Dsei) Yanomami, do Ministério da Saúde, informou que a criança, do sexo feminino, foi transferida a Boa Vista (RR) dois dias após a visita médica, acompanhada dos pais e dos irmãos.
Ela tem 8 anos e pesa 12,5 kg. Internada desde 23 de abril, está em tratamento para pneumonia, anemia e desnutrição grave —a malária foi curada. Ela está estável e em acompanhamento pelo serviço social. Segundo o órgão, trata-se de um caso isolado.
O Dsei negou a escassez de medicamentos e afirma que a quantidade é definida de acordo com a demanda prevista pela semana epidemiológica. O órgão não informou sobre como está o tratamento de outros yanomamis doentes na mesma região, mas alega que o atendimento de saúde é dificultado pelo fluxo constante dos indígenas e atribuiu a alta de incidência de malária à presença do garimpo ilegal.
A seguir, o depoimento de Zacquini:
É uma criança da aldeia Maimasi, a dois dias a pé da Missão Catrimani. Ela está sem assistência há muito tempo, com malária e verminose.
A fotografia foi feita por volta de 17 de abril. O pessoal das equipes de saúde tem receio de denunciar essa situação, pois podem ser punidos, colocados em lugares mais penosos ou ser demitidos. Vários polos de saúde estão abandonados. Não há estoque de medicamentos para verminose na sede do Dsei (Distrito Sanitário Especial Indígena Yanomami), em Boa Vista. Até para malária a quantidade é limitada.
O posto de saúde tem muita dificuldade para conseguir medicamentos. Faltam profissionais para revezamento e falta gasolina para deslocamento. Há três meses, eles usam a canoa com rabeta [motor] dos próprios yanomamis.
Com quadro de verminose e malária, criança yanomami dorme em rede na aldeia Maimasi, perto da Missão Catrimani, na Terra Indígena Yanomami, em Roraima – Divulgação
Para chegar a Maimasi, seriam oito minutos de helicóptero, mas, a princípio, isso só ocorre em casos de emergência. Evidentemente, essa criança é um caso de emergência!
Para levar medicamento ao pólo-base, foram deslocados um avião com uma equipe médica, porém eles ficaram aguardando inutilmente a chegada do helicóptero.
Havia seis meses que ninguém visitava a aldeia. Dessa vez, foram medicamentos para malária, mas não deu para repetir a dose. Uma equipe da Sesai (Secretaria Especial de Saúde Indígena, do Ministério da Saúde), incluindo médico, foi de avião até a Missão Catrimani para levar esses medicamentos.
O pessoal da saúde faz tratamentos com medicamentos, mas o tratamento não tem continuidade quando trocam de equipe. Assim, quando possível, fazem a primeira dose de tratamento, mas depois de um tempo os doentes devem recomeçar a partir da primeira dose.
Estou revoltado e com o sangue fervendo. É uma situação que parece estar se generalizando na Terra Indígena Yanomami.
O vaivém de garimpeiros é contínuo e isso implica voos de avião, barcos, helicópteros e a pé. São milhares os invasores da Terra Indígena Yanomami, e o presidente da República anuncia que irá pessoalmente falar com os militares que estão ali e com os garimpeiros também. Faz questão de dizer que não vai prender estes últimos, mas somente conversar.
Até para malária os medicamentos são contados, incluindo a cloroquina. Tem cloroquina para Covid, mas não para malária. A criança desnutrida está numa aldeia a oito minutos de helicóptero de um posto de saúde, mas leva um dia a pé. E depois dessa aldeia há outras, que na época estavam reunidas para o cerimonial funerário em outra aldeia mais afastada.
A equipe do pólo-base se deslocou a pé para a aldeia e encontrou um grupo grande de yanomamis que fazia um ritual funerário para uma criança que tinha morrido sem assistência. Eles ministraram medicamentos para verminose a todos, mas esse medicamento acabou e não puderam dar uma outra dose, o que é a praxe.
Aliás, havia mais de um ano que aquelas aldeias não recebiam atendimento contra verminose. A criança da foto e outros 16 indígenas presentes estavam com malária, a maioria deles com falciparum, a variedade mais agressiva. Os demais 84 estavam todos com sintomas de gripe e de febre.
Summary: A new study finds that China’s countrywide ban on traffic mobility from February 10 to March 14, 2020 greatly limited automobile emissions and sharply reduced the country’s often severe air pollution. The improved air quality, in turn, prevented thousands of pollution-related deaths.
Soon after coronavirus appeared, an all-encompassing quarantine put into effect by the Chinese government slowed the spread of the disease and saved lives, but the quarantine also produced another unanticipated health benefit.
A new study led by researchers at the Yale School of Public Health and published in the journal Lancet Planetary Health, finds that China’s countrywide ban on traffic mobility from February 10 to March 14 greatly limited automobile emissions and sharply reduced the country’s often severe air pollution.
The improved air quality, in turn, prevented thousands of pollution-related deaths. More premature deaths were avoided by cleaner air — an estimated 12,125 — than lives lost from the pandemic — 4,633 as of May 4, the study finds.
“This is a very surprising result. The pandemic continues to be a terrible thing for China and the rest of the world, but the decrease in emissions that accompanied it has actually conferred some positive health results,” said Kai Chen, assistant professor at the Yale School of Public Health and the study’s first author. “The question is, how can we have one without the other?”
Although the findings cannot be directly applied to other countries due to different severity of and responses to COVID-19, as well as differing air pollution levels and population characteristics, reduced air pollution levels have been detected in other Asian and European countries and the U.S. after their own lockdowns, Chen said. He notes that this reduction in pollution has likely conferred similar health benefits.
The study found that ground-level air pollution levels dropped remarkably throughout China, with nitrogen dioxide (NO2) dropping by 12.9 ?g/m3 (or 37% compared with before the quarantine period) and fine particulate matter (PM2.5) dropping by 18.9 ?g/m3 (30%) across 367 Chinese cities. The decline in NO2 across China during the quarantine period was so dramatic that it was detected by satellite measurements.
NO2 is a gaseous air pollutant, which is mainly produced from fuel burning in vehicles and power plants. NO2 level before the quarantine (January 5 to 20) was as high as 40.5 ?g/m3 in Wuhan, where the outbreak began in China. During the quarantine (February 10 to March 14), those levels had fallen to 18.8 ?g/m3 (micrograms per cubic meter).
Particulate matter includes all solid and liquid particles suspended in air, many of which are hazardous when inhaled. This mixture includes both organic and inorganic particles, such as dust, pollen, soot, smoke, and liquid droplets. Before the quarantine, PM 2.5 (fine inhalable particles with diameters of 2.5 micrometers or smaller) levels were measured at 62.5 ?g/m3 in many Chinese cities. During the quarantine, the fine particulate matter reading has been 36.5 ?g/m3 in those same locations.
The authors then calculated the number of avoided deaths attributable to these decreases in NO2 and PM2.5 across China based on the short-term association between these pollutants and daily mortality using data from a previous epidemiological study of 272 Chinese cities, and mortality data from the China Health and Family Planning Statistical Yearbook 2018. The authors found that among the more than 12,000 avoided deaths, about two-thirds were from avoided cardiovascular diseases (hypertensive disease, coronary heart disease and stroke) and chronic obstructive pulmonary disease.
The findings illustrate the substantial human health benefits related to cardiovascular disease morbidity and mortality that can be achieved when aggressive air pollution control measures are put in place to reduce emissions from vehicles, such as through climate mitigation-related traffic restrictions or efforts to accelerate the transition to electric vehicles, the authors said.
“This unexpected health benefit suggests that if we were to address the climate crisis as aggressively as we are combating the COVID-19 pandemic with strong political will and urgent action, we could prevent the enormous health burdens associated with climate change,” said co-author Paul T. Anastas, professor at the Yale School of Public Health and the Teresa and H. John Heinz III Chair of Chemistry for the Environment.
The authors said that they want to further identify whether climate or weather-related factors and air pollution could influence population susceptibility to COVID-19.
The paper was written with researchers from the University at Buffalo School of Public Health and Health Professions and Boston University School of Public Health.
Kai Chen, Meng Wang, Conghong Huang, Patrick L Kinney, Paul T Anastas. Air pollution reduction and mortality benefit during the COVID-19 outbreak in China. The Lancet Planetary Health, 2020; DOI: 10.1016/S2542-5196(20)30107-8
Summary of the article: Strong coronavirus measures today should only last a few weeks, there shouldn’t be a big peak of infections afterwards, and it can all be done for a reasonable cost to society, saving millions of lives along the way. If we don’t take these measures, tens of millions will be infected, many will die, along with anybody else that requires intensive care, because the healthcare system will have collapsed.
Within a week, countries around the world have gone from: “This coronavirus thing is not a big deal” to declaring the state of emergency. Yet many countries are still not doing much. Why?
Every country is asking the same question: How should we respond? The answer is not obvious to them.
Some countries, like France, Spain or Philippines, have since ordered heavy lockdowns. Others, like the US, UK, or Switzerland, have dragged their feet, hesitantly venturing into social distancing measures.
Here’s what we’re going to cover today, again with lots of charts, data and models with plenty of sources:
What’s the current situation?
What options do we have?
What’s the one thing that matters now: Time
What does a good coronavirus strategy look like?
How should we think about the economic and social impacts?
When you’re done reading the article, this is what you’ll take away:
Our healthcare system is already collapsing. Countries have two options: either they fight it hard now, or they will suffer a massive epidemic. If they choose the epidemic, hundreds of thousands will die. In some countries, millions. And that might not even eliminate further waves of infections. If we fight hard now, we will curb the deaths. We will relieve our healthcare system. We will prepare better. We will learn. The world has never learned as fast about anything, ever. And we need it, because we know so little about this virus. All of this will achieve something critical: Buy Us Time.
If we choose to fight hard, the fight will be sudden, then gradual. We will be locked in for weeks, not months. Then, we will get more and more freedoms back. It might not be back to normal immediately. But it will be close, and eventually back to normal. And we can do all that while considering the rest of the economy too.
Ok, let’s do this.
1. What’s the situation?
Last week, I showed this curve:
It showed coronavirus cases across the world outside of China. We could only discern Italy, Iran and South Korea. So I had to zoom in on the bottom right corner to see the emerging countries. My entire point is that they would soon be joining these 3 cases.
Let’s see what has happened since.
As predicted, the number of cases has exploded in dozens of countries. Here, I was forced to show only countries with over 1,000 cases. A few things to note:
Spain, Germany, France and the US all have more cases than Italy when it ordered the lockdown
An additional 16 countries have more cases today than Hubei when it went under lockdown: Japan, Malaysia, Canada, Portugal, Australia, Czechia, Brazil and Qatar have more than Hubei but below 1,000 cases. Switzerland, Sweden, Norway, Austria, Belgium, Netherlands and Denmark all have above 1,000 cases.
Do you notice something weird about this list of countries? Outside of China and Iran, which have suffered massive, undeniable outbreaks, and Brazil and Malaysia, every single country in this list is among the wealthiest in the world.
Do you think this virus targets rich countries? Or is it more likely that rich countries are better able to identify the virus?
It’s unlikely that poorer countries aren’t touched. Warm and humid weather probablyhelps, but doesn’t prevent an outbreak by itself — otherwise Singapore, Malaysia or Brazil wouldn’t be suffering outbreaks.
The most likely interpretations are that the coronavirus either took longer to reach these countries because they’re less connected, or it’s already there but these countries haven’t been able to invest enough on testing to know.
Either way, if this is true, it means that most countries won’t escape the coronavirus. It’s a matter of time before they see outbreaks and need to take measures.
What measures can different countries take?
2. What Are Our Options?
Since the article last week, the conversation has changed and many countries have taken measures. Here are some of the most illustrative examples:
Measures in Spain and France
In one extreme, we have Spain and France. This is the timeline of measures for Spain:
On Thursday, 3/12, the President dismissed suggestions that the Spanish authorities had been underestimating the health threat. On Friday, they declared the State of Emergency. On Saturday, measures were taken:
People can’t leave home except for key reasons: groceries, work, pharmacy, hospital, bank or insurance company (extreme justification)
Specific ban on taking kids out for a walk or seeing friends or family (except to take care of people who need help, but with hygiene and physical distance measures)
All bars and restaurants closed. Only take-home acceptable.
All entertainment closed: sports, movies, museums, municipal celebrations…
Weddings can’t have guests. Funerals can’t have more than a handful of people.
Mass transit remains open
On Monday, land borders were shut.
Some people see this as a great list of measures. Others put their hands up in the air and cry of despair. This difference is what this article will try to reconcile.
France’s timeline of measures is similar, except they took more time to apply them, and they are more aggressive now. For example, rent, taxes and utilities are suspended for small businesses.
Measures in the US and UK
The US and UK, like countries such as Switzerland, have dragged their feet in implementing measures. Here’s the timeline for the US:
Wednesday 3/11: travel ban.
Friday: National Emergency declared. No social distancing measures
Monday: the government urges the public to avoid restaurants or bars and attend events with more than 10 people. No social distancing measure is actually enforceable. It’s just a suggestion.
Lots of states and cities are taking the initiative and mandating much stricter measures.
The UK has seen a similar set of measures: lots of recommendations, but very few mandates.
These two groups of countries illustrate the two extreme approaches to fight the coronavirus: mitigation and suppression. Let’s understand what they mean.
Option 1: Do Nothing
Before we do that, let’s see what doing nothing would entail for a country like the US:
This fantastic epidemic calculator can help you understand what will happen under different scenarios. I’ve pasted below the graph the key factors that determine the behavior of the virus. Note that infected, in pink, peak in the tens of millions at a certain date. Most variables have been kept from the default. The only material changes are R from 2.2 to 2.4 (corresponds better to currently available information. See at the bottom of the epidemic calculator), fatality rate (4% due to healthcare system collapse. See details below or in the previous article), length of hospital stay (down from 20 to 10 days) and hospitalization rate (down from 20% to 14% based on severe and critical cases. Note the WHO calls out a 20% rate) based on our most recently available gathering of research. Note that these numbers don’t change results much. The only change that matters is the fatality rate.
If we do nothing: Everybody gets infected, the healthcare system gets overwhelmed, the mortality explodes, and ~10 million people die (blue bars). For the back-of-the-envelope numbers: if ~75% of Americans get infected and 4% die, that’s 10 million deaths, or around 25 times the number of US deaths in World War II.
You might wonder: “That sounds like a lot. I’ve heard much less than that!”
So what’s the catch? With all these numbers, it’s easy to get confused. But there’s only two numbers that matter: What share of people will catch the virus and fall sick, and what share of them will die. If only 25% are sick (because the others have the virus but don’t have symptoms so aren’t counted as cases), and the fatality rate is 0.6% instead of 4%, you end up with 500k deaths in the US.
If we don’t do anything, the number of deaths from the coronavirus will probably land between these two numbers. The chasm between these extremes is mostly driven by the fatality rate, so understanding it better is crucial. What really causes the coronavirus deaths?
How Should We Think about the Fatality Rate?
This is the same graph as before, but now looking at hospitalized people instead of infected and dead:
The light blue area is the number of people who would need to go to the hospital, and the darker blue represents those who need to go to the intensive care unit (ICU). You can see that number would peak at above 3 million.
Now compare that to the number of ICU beds we have in the US (50k today, we could double that repurposing other space). That’s the red dotted line.
No, that’s not an error.
That red dotted line is the capacity we have of ICU beds. Everyone above that line would be in critical condition but wouldn’t be able to access the care they need, and would likely die.
This is why people died in droves in Hubei and are now dying in droves in Italy and Iran. The Hubei fatality rate ended up better than it could have been because they built 2 hospitals nearly overnight. Italy and Iran can’t do the same; few, if any, other countries can. We’ll see what ends up happening there.
So why is the fatality rate close to 4%?
If 5% of your cases require intensive care and you can’t provide it, most of those people die. As simple as that.
These numbers only show people dying from coronavirus. But what happens if all your healthcare system is collapsed by coronavirus patients? Others also die from other ailments.
What happens if you have a heart attack but the ambulance takes 50 minutes to come instead of 8 (too many coronavirus cases) and once you arrive, there’s no ICU and no doctor available? You die.
There are 4 million admissions to the ICU in the US every year, and 500k (~13%) of them die. Without ICU beds, that share would likely go much closer to 80%. Even if only 50% died, in a year-long epidemic you go from 500k deaths a year to 2M, so you’re adding 1.5M deaths, just with collateral damage.
If the coronavirus is left to spread, the US healthcare system will collapse, and the deaths will be in the millions, maybe more than 10 million.
The same thinking is true for most countries. The number of ICU beds and ventilators and healthcare workers are usually similar to the US or lower in most countries. Unbridled coronavirus means healthcare system collapse, and that means mass death.
Unbridled coronavirus means healthcare systems collapse, and that means mass death.
By now, I hope it’s pretty clear we should act. The two options that we have are mitigation and suppression. Both of them propose to “flatten the curve”, but they go about it very differently.
Option 2: Mitigation Strategy
Mitigation goes like this: “It’s impossible to prevent the coronavirus now, so let’s just have it run its course, while trying to reduce the peak of infections. Let’s just flatten the curve a little bit to make it more manageable for the healthcare system.”
This chart appears in a very important paper published over the weekend from the Imperial College London. Apparently, it pushed the UK and US governments to change course.
It’s a very similar graph as the previous one. Not the same, but conceptually equivalent. Here, the “Do Nothing” situation is the black curve. Each one of the other curves are what would happen if we implemented tougher and tougher social distancing measures. The blue one shows the toughest social distancing measures: isolating infected people, quarantining people who might be infected, and secluding old people. This blue line is broadly the current UK coronavirus strategy, although for now they’re just suggesting it, not mandating it.
Here, again, the red line is the capacity for ICUs, this time in the UK. Again, that line is very close to the bottom. All that area of the curve on top of that red line represents coronavirus patients who would mostly die because of the lack of ICU resources.
Not only that, but by flattening the curve, the ICUs will collapse for months, increasing collateral damage.
You should be shocked. When you hear: “We’re going to do some mitigation” what they’re really saying is: “We will knowingly overwhelm the healthcare system, driving the fatality rate up by a factor of 10x at least.”
You would imagine this is bad enough. But we’re not done yet. Because one of the key assumptions of this strategy is what’s called “Herd Immunity”.
Herd Immunity and Virus Mutation
The idea is that all the people who are infected and then recover are now immune to the virus. This is at the core of this strategy: “Look, I know it’s going to be hard for some time, but once we’re done and a few million people die, the rest of us will be immune to it, so this virus will stop spreading and we’ll say goodbye to the coronavirus. Better do it at once and be done with it, because our alternative is to do social distancing for up to a year and risk having this peak happen later anyways.”
Except this assumes one thing: the virus doesn’t change too much. If it doesn’t change much, then lots of people do get immunity, and at some point the epidemic dies down
How likely is this virus to mutate? It seems it already has.
This graph represents the different mutations of the virus. You can see that the initial strains started in purple in China and then spread. Each time you see a branching on the left graph, that is a mutation leading to a slightly different variant of the virus.
This should not be surprising: RNA-based viruses like the coronavirus or the flu tend to mutate around 100 times faster than DNA-based ones—although the coronavirus mutates more slowly than influenza viruses.
Not only that, but the best way for this virus to mutate is to have millions of opportunities to do so, which is exactly what a mitigation strategy would provide: hundreds of millions of people infected.
That’s why you have to get a flu shot every year. Because there are so many flu strains, with new ones always evolving, the flu shot can never protect against all strains.
Put in another way: the mitigation strategy not only assumes millions of deaths for a country like the US or the UK. It also gambles on the fact that the virus won’t mutate too much — which we know it does. And it will give it the opportunity to mutate. So once we’re done with a few million deaths, we could be ready for a few million more — every year. This corona virus could become a recurring fact of life, like the flu, but many times deadlier.
The best way for this virus to mutate is to have millions of opportunities to do so, which is exactly what a mitigation strategy would provide.
So if neither doing nothing and mitigation will work, what’s the alternative? It’s called suppression.
Option 3: Suppression Strategy
The Mitigation Strategy doesn’t try to contain the epidemic, just flatten the curve a bit. Meanwhile, the Suppression Strategy tries to apply heavy measures to quickly get the epidemic under control. Specifically:
Go hard right now. Order heavy social distancing. Get this thing under control.
Then, release the measures, so that people can gradually get back their freedoms and something approaching normal social and economic life can resume.
What does that look like?
All the model parameters are the same, except that there is an intervention around now to reduce the transmission rate to R=0.62, and because the healthcare system isn’t collapsed, the fatality rate goes down to 0.6%. I defined “around now” as having ~32,000 cases when implementing the measures (3x the official number as of today, 3/19). Note that this is not too sensitive to the R chosen. An R of 0.98 for example shows 15,000 deaths. Five times more than with an R of 0.62, but still tens of thousands of deaths and not millions. It’s also not too sensitive to the fatality rate: if it’s 0.7% instead of 0.6%, the death toll goes from 15,000 to 17,000. It’s the combination of a higher R, a higher fatality rate, and a delay in taking measures that explodes the number of fatalities. That’s why we need to take measures to reduce R today. For clarification, the famous R0 is R at the beginning (R at time 0). It’s the transmission rate when nobody is immune yet and there are no measures against it taken. R is the overall transmission rate.
Under a suppression strategy, after the first wave is done, the death toll is in the thousands, and not in the millions.
Why? Because not only do we cut the exponential growth of cases. We also cut the fatality rate since the healthcare system is not completely overwhelmed. Here, I used a fatality rate of 0.9%, around what we’re seeing in South Korea today, which has been most effective at following Suppression Strategy.
Said like this, it sounds like a no-brainer. Everybody should follow the Suppression Strategy.
So why do some governments hesitate?
They fear three things:
This first lockdown will last for months, which seems unacceptable for many people.
A months-long lockdown would destroy the economy.
It wouldn’t even solve the problem, because we would be just postponing the epidemic: later on, once we release the social distancing measures, people will still get infected in the millions and die.
Here is how the Imperial College team modeled suppressions. The green and yellow lines are different scenarios of Suppression. You can see that doesn’t look good: We still get huge peaks, so why bother?
We’ll get to these questions in a moment, but there’s something more important before.
This is completely missing the point.
Presented like these, the two options of Mitigation and Suppression, side by side, don’t look very appealing. Either a lot of people die soon and we don’t hurt the economy today, or we hurt the economy today, just to postpone the deaths.
This ignores the value of time.
3. The Value of Time
In our previous post, we explained the value of time in saving lives. Every day, every hour we waited to take measures, this exponential threat continued spreading. We saw how a single day could reduce the total cases by 40% and the death toll by even more.
But time is even more valuable than that.
We’re about to face the biggest wave of pressure on the healthcare system ever seen in history. We are completely unprepared, facing an enemy we don’t know. That is not a good position for war.
What if you were about to face your worst enemy, of which you knew very little, and you had two options: Either you run towards it, or you escape to buy yourself a bit of time to prepare. Which one would you choose?
This is what we need to do today. The world has awakened. Every single day we delay the coronavirus, we can get better prepared. The next sections detail what that time would buy us:
Lower the Number of Cases
With effective suppression, the number of true cases would plummet overnight, as we saw in Hubei last week.
As of today, there are 0 daily new cases of coronavirus in the entire 60 million-big region of Hubei.
The diagnostics would keep going up for a couple of weeks, but then they would start going down. With fewer cases, the fatality rate starts dropping too. And the collateral damage is also reduced: fewer people would die from non-coronavirus-related causes because the healthcare system is simply overwhelmed.
Suppression would get us:
Fewer total cases of Coronavirus
Immediate relief for the healthcare system and the humans who run it
Reduction in fatality rate
Reduction in collateral damage
Ability for infected, isolated and quarantined healthcare workers to get better and back to work. In Italy, healthcare workers represent 8% of all contagions.
Understand the True Problem: Testing and Tracing
Right now, the UK and the US have no idea about their true cases. We don’t know how many there are. We just know the official number is not right, and the true one is in the tens of thousands of cases. This has happened because we’re not testing, and we’re not tracing.
With a few more weeks, we could get our testing situation in order, and start testing everybody. With that information, we would finally know the true extent of the problem, where we need to be more aggressive, and what communities are safe to be released from a lockdown.
We could also set up a tracing operation like the ones they have in China or other East Asia countries, where they can identify all the people that every sick person met, and can put them in quarantine. This would give us a ton of intelligence to release later on our social distancing measures: if we know where the virus is, we can target these places only. This is not rocket science: it’s the basics of how East Asia Countries have been able to control this outbreak without the kind of draconian social distancing that is increasingly essential in other countries.
The measures from this section (testing and tracing) single-handedly curbed the growth of the coronavirus in South Korea and got the epidemic under control, without a strong imposition of social distancing measures.
Build Up Capacity
The US (and presumably the UK) are about to go to war without armor.
We have masks for just two weeks, few personal protective equipments (“PPE”), not enough ventilators, not enough ICU beds, not enough ECMOs (blood oxygenation machines)… This is why the fatality rate would be so high in a mitigation strategy.
But if we buy ourselves some time, we can turn this around:
We have more time to buy equipment we will need for a future wave
We can quickly build up our production of masks, PPEs, ventilators, ECMOs, and any other critical device to reduce fatality rate.
Put in another way: we don’t need years to get our armor, we need weeks. Let’s do everything we can to get our production humming now. Countries are mobilized. People are being inventive, such as using 3D printing for ventilator parts. We can do it. We just need more time. Would you wait a few weeks to get yourself some armor before facing a mortal enemy?
This is not the only capacity we need. We will need health workers as soon as possible. Where will we get them? We need to train people to assist nurses, and we need to get medical workers out of retirement. Many countries have already started, but this takes time. We can do this in a few weeks, but not if everything collapses.
Lower Public Contagiousness
The public is scared. The coronavirus is new. There’s so much we don’t know how to do yet! People haven’t learned to stop hand-shaking. They still hug. They don’t open doors with their elbow. They don’t wash their hands after touching a door knob. They don’t disinfect tables before sitting.
Once we have enough masks, we can use them outside of the healthcare system too. Right now, it’s better to keep them for healthcare workers. But if they weren’t scarce, people should wear them in their daily lives, making it less likely that they infect other people when sick, and with proper training also reducing the likelihood that the wearers get infected. (In the meantime, wearing something is better than nothing.)
All of these are pretty cheap ways to reduce the transmission rate. The less this virus propagates, the fewer measures we’ll need in the future to contain it. But we need time to educate people on all these measures and equip them.
Understand the Virus
We know very very little about the virus. But every week, hundreds of new papers are coming.
The world is finally united against a common enemy. Researchers around the globe are mobilizing to understand this virus better.
How does the virus spread? How can contagion be slowed down? What is the share of asymptomatic carriers? Are they contagious? How much? What are good treatments? How long does it survive? On what surfaces? How do different social distancing measures impact the transmission rate? What’s their cost? What are tracing best practices? How reliable are our tests?
Clear answers to these questions will help make our response as targeted as possible while minimizing collateral economic and social damage. And they will come in weeks, not years.
Find Treatments
Not only that, but what if we found a treatment in the next few weeks? Any day we buy gets us closer to that. Right now, there are already several candidates, such as Favipiravir, Chloroquine, or Chloroquine combined with Azithromycin. What if it turned out that in two months we discovered a treatment for the coronavirus? How stupid would we look if we already had millions of deaths following a mitigation strategy?
Understand the Cost-Benefits
All of the factors above can help us save millions of lives. That should be enough. Unfortunately, politicians can’t only think about the lives of the infected. They must think about all the population, and heavy social distancing measures have an impact on others.
Right now we have no idea how different social distancing measures reduce transmission. We also have no clue what their economic and social costs are.
Isn’t it a bit difficult to decide what measures we need for the long term if we don’t know their cost or benefit?
A few weeks would give us enough time to start studying them, understand them, prioritize them, and decide which ones to follow.
Fewer cases, more understanding of the problem, building up assets, understanding the virus, understanding the cost-benefit of different measures, educating the public… These are some core tools to fight the virus, and we just need a few weeks to develop many of them. Wouldn’t it be dumb to commit to a strategy that throws us instead, unprepared, into the jaws of our enemy?
4. The Hammer and the Dance
Now we know that the Mitigation Strategy is probably a terrible choice, and that the Suppression Strategy has a massive short-term advantage.
But people have rightful concerns about this strategy:
How long will it actually last?
How expensive will it be?
Will there be a second peak as big as if we didn’t do anything?
Here, we’re going to look at what a true Suppression Strategy would look like. We can call it the Hammer and the Dance.
The Hammer
First, you act quickly and aggressively. For all the reasons we mentioned above, given the value of time, we want to quench this thing as soon as possible.
One of the most important questions is: How long will this last?
The fear that everybody has is that we will be locked inside our homes for months at a time, with the ensuing economic disaster and mental breakdowns. This idea was unfortunately entertained in the famous Imperial College paper:
Do you remember this chart? The light blue area that goes from end of March to end of August is the period that the paper recommends as the Hammer, the initial suppression that includes heavy social distancing.
If you’re a politician and you see that one option is to let hundreds of thousands or millions of people die with a mitigation strategy and the other is to stop the economy for five months before going through the same peak of cases and deaths, these don’t sound like compelling options.
But this doesn’t need to be so. This paper, driving policy today, has been brutally criticized for core flaws: They ignore contact tracing (at the core of policies in South Korea, China or Singapore among others) or travel restrictions (critical in China), ignore the impact of big crowds…
The time needed for the Hammer is weeks, not months.
This graph shows the new cases in the entire Hubei region (60 million people) every day since 1/23. Within 2 weeks, the country was starting to get back to work. Within ~5 weeks it was completely under control. And within 7 weeks the new diagnostics was just a trickle. Let’s remember this was the worst region in China.
Remember again that these are the orange bars. The grey bars, the true cases, had plummeted much earlier (see Chart 9).
The measures they took were pretty similar to the ones taken in Italy, Spain or France: isolations, quarantines, people had to stay at home unless there was an emergency or had to buy food, contact tracing, testing, more hospital beds, travel bans…
Details matter, however.
China’s measures were stronger. For example, people were limited to one person per household allowed to leave home every three days to buy food. Also, their enforcement was severe. It is likely that this severity stopped the epidemic faster.
In Italy, France and Spain, measures were not as drastic, and their implementation is not as tough. People still walk on the streets, many without masks. This is likely to result in a slower Hammer: more time to fully control the epidemic.
Some people interpret this as “Democracies will never be able to replicate this reduction in cases”. That’s wrong.
For several weeks, South Korea had the worst epidemic outside of China. Now, it’s largely under control. And they did it without asking people to stay home. They achieved it mostly with very aggressive testing, contact tracing, and enforced quarantines and isolations.
The following table gives a good sense of what measures different countries have followed, and how that has impacted them (this is a work-in-progress. Feedback welcome.)
This shows how countries who were prepared, with stronger epidemiological authority, education on hygiene and social distancing, and early detection and isolation, didn’t have to pay with heavier measures afterwards.
Conversely, countries like Italy, Spain or France weren’t doing these well, and had to then apply the Hammer with the hard measures at the bottom to catch up.
The lack of measures in the US and UK is in stark contrast, especially in the US. These countries are still not doing what allowed Singapore, South Korea or Taiwan to control the virus, despite their outbreaks growing exponentially. But it’s a matter of time. Either they have a massive epidemic, or they realize late their mistake, and have to overcompensate with a heavier Hammer. There is no escape from this.
But it’s doable. If an outbreak like South Korea’s can be controlled in weeks and without mandated social distancing, Western countries, which are already applying a heavy Hammer with strict social distancing measures, can definitely control the outbreak within weeks. It’s a matter of discipline, execution, and how much the population abides by the rules.
Once the Hammer is in place and the outbreak is controlled, the second phase begins: the Dance.
The Dance
If you hammer the coronavirus, within a few weeks you’ve controlled it and you’re in much better shape to address it. Now comes the longer-term effort to keep this virus contained until there’s a vaccine.
This is probably the single biggest, most important mistake people make when thinking about this stage: they think it will keep them home for months. This is not the case at all. In fact, it is likely that our lives will go back to close to normal.
In this video, the South Korea Foreign Minister explains how her country did it. It was pretty simple: efficient testing, efficient tracing, travel bans, efficient isolating and efficient quarantining.
Want to guess their measures? The same ones as in South Korea. In their case, they complemented with economic help to those in quarantine and travel bans and delays.
Is it too late for these countries and others? No. By applying the Hammer, they’re getting a new chance, a new shot at doing this right. The more they wait, the heavier and longer the hammer, but it can control the epidemics.
But what if all these measures aren’t enough?
The Dance of R
I call the months-long period between the Hammer and a vaccine or effective treatment the Dance because it won’t be a period during which measures are always the same harsh ones. Some regions will see outbreaks again, others won’t for long periods of time. Depending on how cases evolve, we will need to tighten up social distancing measures or we will be able to release them. That is the dance of R: a dance of measures between getting our lives back on track and spreading the disease, one of economy vs. healthcare.
How does this dance work?
It all turns around the R. If you remember, it’s the transmission rate. Early on in a standard, unprepared country, it’s somewhere between 2 and 3: During the few weeks that somebody is infected, they infect between 2 and 3 other people on average.
If R is above 1, infections grow exponentially into an epidemic. If it’s below 1, they die down.
During the Hammer, the goal is to get R as close to zero, as fast as possible, to quench the epidemic. In Wuhan, it is calculated that R was initially 3.9, and after the lockdown and centralized quarantine, it went down to 0.32.
But once you move into the Dance, you don’t need to do that anymore. You just need your R to stay below 1: a lot of the social distancing measures have true, hard costs on people. They might lose their job, their business, their healthy habits…
You can remain below R=1 with a few simple measures.
This is an approximation of how different types of patients respond to the virus, as well as their contagiousness. Nobody knows the true shape of this curve, but we’ve gathered data from different papers to approximate how it looks like.
Every day after they contract the virus, people have some contagion potential. Together, all these days of contagion add up to 2.5 contagions on average.
It is believed that there are some contagions already happening during the “no symptoms” phase. After that, as symptoms grow, usually people go to the doctor, get diagnosed, and their contagiousness diminishes.
For example, early on you have the virus but no symptoms, so you behave as normal. When you speak with people, you spread the virus. When you touch your nose and then open door knob, the next people to open the door and touch their nose get infected.
The more the virus is growing inside you, the more infectious you are. Then, once you start having symptoms, you might slowly stop going to work, stay in bed, wear a mask, or start going to the doctor. The bigger the symptoms, the more you distance yourself socially, reducing the spread of the virus.
Once you’re hospitalized, even if you are very contagious you don’t tend to spread the virus as much since you’re isolated.
This is where you can see the massive impact of policies like those of Singapore or South Korea:
If people are massively tested, they can be identified even before they have symptoms. Quarantined, they can’t spread anything.
If people are trained to identify their symptoms earlier, they reduce the number of days in blue, and hence their overall contagiousness
If people are isolated as soon as they have symptoms, the contagions from the orange phase disappear.
If people are educated about personal distance, mask-wearing, washing hands or disinfecting spaces, they spread less virus throughout the entire period.
Only when all these fail do we need heavier social distancing measures.
The ROI of Social Distancing
If with all these measures we’re still way above R=1, we need to reduce the average number of people that each person meets.
There are some very cheap ways to do that, like banning events with more than a certain number of people (eg, 50, 500), or asking people to work from home when they can.
Other are much, much more expensive economically, socially and ethically, such as closing schools and universities, asking everybody to stay home, or closing businesses.
This chart is made up because it doesn’t exist today. Nobody has done enough research about this or put together all these measures in a way that can compare them.
It’s unfortunate, because it’s the single most important chart that politicians would need to make decisions. It illustrates what is really going through their minds.
During the Hammer period, politicians want to lower R as much as possible, through measures that remain tolerable for the population. In Hubei, they went all the way to 0.32. We might not need that: maybe just to 0.5 or 0.6.
But during the Dance of the R period, they want to hover as close to 1 as possible, while staying below it over the long term term. That prevents a new outbreak, while eliminating the most drastic measures.
What this means is that, whether leaders realize it or not, what they’re doing is:
List all the measures they can take to reduce R
Get a sense of the benefit of applying them: the reduction in R
Get a sense of their cost: the economic, social, and ethical cost.
Stack-rank the initiatives based on their cost-benefit
Pick the ones that give the biggest R reduction up till 1, for the lowest cost.
This is for illustrative purposes only. All data is made up. However, as far as we were able to tell, this data doesn’t exist today. It needs to. For example, the list from the CDC is a great start, but it misses things like education measures, triggers, quantifications of costs and benefits, measure details, economic / social countermeasures…
Initially, their confidence on these numbers will be low. But that‘s still how they are thinking—and should be thinking about it.
What they need to do is formalize the process: Understand that this is a numbers game in which we need to learn as fast as possible where we are on R, the impact of every measure on reducing R, and their social and economic costs.
Only then will they be able to make a rational decision on what measures they should take.
Conclusion: Buy Us Time
The coronavirus is still spreading nearly everywhere. 152 countries have cases. We are against the clock. But we don’t need to be: there’s a clear way we can be thinking about this.
Some countries, especially those that haven’t been hit heavily yet by the coronavirus, might be wondering: Is this going to happen to me? The answer is: It probably already has. You just haven’t noticed. When it really hits, your healthcare system will be in even worse shape than in wealthy countries where the healthcare systems are strong. Better safe than sorry, you should consider taking action now.
For the countries where the coronavirus is already here, the options are clear.
On one side, countries can go the mitigation route: create a massive epidemic, overwhelm the healthcare system, drive the death of millions of people, and release new mutations of this virus in the wild.
On the other, countries can fight. They can lock down for a few weeks to buy us time, create an educated action plan, and control this virus until we have a vaccine.
Governments around the world today, including some such as the US, the UK or Switzerland have so far chosen the mitigation path.
That means they’re giving up without a fight. They see other countries having successfully fought this, but they say: “We can’t do that!”
What if Churchill had said the same thing? “Nazis are already everywhere in Europe. We can’t fight them. Let’s just give up.” This is what many governments around the world are doing today. They’re not giving you a chance to fight this. You have to demand it.
Share the Word
Unfortunately, millions of lives are still at stake. Share this article—or any similar one—if you think it can change people’s opinion. Leaders need to understand this to avert a catastrophe. The moment to act is now.
If you are an expert in the field and want to criticize or endorse the article or some of its parts, feel free to leave a private note here or contextually and I will respond or address.
If you want to translate this article, do it on a Medium post and leave me a private note here with your link. Here are the translations currently available:
This article has been the result of a herculean effort by a group of normal citizens working around the clock to find all the relevant research available to structure it into one piece, in case it can help others process all the information that is out there about the coronavirus.
Special thanks to Dr. Carl Juneau (epidemiologist and translator of the French version), Dr. Brandon Fainstad, Pierre Djian, Jorge Peñalva, John Hsu, Genevieve Gee, Elena Baillie, Chris Martinez, Yasemin Denari, Christine Gibson, Matt Bell, Dan Walsh, Jessica Thompson, Karim Ravji, Annie Hazlehurst, and Aishwarya Khanduja. This has been a team effort.
Thank you also to Berin Szoka, Shishir Mehrotra, QVentus, Illumina, Josephine Gavignet, Mike Kidd, and Nils Barth for your advice. Thank you to my company, Course Hero, for giving me the time and freedom to focus on this.
2 MSc in Engineering. Stanford MBA. Ex-Consultant. Creator of viral applications with >20M users. Currently leading a billion-dollar business @ Course Hero
A Itália de onde escrevo, um dos países mais vivazes e alegres do mundo, é hoje apenas um deserto. Cada um dos seus 60 milhões de habitantes acha que é imortal, que o vírus não o tocará, que irá matar não ele mas alguma outra pessoa. Porém, no silêncio do seu coração, cada um sabe que essa ilusão é pueril e que essa pandemia misteriosa, abstrata e tangível ao mesmo tempo, escolhe suas vítimas ao acaso, como numa roleta russa.
Em algum tempo vamos saber se o vírus pode ser debelado ou se nos matará em massa, assim como fez no século passado a famosa gripe espanhola, que matou 1 milhão de pessoas por semana durante 25 semanas seguidas.
Moro há 50 anos no centro de Roma, na rua mais movimentada da cidade, que leva da praça Veneza à Basílica de São Pedro.
Normalmente, essa rua está 24 horas por dia entupida de trânsito, de turistas e peregrinos. Há duas semanas, está muda e deserta. Só de vez em quando ouve-se o grito de uma sirene de ambulância e algum sem-teto passa. A cidade inteira está fantasmagórica como a Los Angeles de “Blade Runner”. Aqui, porém, desapareceram até os replicantes extraterrestres.
Fechados os lugares públicos, as escolas, as fábricas, as lojas, as estações, os portos e os aeroportos, a Itália é agora um país separado do resto da Europa e do mundo. Cada cidade está parada, cada família trancafiada em casa. Quem sai à revelia dos pouquíssimos motivos permitidos é interceptado imediatamente pelas rondas policiais que aplicam penas bastante severas.
Os gregos antigos consideravam que, quando algo é indispensável e todavia impossível, a situação é trágica. Foram necessários 50 dias, milhares de doentes e mortos para que os italianos entendessem que a situação é, enfim, irremediavelmente trágica.
O que significa uma pandemia como essa para Roma, para a Itália, para a humanidade como um todo? Como ela age nas mentes e nos corações de todos nós que, armados com tecnologias poderosas e inteligência artificial, até poucas semanas atrás nos sentíamos os senhores do céu e da terra?
Subitamente nos descobrimos frágeis pigmeus diante da onipotência imaterial de um vírus que, por vias misteriosas, escapou de um morcego chinês para vir matar homens e mulheres em nossas cidades.
A sujeição a um vírus desconhecido, para o qual não há nem cura nem vacina, transformou a Itália numa enorme caserna blindada e os 60 milhões de italianos noutros tantos dóceis soldadinhos empenhados num gigantesco exercício militar no qual estão obrigados a aprender a verdade que antes ignoravam obstinadamente. O que não quer dizer que irão apreendê-la.
Numa Europa onde, até ontem, era permitida a livre circulação de pessoas, mercadorias e dinheiro, agora cada país, em vez de abraçar uma colaboração ainda mais solidária com os demais, tranca suas próprias fronteiras, iludindo-se de forma cínica e infantil que seja possível deter o vírus com barreiras aduaneiras.
Contudo, hoje, mais do que nunca, os soberanismos parecem tentativas fantasiosas contra a globalização. Hoje, mais do que nunca, a difusão da pandemia e sua rápida volta ao mundo demonstraram que deter a globalização é como se opor à força de gravidade. Nosso planeta já é aquela “aldeia global” da qual falava McLuhan, unida por infortúnios e pela vontade de viver, precisando de uma direção unitária, capaz de coordenar a ação sinérgica de todos os povos que desejam se salvar. Nessa aldeia global, nenhum homem, nenhum país é uma ilha.
Talvez tenhamos aprendido que o caso agora é de vida ou morte e que ninguém pode enfrentar sozinho um vírus tão ardiloso e potente. Por isso, são necessários recursos, inteligências, competências, ações e instituições coletivas. Coordenação e coesão geral. É necessária uma cabine de comando, um governo competente que tenha autoridade, uma equipe formada por um vértice político de grande inteligência e apoiada pelos máximos representantes das ciências médicas, da economia, da sociologia, da psicologia social e da comunicação.
Talvez tenhamos aprendido que os fatos e os dados devem prevalecer sobre as opiniões, a competência reconhecida deva prevalecer sobre o simples bom senso, a prudência e a gradualidade das intervenções devem prevalecer às tomadas de decisões arrogantes e à improvisação imprudente. Por outro lado, é necessário tolerar os erros de quem possui a responsabilidade terrível de tomar decisões, líder que deve ser generosamente amparado para que sejam melhoradas.
Talvez tenhamos aprendido que, perante um vírus desconhecido, assim como diante de um problema complexo, as decisões sobre a pandemia não apenas devem ser tomadas pelas pessoas competentes mas também ser comunicadas de forma unívoca, com autoridade, prontamente, de forma abrangente e clara. Todo o alarmismo, todo o exagero, toda a subestimação é terrível porque confunde as ideias e nos faz perder um tempo precioso. Carência e excesso de informações são parâmetros nocivos. Talk shows superficiais e fake news delirantes levam ao cinismo e à desumanização.
Talvez tenhamos aprendido que, nos países civilizados, o bem-estar é uma conquista irrenunciável. Por sorte e pela sabedoria dos nossos pais, a Constituição italiana de 1948 considera a saúde como um direito fundamental de cada ser humano. Já a reforma sanitária de 1978 instituiu um serviço nacional universal que considera a saúde não como meramente a ausência de doença, mas como o bem-estar físico, psíquico e social completo.
Graças a esse regime de saúde, todos os residentes (e também os turistas) fruem dos cuidados médicos sem qualquer custo. Isso nos possibilitou descobrir e curar prontamente os contágios e reduzir o número de mortes.
No país mais rico e mais poderoso do mundo, os EUA, onde o bem-estar é estupidamente mortificado, os suspeitos de Covid-19 precisam desembolsar o equivalente a 1.200 euros pelo teste. O vírus corona, ao se difundir, causaria uma verdadeira hecatombe entre 90 milhões de estadunidenses que, desprovidos de seguro-saúde, seriam cinicamente rejeitados pelos hospitais.
A propaganda neoliberal, que se alastrou sob a bandeira insana de Reagan e Thatcher, desacreditou tudo o que é público em favor do setor privado. Porém, pelo contrário, nessas semanas trágicas, a reação eficiente dos hospitais e dos funcionários públicos diante do surgimento da pandemia nos ensinou que a nossa saúde pública, da mesma forma que outras funções públicas, dispõe, muito mais do que o setor privado, de pessoas preparadas profissionalmente, motivadas e generosas até o heroísmo.
Toda noite, às 18h, todas as janelas da Itália se escancaram e cada um canta ou toca o hino nacional para agradecer aos médicos e a todos os profissionais da saúde.
A pandemia está nos ensinando que o pensamento de Keynes permanece precioso. Em 1980, o prêmio Nobel Robert Lucas Jr. observou: “Não é possível encontrar nenhum bom economista com menos de 40 anos que se diga ‘keynesiano’. Nas universidades, as teorias keynesianas não são levadas a sério e provocam sorrisinhos de superioridade”.
Hoje, essa crise histórica, com seus mortos e com suas tragédias, se porum lado nos leva à recessão, por outro nos lembra que, para evitar uma crise irreparável, em vez de políticas de austeridade, é preferível dar lugar aos investimentos públicos maciços e “open-ended”, ainda que isso leve ao déficit público.
Talvez tenhamos aprendido tudo isso e várias outras coisas com aquilo que ocorreu fora do recinto doméstico, isto é, entre o governo e todo o povo do país. Entretanto, hoje, a nossa vida está segregada entre as paredes domésticas. Todos estão restritos entre as quatro paredes da própria casa: não só as famílias que vivem em harmonia e acordo, mas também os solitários, os casais em crise e os núcleos familiares em que o diálogo entre pais e filhos há muito tempo andava claudicante.
A sociedade industrial nos habituara a separar o local de trabalho do local de vida, nos fazendo passar a maior parte do nosso tempo com chefes e colegas nas empresas: os que a sociologia chama de grupos “secundários”, frios, formais, nos quais as relações são quase exclusivamente profissionais. Uma parte mínima do nosso tempo nos via reunidos em família ou com os amigos, ou seja, com grupos “primários”, calorosos, informais, envolventes.
De repente, o descanso compulsório em casa nos obrigou de forma inédita ao isolamento total, a uma convivência forçada que para alguns parece agradável e tranquilizadora, mas que para outros é invasiva e até opressora. Os mais sortudos conseguem transformar o ócio depressivo em ócio criativo, conjugando a leitura, o estudo, o lúdico com a parcela de trabalho que é possível desempenhar em regime de “smart working”.
Sabíamos teoricamente que essa modalidade de trabalho à distância permite aos trabalhadores uma preciosa economia de tempo, dinheiro, stress e alienação; e às empresas, evita os microconflitos, despesas na manutenção do local de trabalho e promove incremento da eficiência, recuperando de 15 a 20% da produtividade; à coletividade, evita a poluição, o entupimento de trânsito e despesas de manutenção das estradas.
Agora que 10 milhões de italianos, forçados pelo vírus, rapidamente adotaram o teletrabalho, minimizando seu sentimento de inutilidade e os danos à economia nacional, nos perguntamos por que as empresas não haviam adotado antes uma forma de organização tão eficaz e enxuta. A resposta está naquilo que os antropólogos definem como “cultural gap” —lacuna cultural— das empresas, dos sindicatos, dos chefes.
O tempo livre que, até um mês atrás, nos parecia um luxo raro, hoje abunda. O espaço, que nas cidades vazias se dilatou, por sua vez falta nas casas. Por isso, estamos apreciando a ajuda que nos chega da internet, graças à qual, mesmo permanecendo forçosamente distantes, é possível nos reunirmos virtualmente, nos informarmos, nos confrontarmos, nos encorajarmos.
Nessa reclusão, os jovens têm a maior vantagem, graças à sua facilidade com os computadores, enquanto os velhos têm mais vantagem por serem mais independentes, mais acostumados a estar em casa, fazendo pequenos trabalhos e jogos sedentários, contentando-se com a televisão.
Em todos se insinua o medo de que, mais cedo ou mais tarde, possa terminar o abastecimento dos mantimentos. O colapso da economia torna-se cada vez mais inevitável, já que tanto a produção como o consumo encontram-se bloqueados.
Há alguns anos, Kennet Building, um dos pais da teoria geral dos sistemas, comentando a sociedade opulenta, afirmou: “Quem acredita na possibilidade do crescimento infinito num mundo finito ou é louco ou é economista”. E Serge Latouche acrescentou: “O drama é que agora somos todos mais ou menos economistas. Aonde estamos nos encaminhando? Diretamente contra um muro. Estamos a bordo de um bólido sem piloto, sem marcha a ré e sem freios que irá se chocar contra os limites do planeta”. Latouche propõe abandonar a sociedade de consumo com um decrescimento planificado, progressivo e sereno.
A marcha a ré e os freios que a cultura neoliberal se recusou obstinadamente a usar agora foram desencadeados: não graças a uma revolução violenta, mas sim a um vírus invisível que um morcego soprou sobre a sociedade opulenta, obrigando-a a se repensar.
“A Peste” (1947), obra-prima profética de Albert Camus, talvez possa nos ajudar nesse repensar. Naquele romance, a ciência era protagonista, ou seja, o médico Bernardo Rieux, ocupado até o fim, como médico e como homem, de socorrer os contagiados, enquanto “o cheiro de morte emburrecia todos os que não matava”.
Hoje, nós também, como o nosso tão humano irmão Rieux, estamos presos num limbo entre o pesar e a esperança, no qual temos que aprender que “a peste pode vir e ir embora sem que o coração do homem seja modificado”; que “o bacilo da peste não morre nem desaparece nunca, que pode permanecer adormecido por décadas nos móveis e nas roupas, que espera pacientemente nos quartos, nas adegas, nas malas, nos lenços e nos papéis, que talvez chegue o dia em que, infortúnio ou lição aos homens, a peste acordará seus ratos para mandá-los morrer numa cidade feliz”.
Domenico De Masi, sociólogo italiano, é autor dos livros “Ócio Criativo” e “O Futuro do Trabalho”.
Coronavirus victims in Italy will be denied access to intensive care if they are aged 80 or more or in poor health should pressure on beds increase, a document prepared by a crisis management unit in Turin proposes.
Some patients denied intensive care will in effect be left to die, doctors fear.
The unit has drawn up a protocol, seen by The Telegraph, that will determine which patients receive treatment in intensive care and which do not if there are insufficient spaces. Intensive care capacity is running short in Italy as the coronavirus continues to spread.
The document, produced by the civil protection deparment of the Piedmont region, one of those hardest hit, says: “The criteria for access to intensive therapy in cases of emergency must include age of less than 80 or a score on the Charlson comorbidity Index [which indicates how many other medical conditions the patient has] of less than 5.”
The ability of the patient to recover from resuscitation will also be considered.
One doctor said: “[Who lives and who dies] is decided by age and by the [patient’s] health conditions. This is how it is in a war.”
The document says: “The growth of the current epidemic makes it likely that a point of imbalance between the clinical needs of patients with COVID-19 and the effective availability of intensive resources will be reached.
“Should it become impossible to provide all patients with intensive care services, it will be necessary to apply criteria for access to intensive treatment, which depends on the limited resources available.”
It adds: “The criteria set out guidelines if the situation becomes of such an exceptional nature as to make the therapeutic choices on the individual case dependent on the availability of resources, forcing [hospitals] to focus on those cases in which the cost/benefit ratio is more favorable for clinical treatment.”
Luigi Icardi, a councilor for health in Piedmont, said: “I never wanted to see such a moment. It [the document] will be binding and will establish in the event of saturation of the wards a precedence code for access to intensive care, based on certain parameters such as potential survival.”
The document is already complete and only approval from a technical-scientific committee is needed before it is sent to hospitals. The criteria are expected to apply throughout Italy, government sources said.
Italy has 5,090 intensive care beds, which for the moment exceeds the number of patients who need them. It is also working to create new bed capacity in private clinics, nursing homes and even in tents. However, the country also needs also doctors and nurses – the government wants to hire them – and equipment.
Lombardy remains the most critical region. However, the situation is also serious in neighboring Piedmont. Here, in just one day, 180 new cases were recorded, while deaths numbered 27. The trend suggests that the situation is not about to improve.
Roberto Testi, president of the coranavirus technical-scientific committee for Piedmont, told The Telegraph: “Here in Piedmont we aim to delay as long as possible the use of these criteria. At the moment there are still intensive care places available and we are working to create more.
“We want to arrive as late as possible at the point where we have to decide who lives and who dies. The criteria relate only to access to intensive care – those who do not get access to intensive care will still receive all the treatment possible. In medicine we sometimes have to make difficult choices but it’s important to have a system about how to make them.”
A medical official outside an emergency tent installed for patients infected by COVID-19 in Poland- Credit Sky News
Covid-19 is a flu-like illness (symptoms include fever, cough, and breathing problems) caused by a corona virus (SARS CoV-2). Like Ebola, the virus causing Covid-19 circulates within populations of bats and crossed over to humans via the bush meat trade. The first human cases were identified in China in December 2019, and the infection has now (March 2020) reached more than 100 countries.
The disease is now recognised by the World Health Organization as a pandemic. Up to 80 percent of the population of some countries might eventually become infected. Most cases will be mild, and recovery spontaneous. About 5 percent of cases will be life-threatening. Death rates appear to be around 1-2 percent. The elderly are most at risk.[1]
Currently, attention is focused on reducing the rate at which Covid-19 spreads. One aim is to delay the peak of infection beyond the winter flu period in the northern hemisphere, when medical help is stretched. Slowing the epidemic also allows more time for preparation of health systems to cope with large numbers, and for work on vaccine development.
Predictably, some politicians have demanded border closures against immigrants and refugees, even though spread is associated with tourism and normal business travel. Africans internationally stigmatised by Ebola might feel aggrieved that cases of Covid-19 have been introduced from Europe and Asia. But in a globally connected and inter-dependent world blaming and stigmatising helps no one. It is better to share ideas about what can be done to protect.
This is where Africa’s experience of Ebola has something to offer. Communities experiencing Ebola in West Africa in 2014-15 rapidly learnt from scratch how to cope with a deadly new infection, and this provides the rest of the world with important information on strategies to address novel disease threats more generally.
Like Ebola, Covid-19 is a family disease, in the sense that many infections occur in the home. Restrictions on travel can slow the spread of the disease, but it also helps if individuals and families understand infection pathways and implement domestic precautions. This is something in which West Africans confronted by Ebola have had much experience.
The name for Ebola in Mende, one of the main languages of Sierra Leone, the worst affected country in 2014-15, was bonda wote, literally ‘family turn round’. In other words, it was clearly recognised that this was a disease requiring families to change behaviour in major ways, especially in how they cared for the sick.
Covid-19 will require similar changes at the family level, especially in terms of how the elderly are protected. The buzz words for epidemic responders include self-isolation and social distancing, but the details of how to implement these vague concepts have been left to local social imagination.
Answers are required for both the uninfected elderly, and for others who are sick.
Should grandpa be packed off to a shed in the garden away from the family for his own protection? What happens when grandma gets lonely and wants to see the grandchildren? Who does the shopping? How does the daily-paid worker ‘self-isolate’ when there is no sick pay? Who collects the children from school when a single mum is sick?
Much depends on actual family arrangements and housing stock. So African solutions for Ebola will not work directly in other parts of the world. But it is important to know that under the challenge of Ebola local people showed much inventiveness in devising solutions to such problems.
Evidence shows that ways can be found to reduce family risks of infection, even with a disease 30 times more deadly than Covid-19.[2]For Ebola, these ranged from the elbow knock that replaced shaking of hands as a public greeting, to the appointment of a single carer in the household to look after the sick while waiting for help, to the carefully choreographed ‘safe and respectful’ funerals that allowed some element of local ritual back into the burial process, a major source of infection.
Every encouragement should be given to this local adaptive creativity, and the authorities should listen carefully to information from below about what would help to make a difference.
However, Covid-19 is not Ebola, and differences have to be taken into account. Some of the major questions about how the disease spreads are as yet unknown, and citizens and households need to be listening for this information as it becomes available and helped to adapt to its implications in real time.
This implies having very good means of two-way communication. In Sierra Leone a telephone helpline, ‘117’, played an important part in arranging emergency Ebola response, but it was much poorer at harvesting feedback from communities about what could be done better.
It seems that the lesson has not been learnt with Covid-19. In Britain, the National Health Service helpline, ‘111’ has now been ‘stood down’ for Covid-19 enquiries relating to domestic testing, since the epidemic is deemed to have passed into a new phase. How then are the authorities to have a conversation with families about the resources most needed for adaptation at household level?
Case-handling is a second area of difference. Ebola does not spread easily. The virologist Peter Piot put it well when he stated that he would have no problem sitting next to someone with Ebola provided they were not vomiting over him. Infection spreads only through contact with body fluids. Covid-19, however, spreads through the air, as well as via bodily contact, and case numbers will be much higher.
With Ebola in West Africa the number of cases turning up at specialist Ebola care facilities at the height of the epidemic numbered in tens or hundreds per week. With Covid-19 the numbers of cases requiring intensive care at the peak of the epidemic may amount to hundreds of thousands.
Even if stretched out over several months infection on this scale implies a large extra demand for medical care.
Ebola taught that epidemics cause deaths from other diseases through their impact on health systems. In all there were about 12,000 Ebola deaths in Upper West Africa (Guinea, Liberia, Sierra Leone) in 2014-15 but many additional fatalities resulted from, for example, closure of facilities such as maternity clinics.
So contingency planning is required. A key challenge for Covid-19 is how health system care should best be organized, without severely disrupting other forms of health provision.
For Ebola, the first response was to build large field hospitals (Ebola Treatment Centres).[3]These were seen as the safest option. But they were shunned by families, because so few patients came out alive. They were also often in the wrong place (built behind, not ahead, of the epidemic).
Information started to filter through that some communities were taking their own steps to reduce infection and bury the dead. This raised the question whether there was more scope for community care.
Family do-it-yourself responses proved controversial. International responders were adamant that there would be nothing resembling home care; it was too dangerous. Local communities were equally adamant that there would have to be some form of home care; they could not stand by and watch family members die, when an ambulance to take a patient to an ETC might take days to arrive over bad or non-existent roads.
Families saw it as their duty to be involved in care of the sick. So, they repeatedly asked what to do while waiting for help to arrive. Could they not prepare food for the sick? Could they not be trained to safely bury the dead?
No, they were told. Ebola required specialist management.
Communities answered back. They pointed to areas at the outset of the epidemic, where the epidemic was rolled back with only local resources. In Kailahun District, for example, an intense initial outbreak was reduced to a trickle of cases by local responders organizing quarantine and burial with improvised resources. That cases then declined without outside help implied either that the disease burnt out more readily than anticipated, or that local improvisation worked better than expected. There is evidence to support both interpretations.[4]
Experts knew that Ebola control required prompt diagnosis, before the ‘wet’ symptoms of the disease became apparent. Something had to be done to speed up the presentation of cases. The answer was to build much smaller community care centres (CCC) close to where active transmission was taking place.[5]This also changed the relationship between families and Ebola responders from fear to active cooperation.
Staff of CCC were for the most part local volunteers – trained nurses who had not been absorbed on to the payroll of the Ministry of Health, or villagers willing to take on high-risk chores for a decent wage. The fact that staffing was local meant patients saw familiar faces, and this built trust. CCC also normalized Ebola by bringing treatment within a framework of general medical assistance.
As a result, patients were presented more promptly than was the case with the distant ETC. Ebola (indistinguishable from malaria or typhoid in its early phase) was more rapidly identified and isolated. One study estimates that CCC contributed up to one third of the infection control ending the epidemic in Sierra Leone.[6]
This example of responders modifying their approach to infection control better to accommodate family requirements may hold lessons for Covid-19.
Specifically, cases may have to be kept out of main hospitals as much as possible, Thus, there may be a need for field treatment facilities not dissimilar to CCC, as a half-way house between home isolation and intensive care. In effect these facilities would isolate and triage the most vulnerable cases, as was the case with Ebola CCC.
There is also a possibility that any such facilities might be run up by military personnel[7]and staffed by medically trained ‘volunteers’ (retired doctors and nurses), as in Sierra Leone.
Interesting to note, the chief medical advisor for England was previously one of the proponents of the introduction of CCC in Sierra Leone, and we may be about to see some lessons directly transferred.[8]
Quarantine for Ebola in Sierra Leone is also an issue from which Covid-19 responders might wish to draw lessons. Much of it was organised and imposed by the state, and was at times heavy-handed. But communities also organised their own quarantine. They understood that self-isolation was in their own interest, and this sometimes worked surprisingly effectively.
Use was made of an approach used during the civil war of 1991-2002 of mobilising community youth to identify infiltrators. Visitors who might have been carrying the virus were turned away. But in other cases the approach was more focused on sequestering those who were well. Rural families sometimes decamped from villages with outbreaks to settle down for a few weeks in their farms, where sleeping quarters were sometimes built for the purpose.
In this respect, Sierra Leonean rural communities showed a clear appreciation of the fact that there were two distinct kinds of quarantine – self-isolation and protective sequestration. Both kinds are being used as part of the response to Covid-19, but at times without adequate discussion of how the two types differ and have different social motivations – self-protection and altruism towards neighbours. It is not wise to talk about self-isolation for the sick and the elderly in the same breath. The different motivations need to be more clearly explained.
In conclusion, it is also important to say something about what Africa can learn from its own experience of Ebola. The point made above should be reiterated – about the differences as well as similarities between Covid-19 and Ebola.
Prompt case finding, contact tracing and quarantine are being applied to Covid-19 as they were for Ebola.[9]Good hygiene practices, such as hand washing, also remain applicable. African countries with experience of Ebola know how to do these things, and this will be helpful in dealing with early cases.
However, African countries also have to be prepared to learn to adapt to the specific features of this new disease as more data emerge. This will pose more of a challenge, since this will require rapid knowledge-based domestic adaptation to new information on how Covid-19 spreads (perhaps most notably, why it affects the old more than the young, and how older people might be best protected from its effects).
The main lesson for both Africa and other parts of the world from Ebola for Covid-19, however, is that shared learning between communities and medical professionals is a key aspect of human adaptive response to emergent diseases. In any disease in which community mobilization is an important aspect families need to think like epidemiologists, but equally epidemiologists need to think like families.
Paul Richards’ Ebola book front cover, part of the African Arguments book series
References:
[1]Xu, J., Zhao, S., Teng T., Abdalla, A.E., Zhu, W., Xie, L., Wang, Y., Guo, X. (2020) ‘Systematic comparison of two animal-to-human transmitted human coronaviruses: SARS-CoV-2 and SARS-CoV’, Viruses 12, 244.
[2]Richards, P. (2016) Ebola: How a People’s Science Helped End an Epidemic, London: Zed Books.
[3]Richards, P., Mokuwa, E., Welmers, P., Maat, H., Beisel, U. (2019) ‘Trust, and distrust, of Ebola Treatment Centers: a case-study from Sierra Leone’, PLoS ONE14(12): e0224511. https://doi.org/10.1371/journal.pone.0224511.
[4]Glynn, Judith R. et al. (2017) ‘Asymptomatic infection and unrecognised Ebola virus disease in Ebola-affected households in Sierra Leone: a cross-sectional study using a new non-invasive assay for antibodies to Ebola virus’,Lancet Infectious Diseases17(6), 645-653. On local case finding, quarantine and burial procedures see Richards (2016) op. cit.
[5]Mokuwa, E.Y., Maat, H. (2020) ‘Rural populations exposed to Ebola Virus Disease respond positively to localised case handling: evidence from Sierra Leone’, PLoS Negl Trop Dis 14(1): e0007666. https://doi.org/10.1371/journal.pntd.0007666.
[6]Pronyk, P., Rogers, B., Lee, S., Bhatnagar, A., Wolman, Y., Monasch, R., Hipgrave, D., Salama, P., Kucharski, A., Chopra, M., and on behalf of the UNICEF Sierra Leone Ebola Response Team, (2016) ‘The effect of community-based prevention and care on Ebola transmission in Sierra Leone’,American Journal of Public Health 106, 727–32, https://doi.org/10.2105/AJPH.2015.303020.
[7]Aaaron Walawalkar and Jamie Grierson, The Guardian,8 March 2020, 14.12 GMT.
[8]Whitty, C.J.M., Farrar, J., Ferguson, N., Edmunds, W.J., Piot, P., Leach, M., Davies, S.C. (2014) ‘Tough choices to reduce Ebola transmission’, Nature515, 13 November, 192–4; see also Ian Sample and Lisa O’Carroll ‘Prof Chris Whitty – the expert we need in the coronavirus crisis’, Guardian,4 March 2020.
El Niño may carry disease-causing Vibrio bacteria across Pacific
Previous events linked to cases of diarrhoea and cholera
Current El Niño developing similarly to 1977 one when diarrhoea reached Peru
The ongoing El Niño event may be spreading cholera and other diseases caused by Vibrio bacteria from Asia to South America, researchers suggest.
This is because the bacteria, which are typically found in salty water, could ‘piggyback’ on zooplankton that travel to Peru and Chile with the warm easterly and southerly Pacific currents associated with El Niño, according to a comment published in Nature Microbiology last month.
Vibrio bacteria cause severe diarrhoea when people eat raw, contaminated molluscs such as oysters, clams and mussels. Such outbreaks have been linked to previous El Niño episodes.
The ongoing El Niño — dubbed El Niño Godzilla because of its intensity — may be the strongest on record. It is developing similarly to an episode in 1977, during which a diarrhoea epidemic broke out in Peru. In that year, Vibrio parahaemolyticus bacteria caused an estimated 10,000 cases of severe gastroenteritis along the South American coastline.
In 1997, another strong El Niño year, the Vibrio parahaemolyticus strain of the bacteria, which had emerged in India, plagued the South American coast.
“The emergence of cases correlated with southward dissemination of El Niño water during the 1997 event,” says Jaime Martinez-Urtaza, a biologist at the University of Bath in the United Kingdom, and a coauthor of the article.
In terms of cholera, South America had been free of the disease for almost a century — until it reemerged in the early 1990s. Within weeks, cholera spread across South and Central America, going on to cause more than a million cases and 10,000 deaths by 1994.
Martinez-Urtaza says the cholera outbreak “coincided in both time and space with a significant El Niño event in late 1991 and early 1992”.
Ronnie Gavilán, a researcher at Peru’s National Institute of Health, says there is other evidence for El Niño’s influence on Vibrio bacteria in the Americas. He points out that, during warm El Niño events, Vibrioinfections continue to spread in the cold winter months, when they usually only occur in hot summers.
The current El Niño has not yet led to a Vibrio outbreak, but health authorities in Chile and Peru are closely monitoring water quality near the coast.
The delay could be “because the pathogens that may have arrived during the summer season may show up years later”, says Romilio Orellana, a biochemist at the University of Chile.
With the proposed connection between the Zika virus and Brazil’s outbreak of microcephaly in new born babies looking increasingly tenuous, Latin American doctors are proposing another possible cause: Pyriproxyfen, a pesticide used in Brazil since 2014 to arrest the development of mosquito larvae in drinking water tanks. Might the ‘cure’ in fact be the poison?
Malformations detected in thousands of children from pregnant women living in areas where the Brazilian state added Pyriproxyfen to drinking water are not a coincidence, even though the Ministry of Health places direct blame on the Zika virus.
The World Health Organization view that the microcephaly outbreak in Brazil’s impoverished northeast is caused by the Zika virus has, so far, received few challenges.
Brazil’s Health Minister, Marcelo Castro, has gone so far as to say that he has “100% certainty”that there is a link between Zika and microcephaly, a birth defect in which babies are born with small heads.
The view is widely supported in the medical community worldwide, including by the US’s influential Center for Disease Control. But there is no hard evidence of the link, rather a mixture of epidemiological indications and circumstantial evidence.
One of the key scientific papers, by A S Oliveira Melo et al in the journal Ultrasound in Obstetrics & Gynecology, found Zika virus in the amniotic fluids and other tissues of the affected babies and their mothers. But only two women were examined, far too small a number to establish a statistically significant link.
The New York Times also reported on 3rd February on the outcome of analyses by Brazil’s Health Ministry: “Of the cases examined so far, 404 have been confirmed as having microcephaly. Only 17 of them tested positive for the Zika virus. But the government and many researchers say that number may be largely irrelevant, because their tests would find the presence of the virus in only a tiny percentage of cases.”
And last weekend, the most powerful indicator yet that the microcephaly may have another cause altogether was announced by Colombia’s president, Juan Manuel Santos, as reported by the Washington Post. Colombian public health officials, stated Santos, have so far diagnosed 3,177 pregnant women with the Zika virus- but in no case had microcephaly been observed in the foetus.
Argentine doctors: it’s the insecticide
Now a new report has been published by the Argentine doctors’ organisation, Physicians in the Crop-Sprayed Towns (PCST), [1] which not only challenges the theory that the Zika virus epidemic in Brazil is the cause of the increase in microcephaly among newborns, but proposes an alternative explanation.
According to PCST, the Ministry failed to recognise that in the area where most sick people live, a chemical larvicide that produces malformations in mosquitoes was introduced into the drinking water supply in 2014.
This pesticide, Pyriproxyfen, is used in a state-controlled programme aimed at eradicating disease-carrying mosquitos. The Physicians added that the Pyriproxyfen is manufactured by Sumitomo Chemical, a Japanese ‘strategic partner‘ of Monsanto. – a company they have learned to distrust due to the vast volume of the company’s pesticides sprayed onto Argentina’s cropland.
Pyriproxyfen is a growth inhibitor of mosquito larvae, which alters the development process from larva to pupa to adult, thus generating malformations in developing mosquitoes and killing or disabling them. It acts as an insect juvenile hormone or juvenoid, and has the effect of inhibiting the development of adult insect characteristics (for example, wings and mature external genitalia) and reproductive development.
The chemical has a relatively low risk profile as shown by its WHO listing, with low acute toxicity. Tests carried out in a variety of animals by Sumitomo found that it was not a teratogen (did not cause birth defects) in the mammals it was tested on. However this cannot be taken as a completely reliable indicator of its effects in humans – especially in the face of opposing evidence.
The PCST commented: “Malformations detected in thousands of children from pregnant women living in areas where the Brazilian state added Pyriproxyfen to drinking water are not a coincidence, even though the Ministry of Health places a direct blame on the Zika virus for this damage.”
They also noted that Zika has traditionally been held to be a relatively benign disease that has never before been associated with birth defects, even in areas where it infects 75% of the population.
Brazilian doctors also suspect pyriproxyfen
Pyriproxyfen is a relatively new introduction to the Brazilian environment; the microcephaly increase is a relatively new phenomenon. So the larvicide seems a plausible causative factor in microcephaly – far more so than GM mosquitos, which some have blamed for the Zika epidemic and thus for the birth defects.
The PCST report, which also addresses the Dengue fever epidemic in Brazil, concurs with the findings of a separate report on the Zika outbreak by the Brazilian doctors’ and public health researchers’ organisation, Abrasco. [2]
Abrasco also names Pyriproxyfen as a possible cause of the microcephaly. It condemns the strategy of chemical control of Zika-carrying mosquitoes, which it says is contaminating the environment as well as people and is not decreasing the numbers of mosquitoes.
Instead Abrasco suggests that this strategy is in fact driven by the commercial interests of the chemical industry, which it says is deeply integrated into the Latin American ministries of health, as well as the World Health Organization and the Pan American Health Organisation.
Abrasco names the British GM insect company Oxitec as part of the corporate lobby that is distorting the facts about Zika to suit its own profit-making agenda. Oxitec sells GM mosquitoes engineered for sterility and markets them as a disease-combatting product – a strategy condemned by the Argentine Physicians as “a total failure, except for the company supplying mosquitoes.”
Both the Brazilian and Argentine doctors’ and researchers’ associations agree that poverty is a key neglected factor in the Zika epidemic. Abrasco condemned the Brazilian government for its “deliberate concealment” of economic and social causes: “In Argentina and across America the poorest populations with the least access to sanitation and safe water suffer most from the outbreak.” PCST agrees, stating, “The basis of the progress of the disease lies in inequality and poverty.”
Abrasco adds that the disease is closely linked to environmental degradation: floods caused by logging and the massive use of herbicides on (GM) herbicide-tolerant soy crops – in short, “the impacts of extractive industries.”
The notion that environmental degradation may a factor in the spread of Zika finds backing in the view of Dino Martins, PhD, a Kenyan entomologist. Martins said that “the explosion of mosquitoes in urban areas, which is driving the Zika crisis” is caused by “a lack of natural diversity that would otherwise keep mosquito populations under control, and the proliferation of waste and lack of disposal in some areas which provide artificial habitat for breeding mosquitoes.”
Community-based actions
The Argentine Physicians believe that the best defence against Zika is “community-based actions”. An example of such actions is featured in a BBC News report on the Dengue virus in El Salvador.
A favourite breeding place for disease-carrying mosquitoes is storage containers of standing water. El Salvadorians have started keeping fish in the water containers, and the fish eat the mosquito larvae. Dengue has vanished along with the mosquitoes that transmit the disease. And so far, the locals don’t have any Zika cases either.
Simple yet effective programmes like this are in danger of being neglected in Brazil in favour of the corporate-backed programmes of pesticide spraying and releasing GM mosquitoes. The latter is completely unproven and the former may be causing far more serious harm than the mosquitoes that are being targeted.
Comitê de Emergência se reuniu pela primeira vez nesta segunda-feira (1) para reagir ao aumento do número de casos de desordens neurológicas e malformações congênitas, sobretudo nas Américas. País mais atingido é o Brasil
A Organização Mundial da Saúde (OMS) realizou nesta segunda-feira (1) a primeira reunião do Comité de Emergência que trata dos recentes casos de microcefalia e outros distúrbios neurológicos em áreas afetadas pelo vírus zika, sobretudo nas Américas. O país mais atingido é o Brasil.
O Secretariado da OMS informou ao Comitê sobre a situação dos casos de microcefalia e Síndrome de Guillain-Barré, circunstancialmente associados à transmissão do vírus zika. O Comitê foi recebeu informações sobre a história do vírus zika, sua extensão, apresentação clínica e epidemiologia.
As representações do Brasil, França, Estados Unidos e El Salvador apresentaram as primeiras informações sobre uma potencial associação entre a microcefalia – bem como outros distúrbios neurológicos – e a doença provocada pelo vírus zika.
Segundo o comunicado da OMS, os especialistas reunidos em Genebra concordam que uma relação causal entre a infecção do zika durante a gravidez e microcefalia é “fortemente suspeita”, embora ainda não comprovada cientificamente.
A falta de vacinas e testes de um diagnóstico rápido e confiável, bem como a ausência de imunidade da população em países recém-afetados, foram citadas como novos motivos de preocupação.
Para a Comissão da OMS, o recente conjunto de casos microcefalia e outros distúrbios neurológicos relatados no Brasil, logo após ocorrências semelhantes na Polinésia Francesa, em 2014, constituem uma “emergência de saúde pública de importância internacional”, condição conhecida também pela sua sigla em inglês (PHEIC).
Em uma decisão aceita pela diretora-geral da OMS, Margaret Chan, o Comitê da agência da ONU busca assim coordenar uma resposta global de modo a minimizar a ameaça nos países afetados e reduzir o risco de propagação internacional.
Recomendações à diretora-geral da OMS
O Comitê, em resposta às informações fornecidas, fez recomendações à OMS sobre medidas a serem tomadas.
Em relação aos distúrbios neurológicos e microcefalia, o Comitê sugere que a vigilância de microcefalia e da Síndrome de Guillain-Barré deve ser padronizada e melhorada, particularmente em áreas conhecidas de transmissão do vírus zika, bem como em áreas de risco de transmissão.
O Comitê também recomendou que seja intensificada a investigação acerca da etiologia – a causa das doenças – nos novos focos onde ocorrem os casos de distúrbios neurológicos e de microcefalia, para determinar se existe uma relação causal entre o vírus zika e outros fatores desconhecidos.
Como estes grupos se situam em áreas recém-infectadas com o vírus zika, de acordo com as boas práticas de saúde pública e na ausência de outra explicação para esses agrupamentos, o Comitê destaca a importância de “medidas agressivas” para reduzir a infecção com o vírus zika, especialmente entre as mulheres grávidas e mulheres em idade fértil.
Como medida de precaução, o Comitê fez as seguintes recomendações adicionais:
Transmissão do vírus zika
A vigilância para infecção pelo vírus zika deve ser reforçada, com a divulgação de definições de casos padrão e diagnósticos para áreas de risco.
O desenvolvimento de novos diagnósticos de infecção pelo vírus zika devem ser priorizados para facilitar as medidas de vigilância e de controle.
A comunicação de risco deve ser reforçada em países com transmissão do vírus zika para responder às preocupações da população, reforçar o envolvimento da comunidade, melhorar a comunicação e assegurar a aplicação de controle de vetores e medidas de proteção individual.
Medidas de controle de vetores e medidas de proteção individual adequada devem ser agressivamente promovidas e implementadas para reduzir o risco de exposição ao vírus zika.
Atenção deve ser dada para assegurar que as mulheres em idade fértil e mulheres grávidas em especial tenham as informações e materiais necessários para reduzir o risco de exposição.
As mulheres grávidas que tenham sido expostas ao vírus zika devem ser aconselhadas e acompanhadas por resultados do nascimento com base na melhor informação disponível e práticas e políticas nacionais.
Medidas de longo prazo
Esforços de pesquisa e desenvolvimento apropriados devem ser intensificados para vacinas, terapias e diagnósticos do vírus zika.
Em áreas conhecidas de transmissão do vírus zika, os serviços de saúde devem estar preparados para o aumento potencial de síndromes neurológicas e/ou malformações congênitas.
Medidas de viagem
Não deve haver restrições a viagens ou ao comércio com países, regiões e/ou territórios onde esteja ocorrendo a transmissão do vírus zika.
Viajantes para áreas com transmissão do vírus zika devem receber informações atualizadas sobre os potenciais riscos e medidas adequadas para reduzir a possibilidade de exposição a picadas do mosquito.
Recomendações da OMS sobre padrões em matéria de desinfestação de aeronaves e aeroportos devem ser implementadas.
Compartilhamento de dados
As autoridades nacionais devem garantir a comunicação e o compartilhamento ágeis e em tempo de informações relevantes de importância para a saúde pública, para esta Emergência.
Dados clínicos, virológicos e epidemiológicos, relacionados com o aumento das taxas de microcefalia e/ou Síndrome de Guillain-Barré, ou com a transmissão do vírus zika, devem ser rapidamente compartilhados com a OMS para facilitar a compreensão internacional destes eventos, para orientar o apoio internacional para os esforços de controle, priorizando a pesquisa e desenvolvimento de produtos.
Pandora’s box: how GM mosquitos could have caused Brazil’s microcephaly disaster (The Ecologist)
Oliver Tickell
1st February 2016
Aedes Aegypti mosquito feeding on human blood. This is the species that transmits Zika, and that was genetically engineered by Oxitec using the piggyBac transposon. Photo: James Gathany via jentavery on Flickr (CC BY).
In Brazil’s microcephaly epidemic, one vital question remains unanswered: how did the Zika virus suddenly learn how to disrupt the development of human embryos? The answer may lie in a sequence of ‘jumping DNA’ used to engineer the virus’s mosquito vector – and released into the wild four years ago in the precise area of Brazil where the microcephaly crisis is most acute.
These ‘promiscuous’ transposons have found special favour with genetic engineers, whose goal is to create ‘universal’ systems for transferring genes into any and every species on earth. Almost none of the geneticists has considered the hazards involved.
Since August 2015, a large number of babies in Northeast Brazil have been born with very small heads, a condition known as microcephaly, and with other serious malformations. 4,180 suspected cases have been reported.
Epidemiologists have found a convincing correlation between the incidence of the natal deformities and maternal infections with the Zika virus, first discovered in Uganda’s Zika Valley in 1947, which normally produces non-serious illness.
The correlation has been evidenced through the geographical distrubution of Zika infections and the wave of deformities. Zika virus has also been detected in the amniotic fluids and other tissues of the affected babies and their mothers.
This latter finding was recently reported by AS Oliveira Melo et al in a scientific paperpublished in the journal Ultrasound in Obstetrics & Gynecology, which noted evidence of intra-uterine infection. They also warn:
“As with other intrauterine infections, it is possible that the reported cases of microcephaly represent only the more severely affected children and that newborns with less severe disease, affecting not only the brain but also other organs, have not yet been diagnosed.”
The Brazilian Health Minister, Marcelo Castro, says he has “100% certainty” that there is a link between Zika and microcephaly. His view is supported by the medical community worldwide, including by the US Center for Disease Control.
Oliveira Melo et al draw attention to a mystery that lies at the heart of the affair: “It is difficult to explain why there have been no fetal cases of Zika virus infection reported until now but this may be due to the underreporting of cases, possible early acquisition of immunity in endemic areas or due to the rarity of the disease until now.
“As genomic changes in the virus have been reported, the possibility of a new, more virulent, strain needs to be considered. Until more cases are diagnosed and histopathological proof is obtained, the possibility of other etiologies cannot be ruled out.”
And this is the key question: how – if indeed Zika really is the problem, as appears likely – did this relatively innocuous virus acquire the ability to produce these terrible malformations in unborn human babies?
Oxitec’s GM mosquitoes
An excellent article by Claire Bernish published last week on AntiMedia draws attention to an interesting aspect of the matter which has escaped mainstream media attention: the correlation between the incidence of Zika and the area of release of genetically modified Aedes aegypti mosquitos engineered for male insterility (see maps, above right).
The purpose of the release was to see if it controlled population of the mosquitos, which are the vector of Dengue fever, a potentially lethal disease. The same species also transmits the Zika virus.
The releases took in 2011 and 2012 in the Itaberaba suburb of the city of Juazeiro, Bahia, Northeast Brazil, about 500 km west of ther coastal city of Recife. The experiment was written up in July 2015 in the journal PLOS Neglected Tropical Diseases in a paper titled ‘Suppression of a Field Population of Aedes aegypti in Brazil by Sustained Release of Transgenic Male Mosquitoes’ by Danilo O. Carvalho et al.
An initial ‘rangefinder of 30,000 GM mosquitos per week took place between 19th May and 29th June 2011, followed by a much larger release of 540,000 per week in early 2012, ending on 11th February.
At the end of it the scientists claimed “effective control of a wild population of Ae. aegypti by sustained releases of OX513A male Ae. aegypti. We diminished Ae. aegypti population by 95% (95% CI: 92.2%-97.5%) based on adult trap data and 78% (95% CI: 70.5%-84.8%) based on ovitrap indices compared to the adjacent no-release control area.”
So what’s to worry about?
The idea of the Oxitec mosquitoes is simple enough: the males produce non-viable offspring which all die. So the GM mosqitoes are ‘self-extinguishing’ and the altered genes cannot survive in the wild population. All very clever, and nothing to worry about!
But in fact, it’s not so simple. In 2010 geneticist Ricarda Steinbrecher wrote to the biosafety regulator in Malaysia – also considering a release of the Oxitec mosquitoes – with a number of safety concerns, pointing out the 2007 finding by Phuc et al that 3-4% of the first generation mosquitos actually survive.
The genetic engineerig method employed by Oxitec allows the popular antibiotic tetracycline to be used to repress the lethality during breeding. But as a side-effect, the lethality is also reduced by the presence of tetracycline in the environment; and as Bernish points out, Brazil is among the world’s biggest users of anti-microbials including tetracycline in its commercial farming sector:
“As a study by the American Society of Agronomy, et. al., explained, ‘It is estimated that approximately 75% of antibiotics are not absorbed by animals and are excreted in waste.’ One of the antibiotics (or antimicrobials) specifically named in that report for its environmental persistence is tetracycline.
In fact, as a confidential internal Oxitec document divulged in 2012, that survival rate could be as high as 15% – even with low levels of tetracycline present. ‘Even small amounts of tetracycline can repress’ the engineered lethality. Indeed, that 15% survival rate was described by Oxitec.”
She then quotes the leaked Oxitec paper: “After a lot of testing and comparing experimental design, it was found that [researchers] had used a cat food to feed the [OX513A] larvae and this cat food contained chicken. It is known that tetracycline is routinely used to prevent infections in chickens, especially in the cheap, mass produced, chicken used for animal food. The chicken is heat-treated before being used, but this does not remove all the tetracycline. This meant that a small amount of tetracycline was being added from the food to the larvae and repressing the [designed] lethal system.”
So in other words, there is every possibility for Oxitec’s modified genes to persist in wild populations of Aedes aegypti mosquitos, especially in the environmental presence of tetracycline which is widely present in sewage, septic tanks, contaminated water sources and farm runoff.
‘Promiscuous’ jumping genes
On the face of it, there is no obvious way in which the spread of Oxitec’s GM mosquitos into the wild could have anything to do with Brazil’s wave of micrcophaly. Is there?
Actually, yes. The problem may arise from the use of the ‘transposon’ (‘jumping’ sequence of DNA used in the genetic engineering process to introduce the new genes into the target organism). There are several such DNA sequences in use, and one of the most popular is known as known as piggyBac.
As a 2001 review article by Dr Mae Wan Ho shows, piggyBac is notoriously active, inserting itself into genes way beyond its intended target: “These ‘promiscuous’ transposons have found special favour with genetic engineers, whose goal is to create ‘universal’ systems for transferring genes into any and every species on earth. Almost none of the geneticists has considered the hazards involved …
“It would seem obvious that integrated transposon vectors may easily jump out again, to another site in the same genome, or to the genome of unrelated species. There are already signs of that in the transposon, piggyBac, used in the GM bollworms to be released by the USDA this summer.
The piggyBac transposon was discovered in cell cultures of the moth Trichopulsia, the cabbage looper, where it caused high rates of mutations in the baculovirus infecting the cells by jumping into its genes … This transposon was later found to be active in a wide range of species, including the fruitfly Drosophila, the mosquito transmitting yellow fever, Aedes aegypti, the medfly, Ceratitis capitata, and the original host, the cabbage looper.
“The piggyBac vector gave high frequencies of transpositions, 37 times higher than mariner and nearly four times higher than Hirmar.”
In a later 2014 report Dr Mae Wan Ho returned to the theme with additional detail and fresh scientific evidence (please refer to her original article for references): “The piggyBac transposon was discovered in cell cultures of the moth Trichopulsia, the cabbage looper, where it caused high rates of mutations in the baculovirus infecting the cells by jumping into its genes …
“There is also evidence that the disabled piggyBac vector carrying the transgene, even when stripped down to the bare minimum of the border repeats, was nevertheless able to replicate and spread, because the transposase enzyme enabling the piggyBac inserts to move can be provided by transposons present in all genomes.
“The main reason initially for using transposons as vectors in insect control was precisely because they can spread the transgenes rapidly by ‘non-Mendelian’ means within a population, i.e., by replicating copies and jumping into genomes, thereby ‘driving’ the trait through the insect population. However, the scientists involved neglected the fact that the transposons could also jump into the genomes of the mammalian hosts including human beings …
“In spite of instability and resulting genotoxicity, the piggyBac transposon has been used extensively also in human gene therapy. Several human cell lines have been transformed, even primary human T cells using piggyBac. These findings leave us little doubt that the transposon-borne transgenes in the transgenic mosquito can transfer horizontally to human cells. The piggyBac transposon was found to induce genome wide insertionmutations disrupting many gene functions.”
Has the GM nightmare finally come true?
So down to the key question: was the Oxitec’s GM Aedes aegypti male-sterile mosquito released in Juazeiro engineered with the piggyBac transposon? Yes, it was. And that creates a highly significant possibility: that Oxitec’s release of its GM mosquitos led directly to the development of Brazil’s microcephaly epidemic through the following mechanism:
1. Many of the millions of Oxitec GM mosquitos released in Juazeiro in 2011/2012 survive, assisted, but not dependent on, the presence of tetracycline in the environment.
2. These mosquitos interbreed with with the wild population and their novel genes become widespread.
3. The promiscuous piggyBac transposon now present in the local Aedes aegyptipopulation takes the opportunity to jump into the Zika virus, probably on numerous occasions.
4. In the process certain mutated strains of Zika acquire a selective advantage, making them more virulent and giving them an enhanced ability to enter and disrupt human DNA.
5. One way in which this manifests is by disrupting a key stage in the development of human embryos in the womb, causing microcephaly and the other reported deformations. Note that as Melo Oliveira et al warn, there are almost certainly other manifestations that have not yet been detected.
6. It may be that the piggyBac transposon has itself entered the DNA of babies exposed in utero to the modified Zika virus. Indeed, this may form part of the mechanism by which embryonic development is disrupted.
In the latter case, one implication is that the action of the gene could be blocked by giving pregnant women tetracycline in order to block its activity. The chances of success are probably low, but it has to be worth trying.
No further releases of GM insects!
While I am certainly not claiming that this is what actually took place, it is at least a credible hypothesis, and moreover a highly testable one. Nothing would be easier for genetic engineers than to test amniotic fluids, babies’ blood, wild Aedes mosquitos and the Zika virus itself for the presence of the piggyBac transposon, using well established and highly sensitive PCR (polymerase chain reaction) techniques.
If this proves to be the case, those urging caution on the release of GMOs generally, and transgenic insects bearing promiscuous transposons in particular, will have been proved right on all counts.
But most important, such experiments, and any deployment of similar GM insects, must be immediately halted until the possibilities outlined above can be safely ruled out. There are plans, for example, to release similarly modified Anopheles mosquitos as an anti-malarial measure.
There are also calls for even more of the Oxitec Aedes aegypti mosquitos to be released in order to halt the transmission of the Zika virus. If that were to take place, it could give rise to numerous new mutations of the virus with the potential to cause even more damage to the human genome, that we can, at this stage, only guess at.
A new ridiculous rumor is spreading around the internets. According to conspiracy theorists, the recent outbreak of Zika can be blamed on the British biotech company Oxitec, which some are saying even intentionally caused the disease as a form of ethnic cleansing or population control. The articles all cite a lone Redditor who proposed the connection on January 25th to the Conspiracy subreddit. “There are no biological free lunches,” says one commenter on the idea. “Releasing genetically altered species into the environment could have disastrous consequences” another added. “Maybe that’s what some entities want to happen…?”
For some reason, it’s been one of those months where random nonsense suddenly hits mainstream. Here are the facts: there’s no evidence whatsoever to support this conspiracy theory, or any of the other bizarre, anti-science claims that have popped up in the past few weeks. So let’s stop all of this right here, right now: The Earth is round, not flat (and it’s definitely not hollow). Last year was the hottest year on record, and climate change is really happening (so please just stop, Mr. Cruz). And FFS, genetically modified mosquitoes didn’t start the Zika outbreak.
Background on Zika
The Zika virus is a flavivirus closely related to notorious pathogens including dengue, yellow fever, Japanese encephalitis, and West Nile virus. The virus is transmitted by mosquitoes in the genus Aedes, especially A. aegypti, which is a known vector for many of Zika’s relatives. Symptoms of the infection appear three to twelve days post bite. Most people are asymptomatic, which means they show no signs of infection. The vast majority of those who do show signs of infection report fever, rash, joint pain, and conjunctivitis (red eyes), according to the U.S. Centers for Disease Control. After a week or less, the symptoms tend to go away on their own. Serious complications have occurred, but they have been extremely rare.
The Zika virus isn’t new. It was first isolated in 1947 from a Rhesus monkey in the Zika Forest in Uganda, hence the pathogen’s name. The first human cases were confirmed in Uganda and Tanzania in 1952, and by 1968, the virus had spread to Nigeria. But since then, the virus has found its way out of Africa. The first major outbreak occurred on the island of Yap in Micronesia for 13 weeks 2007, during which 185 Zika cases were suspected (49 of those were confirmed, with another 59 considered probable). Then, in October 2013, an outbreak began in French Polynesia; around 10,000 cases were reported, less than 100 of which presented with severe neurological or autoimmune complications. One confirmed case of autochthonous transmission occurred in Chile in 2014, which means a person was infected while they were in Chile rather than somewhere else. Cases were also reported that year from several Pacific Islands. The virus was detected in Chile until June 2014, but then it seemed to disappear.
Fast forward to May 2015, when the Pan American Health Organization (PAHO) issued an alert regarding the first confirmed Zika virus infection in Brazil. Since then, several thousand suspected cases of the disease and a previously unknown complication—a kind of birth defect known as microcephaly where the baby’s brain is abnormally small—have been reported from Brazil. (It’s important to note that while the connection between the virus and microcephaly is strongly suspected, the link has yet to be conclusively demonstrated.)
The recent spread of the virus has been described as “explosive”; Zika has now been detected in 25 countries and territories. The rising concern over both the number of cases and reports of serious complications has led the most affected areas in Brazil to declare a state of emergency, and on Monday, The World Health Organization’s Director-General will convene an International Health Regulations Emergency Committee on Zika virus and the observed increase in neurological disorders and neonatal malformations. At this emergency meeting, the committee will discuss mitigation strategies and decide whether the organization will officially declare the virus a “Public Health Emergency of International Concern.”
GM to the Rescue
The mosquito to blame for the outbreak—Aedes aegypti—doesn’t belong in the Americas. It’s native to Africa, and was only introduced in the new world when Europeans began to explore the globe. In the 20th century, mosquito control programs nearly eradicated the unwelcome menace from the Americas (largely thanks to the use of the controversial pesticide DDT); as late as the mid 1970s, Brazil and 15 other nations were Aedes aegypti-free. But despite the successes, eradication efforts were halted, allowing the mosquito to regain its lost territory.
Effective control measures are expensive and difficult to maintain, so at the tail end of the 20th century and into the 21st, scientists began to explore creative means of controlling mosquito populations, including the use of genetic modification. Oxitec’s mosquitoes are one of the most exciting technologies to have emerged from this period. Here’s how they work, as I described in a post almost exactly a year ago:
While these mosquitoes are genetically modified, they aren’t “cross-bred with the herpes simplex virus and E. colibacteria” (that would be an interkingdom ménage à trois!)—and no, they cannot be “used to bite people and essentially make them immune to dengue fever and chikungunya” (they aren’t carrying a vaccine!). The mosquitoes that Oxitec have designed are what scientists call “autocidal” or possess a “dominant lethal genetic system,” which is mostly fancy wording for “they die all by themselves”. The males carry inserted DNA which causes the mosquitoes to depend upon a dietary supplement that is easy to provide in the lab, but not available in nature. When the so-called mutants breed with normal females, all of the offspring require the missing dietary supplement because the suicide genes passed on from the males are genetically dominant. Thus, the offspring die before they can become adults. The idea is, if you release enough such males in an area, then the females won’t have a choice but to mate with them. That will mean there will be few to no successful offspring in the next generation, and the population is effectively controlled.
Male mosquitoes don’t bite people, so they cannot serve as transmission vectors for Zika or any other disease. As for fears that GM females will take over: less than 5% of all offspring survive in the laboratory, and as Glen Slade, director of Oxitec’s Brazilian branch notes, those are the best possible conditions for survival. “It is considered unlikely that the survival rate is anywhere near that high in the harsher field conditions since offspring reaching adulthood will have been weakened by the self-limiting gene,” he told me. And contrary to what the conspiracy theorists claim, scientists have shown that tetracycline in the environment doesn’t increase that survival rate.
Brazil, a hotspot for dengue and other such diseases, is one of the countries where Oxitec is testing their mozzies—so far, everywhere that Oxitec’s mosquitoes have been released, the local populations have been suppressed by about 90%.
Wrong Place, Wrong Time
Now that we’ve covered the background on the situation, let’s dig into the conspiracy theory. We’ll start with the main argument laid out as evidence: that the Zika outbreak began in the same location at the same time as the first Oxitec release:
Though it’s often said, it’s worth repeating: correlation doesn’t equal causation. If it did, then Nicholas Cage is to blame for people drowning (Why, Nick? WHY?). But even beyond that, there are bigger problems with this supposed correlation: even by those maps, the site of release is on the fringe of the Zika hotspot, not the center of it. Just look at the two overlaid:
The epicenter of the outbreak and the release clearly don’t line up—the epicenter is on the coast rather than inland where the map points. Furthermore, the first confirmed cases weren’t reported in that area, but in the town of Camaçari, Bahia, which is—unsurprisingly—on the coast and several hundred kilometers from the release site indicated.
But perhaps more importantly, the location on the map isn’t where the mosquitoes were released. That map points to Juazeiro de Norte, Ceará, which is a solid 300 km away from Juazeiro, Bahia—the actual site of the mosquito trial. That location is even more on the edge of the Zika-affected area:
The mistake was made initially by the Redditor who proposed the conspiracy theory and has been propagated through lazy journalistic practices by every proponent since. Here’s a quick tip: if you’re basing your conspiracy theory on location coincidence, it’s probably a good idea to actually get the location right.
By July 2015, shortly after the GM mosquitoes were first released into the wild in Juazeiro, Brazil, Oxitec proudly announced they had “successfully controlled the Aedes aegypti mosquito that spreads dengue fever, chikungunya and zika virus, by reducing the target population by more than 90%.”
A new control effort employing Oxitec mosquitoes did begin in April 2015, but not in Juaziero, or any of the northeastern states of Brazil where the disease outbreak is occurring. As another press release from Oxitec states, the 2015 releases of their GM mosquitoes were in Piracicaba, São Paulo, Brazil:
Following approval by Brazil’s National Biosafety Committee (CTNBio) for releases throughout the country, Piracicaba’s CECAP/Eldorado district became the world’s first municipality to partner directly with Oxitec and in April 2015 started releasing its self-limiting mosquitoes whose offspring do not survive. By the end of the calendar year, results had already indicated a reduction in wild mosquito larvae by 82%. Oxitec’s efficacy trials across Brazil, Panama and the Cayman Islands all resulted in a greater than 90% suppression of the wild Ae. aegypti mosquito population–an unprecedented level of control.
Based on the positive results achieved to date, the ‘Friendly Aedes aegypti Project’ in CECAP/Eldorado district covering 5,000 people has been extended for another year. Additionally, Oxitec and Piracicaba have signed a letter of intent to expand the project to an area of 35,000-60,000 residents. This geographic region includes the city’s center and was chosen due to the large flow of people commuting between it and surrounding neighborhoods which may contribute to the spread of infestations and infections.
Piracicaba, for the record, is more than 1300 miles away from the Zika epicenter:
So not only did the conspiracy theorists get the location of the first Brazil release wrong, they either got the date wrong, too, or got the location of the 2015 releases really, really off. Either way, the central argument that the release of GM mosquitoes by Oxitec coincides with the first cases of Zika virus simply doesn’t hold up.
Scientists Speak Out
As this ludicrous conspiracy theory has spread, so, too, has the scientific opposition to it. “Frankly, I’m a little sick of this kind of anti-science platform,” said vector ecologist Tanjim Hossain from the University of Miami, when I asked him what he thought. “This kind of fear mongering is not only irresponsible, but may very well be downright harmful to vulnerable populations from a global health perspective.”
Despite the specious allusions made by proponents of the conspiracy, this is still not Jurassic Park, says Hossain.
“We have a problem where ZIKV is spreading rapidly and is widely suspected of causing serious health issues,” he continued. “How do we solve this problem? An Integrated Vector Management (IVM) approach is key. We need to use all available tools, old and new, to combat the problem. GM mosquitoes are a fairly new tool in our arsenal. The way I see it, they have the potential to quickly reduce a local population of vector mosquitoes to near zero, and thereby can also reduce the risk of disease transmission. This kind of strategy could be particularly useful in a disease outbreak ‘hotspot’ because you could hypothetically stop the disease in its tracks so to speak.”
Other scientists have shared similar sentiments. Alex Perkins, a biological science professor at Notre Dame, told Business Insider that rather than causing the outbreak, GM mosquitoes might be our best chance to fight it. “It could very well be the case that genetically modified mosquitos could end up being one of the most important tools that we have to combat Zika,” Perkins said. “If anything, we should potentially be looking into using these more.”
Brazilian authorities couldn’t be happier with the results so far, and are eager to continue to fight these deadly mosquitoes by any means they can. “The initial project in CECAP/Eldorado district clearly showed that the ‘friendly Aedes aegypti solution’ made a big difference for the inhabitants of the area, helping to protect them from the mosquito that transmits dengue, Zika and chikungunya,” said Pedro Mello, secretary of health in Piracicaba. He notes that during the 2014/2015 dengue season, before the trial there began, there were 133 cases of dengue. “In 2015/2016, after the beginning of the Friendly Aedes aegypti Project, we had only one case.”
It’s long past time to stop villainizing Oxitec’s mosquitoes for crimes they didn’t commit. Claire Bernish, The Daily MFail, Mirror and everyone else who has spread these baseless accusations: I’m talking to you. The original post was in the Conspiracy subreddit—what more of a red flag for “this is wildly inaccurate bullsh*t” do you need? (After all, if this is a legit source, where are your reports on the new hidden messages in the $100 bill? or why the Illuminati wants people to believe in aliens?). It’s well known that large-scale conspiracy theories are mathematically challenged. Don’t just post whatever crap is spewed on the internet because you know it’ll get you a few clicks. It’s dishonest, dangerous, and, frankly, deplorable to treat nonsense as possible truth just to prey upon your audience’s very real fears of an emerging disease. You, with your complete lack of integrity, are maggots feeding on the decay of modern journalism, and I mean that with no disrespect to maggots.
Pedro Venceslau e Fabio Leite – O Estado de S. Paulo
26 Fevereiro 2015 | 03h 00
Diretor disse em CPI que problema não colocaria usuário em risco; empresa também afirmou que pressão está fora da norma
SÃO PAULO – O risco de contaminação da água admitido nesta quarta-feira, 25, pelo diretor metropolitano da Companhia de Saneamento Básico do Estado de São Paulo (Sabesp), Paulo Massato, em caso de rodízio oficial já é realidade em algumas regiões altas da Grande São Paulo. São locais onde a rede fica despressurizada após o fechamento manual dos registros na rua, conforme um alto dirigente da empresa admitiu ao Estado no início do mês.
“Se implementado o rodízio, a rede fica despressurizada, principalmente em regiões de topografia acidentada, nos pontos em que a tubulação está em declive. Se o lençol freático está contaminado, isso aumenta o risco de contaminação (da água na rede)”, afirmou Massato, nesta quarta, durante sessão da CPI da Sabesp na Câmara Municipal.
O resultado desse contágio, segundo ele, não colocaria a vida dos consumidores em risco, mas poderia causar disenteria, por exemplo. “Nós temos hoje medicina suficiente para minimizar risco de vida para a população. Uma disenteria pode ser mais grave ou menos grave, mas é um risco (implementar o rodízio) que nós queremos evitar ”, completou. Apesar do alerta, ele disse que a estatal poderia “descontaminar” rapidamente a água afetada.
‘Estamos em uma situação de anormalidade. Nós não conseguiríamos abastecer 6 milhões de habitantes se mantivéssemos a normalidade’, disse Massato
No início do mês, um dirigente da Sabesp admitiu ao Estado que em 40% da rede onde não há válvulas redutoras de pressão (VRPs) instaladas, o racionamento de água é feito por meio do fechamento manual, flagrado pela reportagem na Vila Brasilândia, zona norte da capital. Segundo ele, a manobra “não esvazia totalmente” a rede, mas “despressuriza pontos mais altos”.
“A zona baixa fica com água. Se não houver consumo excessivo, a maior parte da rede fica com água. Acaba despressurizando zonas altas, isso acontece mesmo. Tanto é que quando abre (o registro) para encher de novo, as zonas mais altas e distantes acabam sofrendo mais, ficando mais tempo sem água”, afirmou.
Para o engenheiro Antonio Giansante, professor de Engenharia Hídrica do Mackenzie, é grande o risco de contaminação em caso de fechamento da rede. “Em uma eventualidade de o tubo estar seco, pode ser que entre água de qualidade não controlada, em geral, contaminada por causa das redes coletoras de esgoto, para dentro da rede da Sabesp.”
Segundo interlocutores do governador Geraldo Alckmin (PSDB), a declaração desagradou o tucano, uma vez que o rodízio não está descartado. Massato já havia causado constrangimento ao governo ao dizer, em 27 de janeiro, que São Paulo poderia ficar até cinco dias sem água por semana em caso de racionamento.
Fora da norma. Massato e o presidente da Sabesp, Jerson Kelman, que também prestou depoimento à CPI, admitiram aos vereadores que a empresa mantém a pressão da água na rede abaixo do recomendado pela Associação Brasileira de Normas Técnicas (ABNT), conforme o Estado revelou no início do mês. Segundo o órgão, são necessários ao menos 10 metros de coluna de água para encher todas as caixas.
“Nós estamos garantindo 1 metro da coluna de água, preservando a rede de distribuição. Mas não tem pressão suficiente para chegar na caixa d’água”, admitiu Massato. “Estamos abaixo dos 10 metros de coluna de água, principalmente nas zonas mais altas e mais distantes dos reservatórios.”
“Essa é uma medida mitigadora para evitar algo muito pior para a população, que é o rodízio”, afirmou Kelman. “São poucos pontos na rede em que não se tem a pressão exigida pela ABNT para condições normais. Isso não é uma opção da Sabesp. Não estamos em condições normais”, completou.
Em dezembro, Alckmin disse que a Sabesp cumpria “rigorosamente” a norma técnica. A Sabesp foi notificada pela Agência Reguladora de Saneamento e Energia do Estado de São Paulo (Arsesp) e respondeu na terça-feira aos questionamentos feitos sobre as manobras na rede. O órgão fiscalizador, contudo, ainda não se pronunciou.
Ar encanado. Questionados sobre a investigação do Ministério Público Estadual que apura suposta cobrança por “ar encanado” pela Sabesp, revelada pelo Estado, os dirigentes da empresa disseram que a prática atingiu apenas 2% dos clientes. Das 22 mil reclamações registradas em fevereiro sobre aumento indevido da conta, 500 culpavam o ar encanado. O problema ocorre quando a água retorna na rede e empurra o ar de volta para as ligações das casas, podendo adulterar a medição do hidrômetro. / COLABOROU RICARDO CHAPOLA
Summary: The Ebola virus disease epidemic already devastating swaths of West Africa will likely get far worse in the coming weeks and months unless international commitments are significantly and immediately increased, new research predicts.
The Ebola virus disease epidemic already devastating swaths of West Africa will likely get far worse in the coming weeks and months unless international commitments are significantly and immediately increased, new research led by Yale researchers predicts.
The findings are published in the Oct. 24 issue of The Lancet Infectious Diseases.
A team of seven scientists from Yale’s Schools of Public Health and Medicine and the Ministry of Health and Social Welfare in Liberia developed a mathematical transmission model of the viral disease and applied it to Liberia’s most populous county, Montserrado, an area already hard hit. The researchers determined that tens of thousands of new Ebola cases — and deaths — are likely by Dec. 15 if the epidemic continues on its present course.
“Our predictions highlight the rapidly closing window of opportunity for controlling the outbreak and averting a catastrophic toll of new Ebola cases and deaths in the coming months,” said Alison Galvani, professor of epidemiology at the School of Public Health and the paper’s senior author. “Although we might still be within the midst of what will ultimately be viewed as the early phase of the current outbreak, the possibility of averting calamitous repercussions from an initially delayed and insufficient response is quickly eroding.”
The model developed by Galvani and colleagues projects as many as 170,996 total reported and unreported cases of the disease, representing 12% of the overall population of some 1.38 million people, and 90,122 deaths in Montserrado alone by Dec. 15. Of these, the authors estimate 42,669 cases and 27,175 deaths will have been reported by that time.
Much of this suffering — some 97,940 cases of the disease — could be averted if the international community steps up control measures immediately, starting Oct. 31, the model predicts. This would require additional Ebola treatment center beds, a fivefold increase in the speed with which cases are detected, and allocation of protective kits to households of patients awaiting treatment center admission. The study predicts that, at best, just over half as many cases (53,957) can be averted if the interventions are delayed to Nov. 15. Had all of these measures been in place by Oct. 15, the model calculates that 137,432 cases in Montserrado could have been avoided.
There have been approximately 9,000 reported cases and 4,500 deaths from the disease in Liberia, Sierra Leone, and Guinea since the latest outbreak began with a case in a toddler in rural Guinea in December 2013. For the first time cases have been confirmed among health-care workers treating patients in the United States and parts of Europe.
“The current global health strategy is woefully inadequate to stop the current volatile Ebola epidemic,” co-author Dr. Frederick Altice, professor of internal medicine and public health added. “At a minimum, capable logisticians are needed to construct a sufficient number of Ebola treatment units in order to avoid the unnecessary deaths of tens, if not hundreds, of thousands of people.”
Other authors include lead author Joseph Lewnard, Martial L. Ndeffo Mbah, Jorge A. Alfaro-Murillo, Luke Bawo, and Tolbert G. Nyenswah.
The National Institutes of Health funded the study.
Journal Reference:
Joseph A Lewnard, Martial L Ndeffo Mbah, Jorge A Alfaro-Murillo, Frederick L Altice, Luke Bawo, Tolbert G Nyenswah, Alison P Galvani. Dynamics and control of Ebola virus transmission in Montserrado, Liberia: a mathematical modelling analysis. Lancet Infectious Diseases, October 24, 2014 DOI:10.1016/S1473-3099(14)70995-8
A epidemia já causou mais de 4,5 mil mortes na África Ocidental
A epidemia de ebola vai demorar pelo menos quatro meses para ser contida se todas as medidas necessárias forem tomadas, disse hoje (22) o responsável geral da Cruz Vermelha, Elhadj As Sy, alertando para “o preço da inação”. A epidemia já causou mais de 4,5 mil mortes na África Ocidental e os especialistas alertam que a taxa de infecção poderá chegar a 10 mil por semana no início de dezembro.
Ainda não há vacina aprovada para o ebola, que também atingiu profissionais da saúde na Espanha e nos Estados Unidos.
Elhadj As Sy listou uma série de medidas que poderiam ajudar a colocar o ebola sob controle, incluindo “um bom isolamento, bom tratamento dos casos confirmados, e bom, seguro e digno enterro às pessoas falecidas”. “Será possível, como era possível no passado, conter esta epidemia dentro de quatro a seis meses” se a resposta for adequada, acrescentou.
“Eu acho que esta é a nossa melhor perspectiva e nós estamos fazendo todo o possível para mobilizar nossos recursos e nossas capacidades para travar o surto”, destacou. As Sy, que falava em uma conferência da Cruz Vermelha da Ásia-Pacífico, acrescentou que “há sempre um preço pela inação”.
Novas medidas serão adotadas hoje nos Estados Unidos, entre as quais os voos dos países mais afetados – Libéria, Serra Leoa e Guiné-Conacri – serão encaminhados para cinco aeroportos e os passageiros passarão por exames mais completos de saúde.
Entretanto, especialistas que escrevem para a revista The Lancet, disseram, na terça-feira (21), que a triagem dos passageiros nos aeroportos de saída seria uma opção melhor do que monitorá-los no destino da viagem.
Photo: Boakai Fofana/allAfrica. A burial team carries the body of a suspected Ebola victim under the watchful eyes of police officers.
By Franklin Doloquee
Two Ebola patients, who died of the virus in separate communities in Nimba County have reportedly resurrected in the county. The victims, both females, believed to be in their 60s and 40s respectively, died of the Ebola virus recently in Hope Village Community and the Catholic Community in Ganta, Nimba.
But to the amazement of residents and onlookers on Monday, the deceased reportedly regained life in total disbelief. The New Dawn Nimba County correspondent said the late Dorris Quoi of Hope Village Community and the second victim only identified as Ma Kebeh, said to be in her late 60s, were about to be taken for burial when they resurrected.
Ma Kebeh had reportedly been in door for two nights without food and medication before her alleged death. Nimba County has had bizarre news of Ebola cases with a native doctor from the county, who claimed that he could cure infected victims, dying of the virus himself last week.
News of the resurrection of the two victims has reportedly created panic in residents of Hope Village Community and Ganta at large, with some citizens describing Dorris Quoi as a ghost, who shouldn’t live among them. Since the Ebola outbreak in Nimba County, this is the first incident of dead victims resurrecting.
Suspected Ebola patient Finda “Zanabo” prays over her sick family members before being admitted to the Doctors Without Borders Ebola treatment center on Aug. 21, 2014, near Monrovia, Liberia. Photo by John Moore/Getty Images
Its exponential growth: At this point, the number of people infected is doubling approximately every three weeks, leading some epidemiologists to projectbetween 77,000 and 277,000 cases by the end of 2014.
The gruesomeness with which it kills: by hijacking cells and migrating throughout the body to affect all organs, causing victims to bleed profusely.
The ease with which it is transmitted: through contact with bodily fluids, including sweat, tears, saliva, blood, urine, semen, etc., including objects that have come in contact with bodily fluids (such as bed sheets, clothing, and needles) and corpses.
The threat of mutation: Prominent figures have expressed serious concerns that this disease will go airborne, and there are many other mechanisms through which mutation might make it much more transmissible.
Terrifying as these factors are, it is not clear to me that any of them capture what is truly, horribly tragic about this disease.
The most striking thing about the virus is the way in which it propagates. True, through bodily fluids, but to suggest as much is to ignore the conditions under which bodily contact occurs. Instead, the mechanism Ebola exploits is far more insidious. This virus preys on care and love, piggybacking on the deepest, most distinctively human virtues. Affected parties are almost all medical professionals and family members, snared by Ebola while in the business of caring for their fellow humans. More strikingly, 75 percent of Ebola victims are women, people who do much of the care work throughout Africa and the rest of the world. In short, Ebola parasitizes our humanity.
More than most other pandemic diseases (malaria, cholera, plague, etc.) and more than airborne diseases (influenza, swine flu, H5N1, etc.) that are transmitted indiscriminately through the air, this disease is passed through very minute amounts of bodily fluid. Just a slip of contact with the infected party and the caregiver herself can be stricken.
If Ebola is not stopped, this disease can destroy whole families within a month, relatives of those families shortly thereafter, friends of those relatives after that, and on and on. As it takes hold (and it is taking hold fast), it cuts out the heart of family and civilization. More than the profuse bleeding and high kill rate, this is why the disease is terrifying. Ebola sunders the bonds that make us human.
Aid providers are now working fastidiously to sever these ties themselves, fighting hopelessly against the natural inclinations that people have to love and care for the ill. They have launched aggressive public information campaigns, distributedupdates widely, called for more equipment and gear, summoned the military, tried to rein in the hysteria, and so on. Yet no sheet of plastic or latex can disrupt these human inclinations.
Such heroic efforts are the appropriate medical response to a virulent public health catastrophe. The public health community is doing an incredible job, facing unbelievable risks, relying on extremely limited resources. Yet these efforts can only do half of the work. Infected parties—not all, to be sure, but some (enough)—cannot abide by the rules of disease isolation. Some will act without donning protective clothing. Some will assist without taking proper measures. And still others will refuse to enter isolation units because doing so means leaving their families and their loved ones behind, abandoning their humanity, and subjecting themselves to the terror of dying a sterile, lonely death.
It is tempting, at these times, to focus on the absurd and senseless actions of a few. One of the primary vectors in Sierra Leone is believed to have been a traditional healer who had been telling people that she could cure Ebola. In Monrovia a few weeks back, angry citizens stormed a clinic and removed patients from their care. “There is no Ebola!” they are reported to have been shouting. More recently, the largest newspaper in Liberia published an article suggesting that Ebola is a conspiracy of the United States, aimed to undermine Africa. And, perhaps even more sadly, a team of health workers and journalists was just brutally murdered in Guinea. It is easy, in other words, to blame the spread on stupidity, or illiteracy, or ritualism, or conspiracy theories, or any number of other irrational factors.
A man checks on a very sick Saah Exco, 10, in a back alley of the West Point slum on Aug. 19, 2014, in Monrovia, Liberia. Photo by John Moore/Getty Images
But imagine: You are a parent whose child has suddenly come ill with a fever. Do you cast your child away and refuse to touch him? Do you cover your face and your arms? Stay back! Unclean! Or do you comfort your child when he asks for you, arms outstretched, to make the pain go away?
Imagine: You live in a home with five other family members. Your sister falls ill, ostensibly from Ebola, but possibly from malaria, typhoid, yellow fever, or the flu. You are aware of the danger to yourself and your other family members, but you have no simple means to move her, and she is too weak to move herself. What do you do?
Imagine: You are a child of 5 years old. Your mother is sick. She implores you to back away. But you are scared. What you need, more than anything, is a hug and a cry.
Who can blame a person for this? It is a terrible, awful predicament. A moral predicament. To stay, comfort, and give love and care to those who are in desperate need, or to shuttle them off into an isolation ward, perhaps never to see them again? What an inhumane decision this is.
What makes the Ebola virus so terrifying is not its kill rate, its exponential growth, the gruesome way in which it kills, the ease of transmission, or the threat of mutation, but rather that people who care can do almost nothing but sit on the sidelines and watch.
* * *
Many have asked whether Ebola could come here, come West. (The implication, in its way, is crass—as if to suggest that we need not be concerned about a tragedy unless it poses a threat to us.) We have been reassured that it will never spread widely here, because our public health networks are too strong, our hospitals too well-stocked. The naysayers may be right about this. But they are not right that it does not pose a threat to us.
For starters, despite the pretense, the West is not immune from absurd, unscientific thinking. We have our fair share of scientific illiteracy, skepticism, ritualism, and foolishness. But beyond this, it is our similarities, not our differences, that make us vulnerable to this plague. We are human. Every mechanism we have for caring—touching, holding, feeding, playing, warming, comforting, caressing—every mechanism that we use to bind us to our families and our neighbors, is preyed upon by Ebola. We cannot seal each other into hyperbaric chambers and expect that once we emerge, the carnage will be over. We are humans, and we will care about our children and our families even if it means that we may die in doing so.
The lesson here is a vital one: People do not give up on humanity so very easily. Even if we persuade all of the population to forgo rituals like washing the dead, we will not easily persuade parents to keep from holding their sick children, children from clinging to their ailing parents, or children from playing and wrestling and slobbering all over one another. We tried to alter such behaviors with HIV/AIDS. A seemingly simple edict—“just lay off the sex with infected parties”—would seem all that is required to halt that disease. But we have learned over the decades that people do not give up sex so readily.
If you think curtailing sex is hard, love and compassion will be that much harder. Humans will never give this up—we cannot give this up, for it is fundamental to who we are. The more that medical personnel require this of people without also giving them methods to manifest care, the more care and compassion will manifest in pockets outside of quarantine. And the more humanity that manifests unchecked, the more space this virus has to grow. Unchecked humanity will seep through the cracks and barriers that we build to keep our families safe, and if left to find its own way, will carry a lethal payload.
The problem is double-edged. Ebola threatens humanity by preying on humanity. The seemingly simple solution is to destroy humanity ourselves—to seal everything off and let the disease burn out on its own. But doing so means destroying ourselves in order to save ourselves, which is no solution at all.
A medical worker in a protective suit works near Ebola patients in a Doctors Without Borders hospital on Sept. 7, 2014, in Monrovia, Liberia. Photo by Dominique Faget/AFP/Getty Images
We must find a method of caring without touching, of contacting without making contact. The physiological barriers are, for the time being, necessary. But we cannot stop people from caring about one another, so we must create, for the time being, mechanisms for caring. Since we will never be able to beat back humanity, we must coordinate humanity, at the family level, the local level, and the global level.
The only one way to battle a disease that affixes itself parasitically to our humanity is to overwhelm it with greater, stronger humanity. To immunize Africa and the rest of the world with a blast of humanity so powerful that the disease can no longer take root. What it will take to beat this virus is to turn its most powerful vehicle, our most powerful weapon, against it.
Here are some things we can do:
Donate to the great organizations that are working tirelessly to bring this disease under control. They need volunteers, medical supplies, facilities, transportation, food, etc. Share information about Ebola, so people will learn about it, know about it, and know how to address it when it comes. And inform and help others. It is natural at a time of crisis to call for sealing the borders, to build fences and walls that separate us further from outside threats. But a disease that infects humanity cannot easily be walled off in this way. Walling off just creates unprotected pockets of humanity, divisions between us and them: my family, your family; that village, this village; inside, outside.
* * *
One final thing.
When Prince Prospero, ill-fated protagonist of Edgar Allan Poe’s story “The Masque of the Red Death,” locked himself in his castle to avoid a contagion that was sweeping his country—a disease that caused “profuse bleeding at the pores”—he assumed mistakenly that the only reasonable solution to his problem was to remove himself from the scene. For months he lived lavishly, surrounded by courtiers, improvisatori, buffoons, musicians, and wine, removed from danger while the pestilence wrought havoc outside.
As with much of Poe’s writing, Prospero’s tale does not end well. For six months, all was calm. He and his courtiers enjoyed their lives, secure and isolated from the plague laying waste to the countryside. Then, one night during a masquerade ball, the Red Death snuck into the castle, hidden behind a mask and a cloak, to afflict Prospero and his revelers, dropping them one by one in the “blood-bedewed halls.” Prospero’s security was a façade, leaving darkness and decay to hold “illimitable dominion over all.” The eventual intrusion that would be his undoing foretells of a danger in believing that we can keep the world’s ills at bay by keeping our distance.
If we seek safety by shutting out the rest of the world, we are in for a brutally ugly awakening. Nature is a cruel mistress, but Ebola is her cruelest, most devious trick yet.











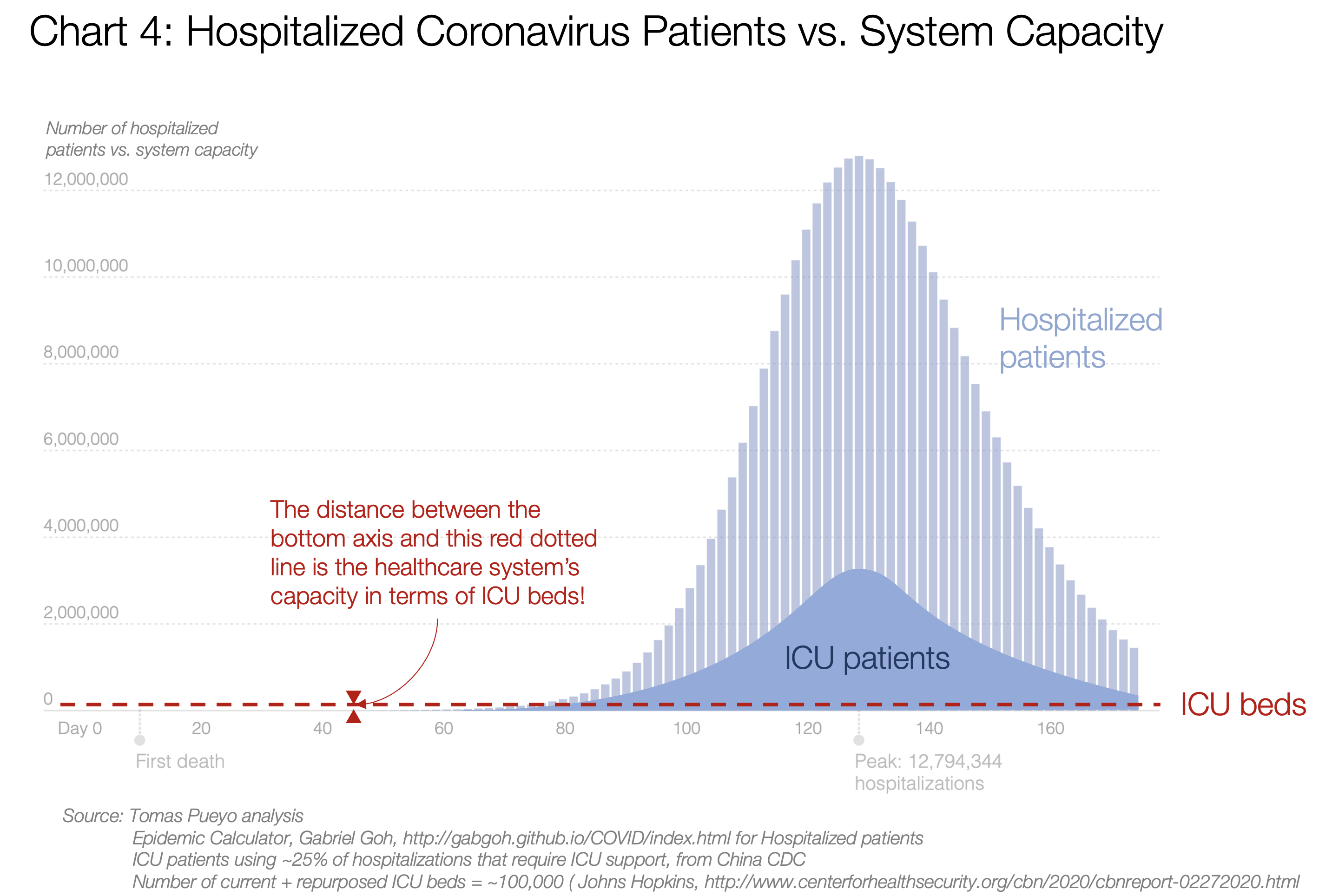

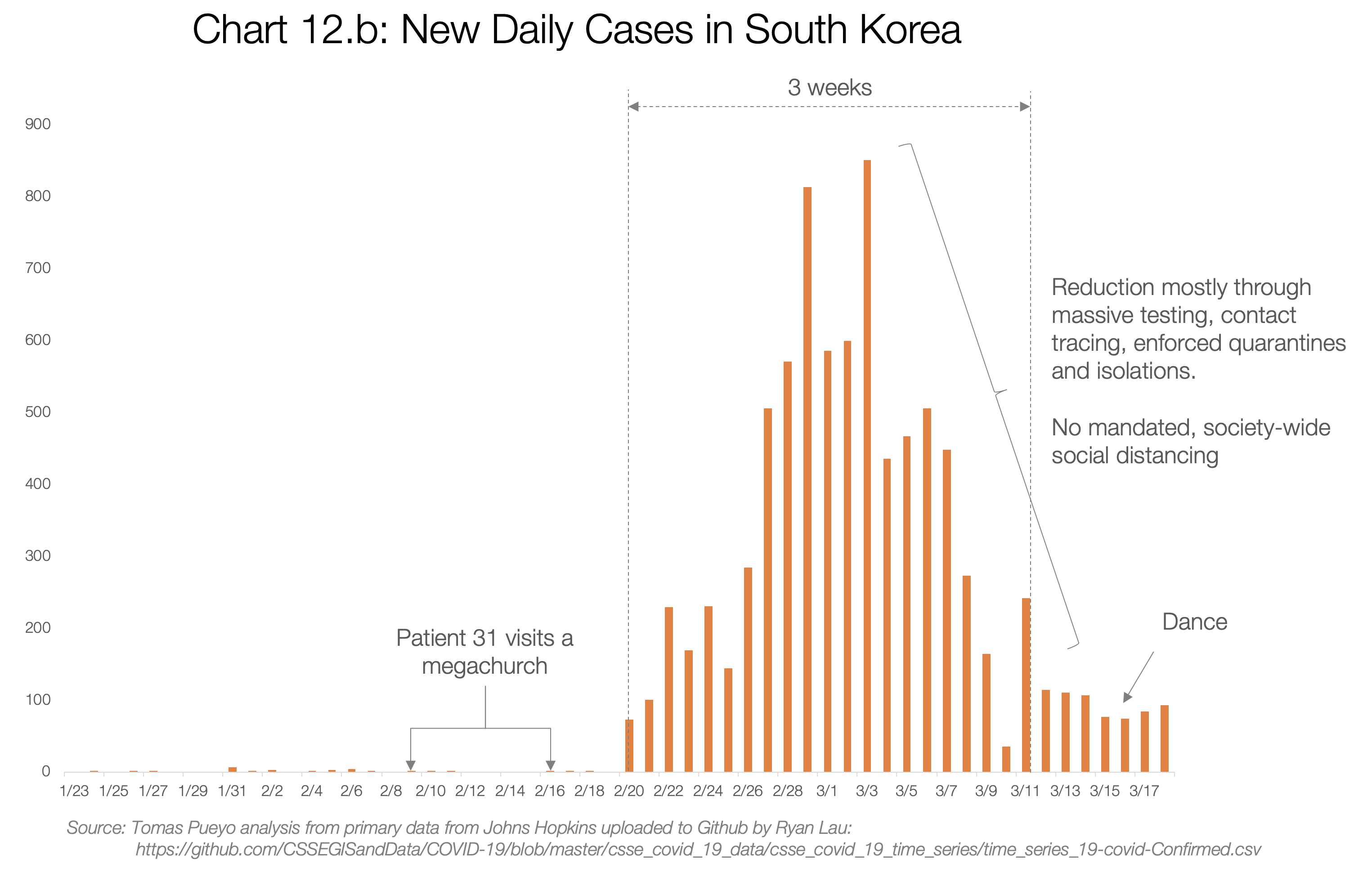
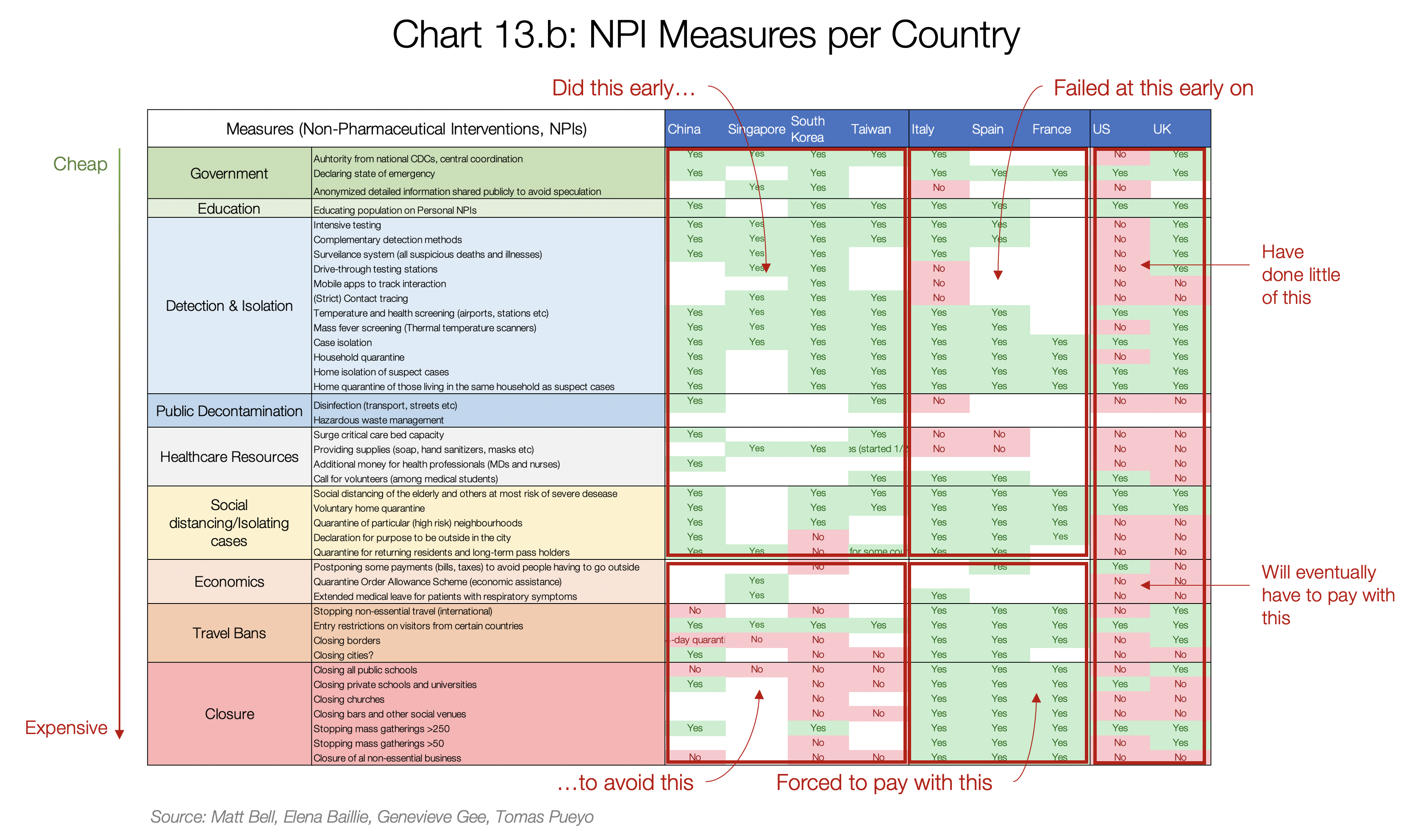

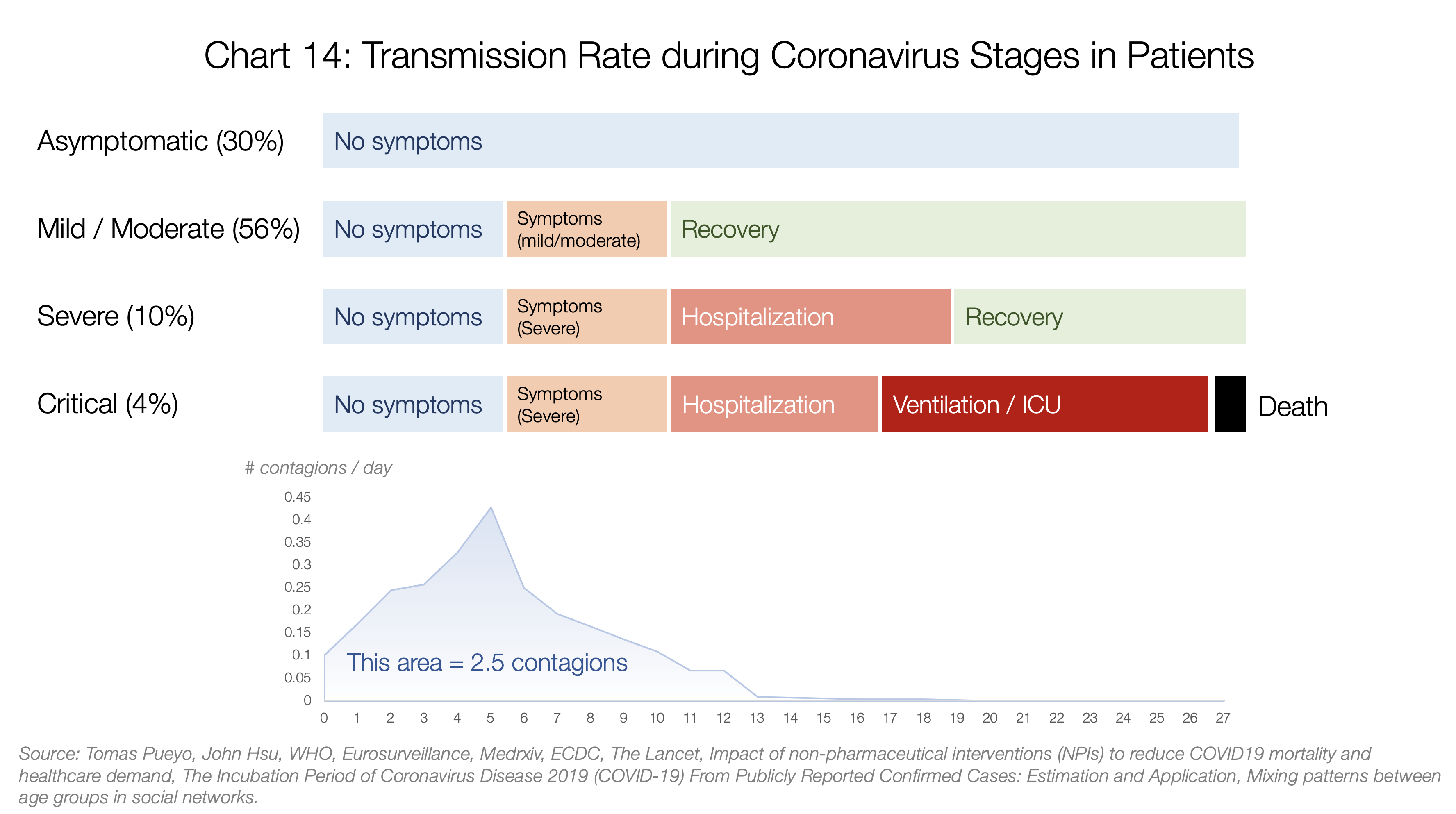
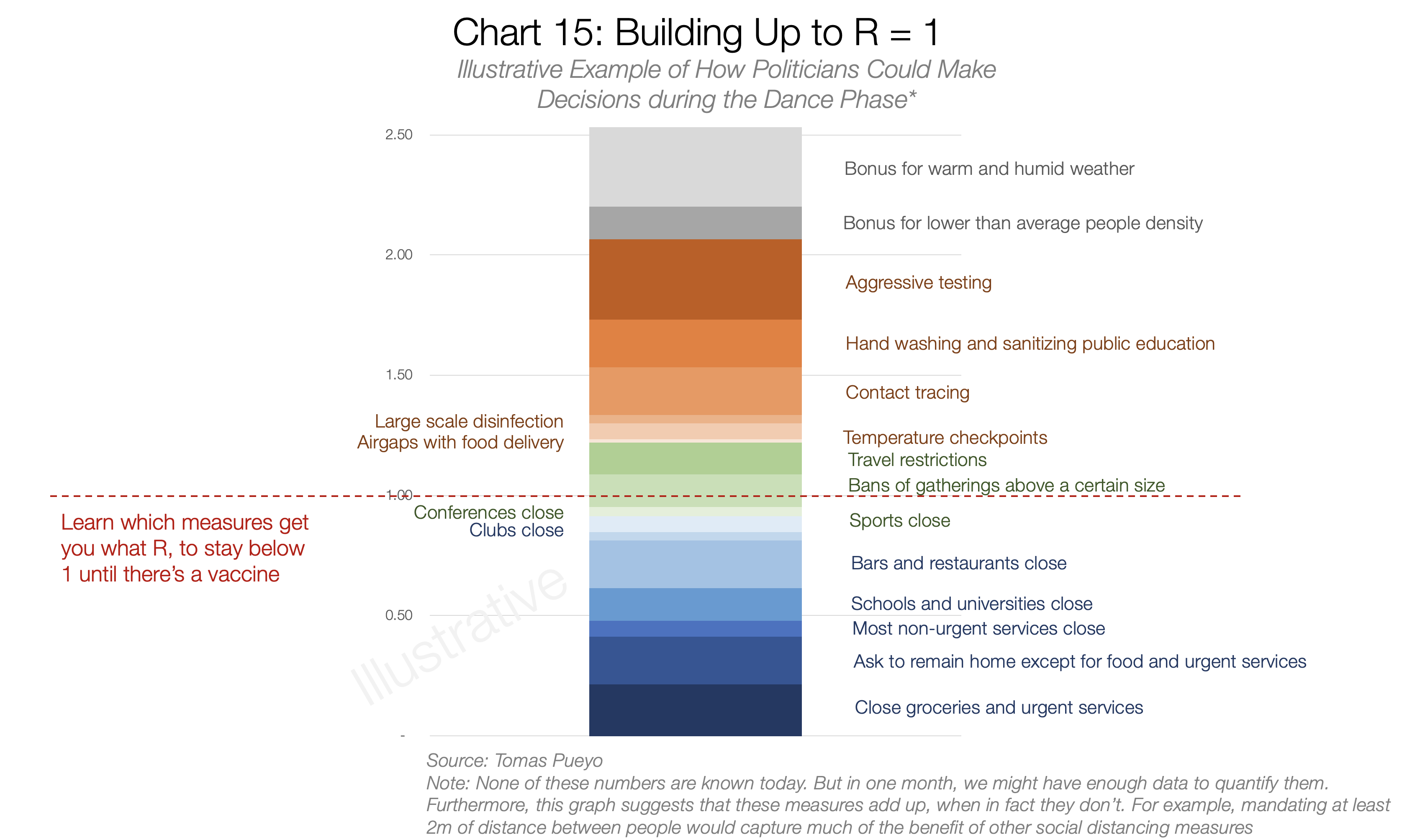














 Suspected Ebola patient Finda “Zanabo” prays over her sick family members before being admitted to the Doctors Without Borders Ebola treatment center on Aug. 21, 2014, near Monrovia, Liberia. Photo by John Moore/Getty Images
Suspected Ebola patient Finda “Zanabo” prays over her sick family members before being admitted to the Doctors Without Borders Ebola treatment center on Aug. 21, 2014, near Monrovia, Liberia. Photo by John Moore/Getty Images A man checks on a very sick Saah Exco, 10, in a back alley of the West Point slum on Aug. 19, 2014, in Monrovia, Liberia. Photo by John Moore/Getty Images
A man checks on a very sick Saah Exco, 10, in a back alley of the West Point slum on Aug. 19, 2014, in Monrovia, Liberia. Photo by John Moore/Getty Images A medical worker in a protective suit works near Ebola patients in a Doctors Without Borders hospital on Sept. 7, 2014, in Monrovia, Liberia. Photo by Dominique Faget/AFP/Getty Images
A medical worker in a protective suit works near Ebola patients in a Doctors Without Borders hospital on Sept. 7, 2014, in Monrovia, Liberia. Photo by Dominique Faget/AFP/Getty Images