It was late fall of 2022 when David Stallknecht heard that bodies were raining from the sky.
Stallknecht, a wildlife biologist at the University of Georgia, was already fearing the worst. For months, wood ducks had been washing up on shorelines; black vultures had been teetering out of tree tops. But now thousands of ghostly white snow-goose carcasses were strewn across agricultural fields in Louisiana, Missouri, and Arkansas. The birds had tried to take flight, only to plunge back to the ground. “People were saying they were literally dropping down dead,” Stallknecht told me. Even before he and his team began testing specimens in the lab, they suspected they knew what they would find: yet another crop of casualties from the deadly strain of avian influenza that had been tearing across North America for roughly a year.
Months later, the bird-flu outbreak continues to rage. An estimated 58.4 million domestic birds have died in the United States alone. Farms with known outbreaks have had to cull their chickens en masse, sending the cost of eggs soaring; zoos have herded their birds indoors to shield them from encounters with infected waterfowl. The virus has been steadily trickling into mammalian populations—foxes, bears, mink, whales, seals—on both land and sea, fueling fears that humans could be next. Scientists maintain that the risk of sustained spread among people is very low, but each additional detection of the virus in something warm-blooded and furry hints that the virus is improving its ability to infiltrate new hosts. “Every time that happens, it’s another chance for that virus to make the changes that it needs,” says Richard Webby, a virologist at St. Jude Children’s Research Hospital. “Right now, this virus is a kid in a candy store.”
A human epidemic, though, remains a gloomy forecast that may not come to pass. In the meantime, the outbreak has already been larger, faster-moving, and more devastating to North America’s wildlife than any other in recorded history, and has not yet shown signs of stopping. “I would use just one word to describe it: unprecedented,” says Shayan Sharif, an avian immunologist at Ontario Veterinary College. “We have never seen anything like this before.” This strain of bird flu is unlikely to be our next pandemic. But a flu pandemic has already begun for countless other creatures—and it could alter North America’s biodiversity for good.
Deadly strains of avian flu have been ferried onto North American shores multiple times before, and rapidly petered out. That was the case in 2014, when a highly virulent version of the virus crossed the Pacific from Asia and invaded U.S. poultry farms, forcing workers to exterminate millions of chickens and turkeys. The brutal interventions worked: “They did all the right things, and nipped it in the bud,” says Nicole Nemeth, a veterinary pathologist at the University of Georgia. Hardly any wild birds were affected; egg prices bumped up briefly, then settled back roughly to baseline. “It just kind of died down,” Nemeth told me. “And everyone breathed a sigh of relief.”
Some birds are likely to make it through the outbreak just fine. For as long as humans have been aware of this particular strain of avian influenza, scientifically classed as H5N1, the virus has been relatively gentle on certain types of waterfowl, especially mallards, pintails, and other so-called dabbling ducks. “Some populations have a prevalence as high as 40 percent, and they’re as normal as normal could be,” Stallknecht said. Those same species have also been some of avian flu’s best chauffeurs in the past, silently spreading the feces-borne infection across countries and continents during their seasonal migrations.
Others haven’t been so lucky. Some of the same respiratory issues that strike humans who have the flu—sneezing, coughing, pneumonia when the disease gets severe—can hit birds, too. But across a variety of susceptible species, necropsies show more extensive damage, with evidence of virus in various organs, including the liver, gut, and brain. The neurologic problems can be among the worst: Swans might swim in listless circles; geese might waddle shakily onto shores, their necks twisted and turned; eagles might flap defeatedly from their perches, unable to launch themselves into the air. Michelle Hawkins, a veterinarian at UC Davis, told me that several of the red-tailed hawks she’s treated in her clinic have arrived with their eyes shaking so vigorously from side to side that the spasms turn the animals’ head; others appear to gaze off into nothingness, unresponsive even when humans approach.
Death can come swiftly—sometimes within a day or two of the infection’s start. Birds simply keel over as if they’ve been shot, their bodies dropping like rocks. On poultry farms, outbreaks can wipe out entire flocks in just two or three days. In wilder settings, locals have spotted bald eagles plummeting out of their nests, leaving shrieking chicks behind. By the time infected birds reach Hawkins in her clinic, “they’re usually almost dead,” she told me. “And we can’t figure out how to help them except to put them out of their misery.” Hawkins estimated that in the past few months alone, her team’s euthanasia rate has gone up by about 50 percent.
Mammals so far haven’t fared much better. Last spring, the corpse of a dolphin infected with the virus was found wedged into a canal in Florida—around the same time that Wisconsin locals happened upon litters of ailing fox kits, drooling, twitching, and struggling to stand in the hours before they seized and died. In the fall, three young, flu-stricken grizzlies in Montana were euthanized after researchers noticed that the disoriented animals had begun to go blind. Wendy Puryear, a molecular virologist at Tufts University, told me that seals sick with the virus will sometimes convulse so badly that they can barely hold their bodies straight. Every seal she’s seen that tested positive has ended up dead within days. This month, researchers in Peru reported that they were picking up the virus in some of the sea lions that have died by the hundreds along the country’s coast; a similar situation may now be playing out among a number of Scotland’s seals.
It’s hard to say why this outbreak is so much worse than the ones that came before. Microbial evolution may be one culprit: Flu viruses are particularly inclined to tweak their RNA code; when two genetically distinct versions of the pathogens wind up in the same cell, they can also swap bits of their genomes. This iteration of H5N1 may be particularly adept at sparking lethal disease—something Justin Brown, a veterinary pathologist at Penn State, thinks is quite likely, given how many animals have died. It may also be more easily exiting birds’ bodies in feces, or more efficiently entering cells in the airway or gut. “This particular virus seems to be better adapted to wild birds. I think that’s the key thing,” Stallknecht told me. As climate change alters migration schedules, and pushes certain avian species into more frequent contact with one another’s contaminated scat, the risks of intermingling are only growing. The greater the number of infections, the more animals will die. “It becomes a numbers game,” Stallknecht said.
Flu viruses have never had much trouble spreading: They can be breathed out or defecated; they can persist on surfaces for hours, and in cool waters for days. But Webby suspects that the ballooning of this epidemic can be at least partly blamed on the severity of disease. “The easiest birds to catch are the ones that are sick,” he told me. Hawks, eagles, owls, and other predatory birds may be stumbling across dying ducks and eating them, unwittingly infecting themselves. Nemeth thinks that certain species, including black vultures, are now cutting out the middlebird and feasting on the carcasses of their own kin as they continue to die in droves. “They see dead tissue, they’re going to eat it,” she told me. It’s a morbid tragedy of abundance, as the virus climbs the food chain to reach species it hasn’t easily accessed before. “The biggest impact is on these atypical hosts,” Webby told me, which lack the prior exposures to the virus that might have helped protect them.
Predation or scavenging of sick or dead birds is probably how certain mammals—grizzlies, foxes, opossums, and the like—are catching the virus too. The seals and dolphins present a bit more of a puzzle, Puryear told me, though it’s possible to guess at what’s at play. At least some types of seals have been documented consuming birds; other marine mammals might simply be gulping feces-infested water. A recent avian-flu outbreak at a mink farm in Spain suggests a more troubling mode of transmission: mammals repeatedly conveying the virus to one another—a possible first for H5N1. “That is really disconcerting,” Sharif told me. “It tells me the virus is adapting to mammals.”
Animals vulnerable to the virus don’t have many good options for protection. Some avian-flu vaccines have been used on certain poultry farms, mostly abroad. But some of the same issues that plague human-flu vaccines are obstacles in the bird world too, Brown told me: The ingredients of the shots aren’t always good matches for the circulating virus, and the immunizations, which may be pretty good at staving off severe disease, don’t do much to block infection or transmission, making outbreaks tough to contain. Wild birds, which can’t be corralled and immunized en masse, are essentially out of luck. Nemeth told me that some of her colleagues in Florida have been trying to clear the ground of carcasses so that they won’t become sources of infection for yet another unlucky mammal or bird. “But they just can’t keep up with the number of deaths,” she said. Essentially all avian species are thought to be susceptible to infection—and there’s simply no way to reach every bird, says Becky Poulson, an avian-flu researcher at the University of Georgia. After hopscotching across the globe for decades, H5N1 now seems very likely to be in North America for good, “part of the new normal here,” Poulson told me.
Experts told me they’re hopeful that the outbreak will abate before long. But even if that happens, some species may not live to see it. North America’s birds already face a medley of threats—chemical pollution, window collisions, habitat destruction, roving colonies of feral cats—and some of them cannot sustain another blow. “This could be the last nail in the coffin for some species,” says Min Huang, who leads the migratory-bird program at Connecticut’s Department of Energy and Environmental Protection.
The current epidemic “may not be directly affecting us, in that almost none of us are getting sick,” says Kishana Taylor, a virologist at Rutgers University. But the extent of its reach into wildlife means that humans will still notice its many impacts. In a world with fewer birds, other animals—such as coyotes, snakes, and even humans—might go hungrier, while the fish, insects, and rats that birds eat could experience population booms. The treetops and shorelines, once alive with song, could go silent; far fewer seeds might be dispersed. The U.S.’s national bird—one of the country’s few conservation success stories—could once again find itself pushed to the brink. Some locals in the Southeast have already told Nemeth that they’re feeling the absence of vultures, as roadside deer carcasses begin to fester in the sun. The bird pandemic will have its survivors. But they are likely to be living in a world that is quieter, lonelier, and harsher than it was before.
Climate change is already killing people, but countries don’t have an easy way to count those deaths. A new project might change that.
Climate change can kill people in all kinds of ways. There are the obvious ones—wildfires, storms, and floods—yet rising temperatures may also lead to the increased spread of deadly diseases, make food harder to come by, and increase the risk of conflict.
Although we know about these wide-ranging but equally terrifying risks, attempts to pinpoint the number of deaths caused by climate change have been piecemeal. One recent study estimated that climate change was to blame for 37 percent of heat-related deaths over the past three decades. In 2021, Daniel Bressler, a PhD student at Columbia University in New York, estimated that every additional 4,400 metric tons of carbon dioxide emitted will cause one heat-related death later this century. He called this number the “mortality cost of carbon.”
Putting a number on climate deaths isn’t just an academic exercise. People are already dying because of extreme temperature and weather events, and we can expect this to become more common as the planet continues to heat up. If governments want to put in place policies to prevent these deaths, they need a way of accurately measuring the deaths and ill health linked to warming. The search is on for the true mortality cost of carbon.
As part of this search, the UK government has made its first attempt at putting a number on climate change deaths. The UK Office for National Statistics (ONS)—an independent government agency responsible for producing official data—has for the first time reported climate-related deaths and hospital admissions in England and Wales. The report covers the years 2001 to 2020, but future reports will be released annually, revealing for the first time detailed information about the impact that climate change is having on health in the two nations. (Statistics for Scotland and Northern Ireland are recorded separately.)
The main finding from this investigation is counterintuitive. The report found that the number of deaths associated with warm or cold temperatures actually decreased between 2001 and 2020. On average, 27,755 fewer people were dying each year due to unusually warm or cold temperatures. In other words, climate change might have actually prevented over half a million deaths in England and Wales over this period. In 2001 there were 993 climate-related deaths per 100,000 people in England and Wales. By 2019 that figure had fallen to 771.
But let’s not get ahead of ourselves. There are a number of reasons why the net number of temperature-related deaths appeared to decline over this period, says Myer Glickman, head of the epidemiological, climate, and global health team at the ONS. For a start, statisticians took a relatively narrow definition of climate-related deaths. They only included deaths from conditions where scientists had previously found a clear link between temperature and disease outcome, and they also excluded any health condition where their own analysis showed no link between temperature and outcome. This means that the mortality data doesn’t include deaths from violence or natural forces (such as storms, landslides, or flooding).
The analysis also excluded deaths from air pollution, which Public Health England estimates is equivalent to between 28,000 and 36,000 deaths each year in the UK. Glickman says that there is no accepted way to separate out the effect that temperature increases have on air pollution. Add all these caveats together and it’s likely that the ONS analysis is a little on the conservative side.
Then there is the big reason why climate change has not led to more deaths in England and Wales: the very mild climate. Although average temperatures in the UK have increased by 0.9 degrees compared to the period from 1961 to 1990, its residents are not some of the 3 billion people who face unlivable conditions if greenhouse gas emissions increase rapidly. And while deaths linked to cold weather were down in England and Wales, on warmer days there was a net increase in hospital admissions linked to warmer weather. This was particularly true when it comes to injuries, which may be because more people do outdoor activities when it’s warmer or might be linked to the increases in violence and mental health problems that are associated with warmer temperatures.
The lower rate of deaths might also be a sign that our attempts to fight back against cold weather are working. Widespread flu vaccinations, support for people to pay their heating bills, and increases in home insulation mean that the coldest days didn’t hit as hard as they might have without these mitigations in place, Glickman says. And warmer homes might be a good thing now, but as summers in the UK get hotter and air-conditioning remains rare, it may start to become a problem.
The ONS will now release this data on a yearly basis, but Glickman’s next project is to look more closely at how temperature changes affected different areas. “We’re going to drill down to a local level temperature,” he says. “That’s going to give us a lot more resolution on what’s happening and who it’s happening to.” The impact of climate change might depend on how wealthy an area is, for example, or whether its residents have easy access to health care or community support.
Glickman also wants to explore indirect impacts of climate on health. “What will be a big interest in the coming years is the lower-level health impacts of things like flooding,” he says. If someone’s home is flooded, it might increase their vulnerability to respiratory disease or worsen their mental health. Researchers from the UK have already found that people with mental illnesses are more at risk of death during hot weather. We don’t know why that is exactly, but researchers think it might be because people with mental illnesses are more likely to be socially isolated or already have poorer health, which makes them more vulnerable when temperatures rise.
The team behind the ONS report are also part of a wider effort to create a global system to count climate-related health impacts. “What we don’t have is a robust set of statistics to categorize the impact of climate on health,” says Bilal Mateen, a senior manager of digital technology at Wellcome Trust, the health charity funding the new climate change health impact initiative.
The first year of the project will be spent identifying countries to partner with before developing and testing different ways of measuring climate change deaths that work for specific countries, says Mateen. The idea is to use this data to help countries devise policies that lessen the health impact of climate change. “We can begin to tease out what works, what doesn’t, and what adaptation and mitigation interventions we should be supporting,” Mateen says.
If it’s true that warmer homes and flu vaccines helped reduce climate change deaths in England and Wales, it’s a sign that populations that are healthier on the whole might be better at surviving the ravages of a heating world. Other countries may want to take note. “All policies are health policies,” says Mateen. “There is a clear need to support job stability, to address fuel poverty and every other policy that’s outside of the mandate of the health minister, because we know that those social determinants of health have downstream impact.”
Last summer, a doctor wrote “climate change” in his patient’s chart. But is medicine really ready to address systemic health impacts?
Last June, a heat dome settled over British Columbia, shattering the region’s heat records for five consecutive days and hitting temperatures of over 120 degrees. The dome was responsible for at least 500 human deaths (and potentially a billion marine creature casualties) and stretched the health systems in the region to their breaking point.
And at one rural hospital in Nelson, British Columbia, doctor Kyle Merritt began to feel like there was more he should do than simply treat all the patients coming in with heat stroke and exhaustion. “I was upset with what I was seeing,” he says, “I felt like it should be documented in some way.” So when a 70-year-old woman arrived with heat stroke, he wrote “climate change” in her medical chart as the underlying reason she had to be admitted to the hospital.
It was the first and only time Merritt chose to include “climate change” as an underlying condition in a patient’s chart. “It was the first patient that I felt like it was really clear cut,” he says. Had the conditions outside not been so extreme, he might have been able to discharge her and let her recover at home. When we spoke, Merritt emphasized that it was a decision he made in the heat of the moment. He never expected it to become national news.
Months later, when speaking with the founders of a small organization called Doctors for Planetary Health, Merritt shared the story of his decision to write “climate change” in the patient’s chart. When they asked to use that story in a press release accompanying a planned climate rally, Merritt didn’t think anyone was going to read the press release about this little thing that happened.
But read it they did. Eventually, Merritt’s story was all over the news, often under erroneous headlines claiming he had “diagnosed” a patient with climate change (the phrase appears in her chart as an underlying cause, not a diagnosis). The story was covered by national publications like NBC News, The Hill, The Daily Mail, along with a host of right-wing news sites like GOP USA.
Some praised the decision for bringing necessary awareness to the connection between climate change and health. “When I saw this, I thought, ‘Yes, this is what we need. We need more attention to the social determinants of health,’” says Keisha Ray, an assistant professor at the McGovern Center for Humanities and Ethics at UTHealth. Others claimed this was “the latest example of team-left lunacy.” Some columnists argued, incorrectly, that the patient probably didn’t get proper treatment because her doctor “diagnosed her” with something incurable. (Merritt admitted the patient to the emergency room and she was treated for her condition.)
When I read the story, my question was less about Merritt and more about the patient herself. Did she know she was the center of this news blip? Had he talked to her about climate change, or the fact that he was writing it in her chart? Did she give permission to be in the press release? And what are the ethics of turning a patient into a public point?
Doctors use case studies all the time to communicate with one another, and with the press. And for good reason: People connect with and remember stories far better than generalized facts. But using a patient to explain a concept, or to help educate doctors on how to treat someone more effectively, is different from using a patient’s story to make this broader, public point about climate and health. Even Merritt admitted that writing “climate change” in this woman’s chart didn’t do much to help her or other patients suffering during the heat dome. “It’s not like some other doctor was going to look at it and make sure they were never exposed to climate change,” he says. “Practically speaking, it doesn’t really do that much.”
Medicine has a checkered history when it comes to using patient stories and protecting privacy. For decades, doctors paraded patients in front of the public without their consent. In 1906, for example, a famous doctor named Wilfred Grenfell published the story of a 9-year-old boy who had accidentally shot himself in the knee. Grenfell used the boy’s full name, image, and identity, telling the tale with gusto each time he spoke to the public and his colleagues—even distorting the facts of the case, turning “slight” bleeding in the original chart into “shocking” bleeding and a “heterogeneous mass of bloody rags”—in order to entertain donors, make himself seem more heroic, and maintain his status as a celebrity doctor. Fast forward to today, and issues of patient privacy are still very present. In 2012 the ABC show NY Med, which at the time starred celebrity doctor Mehmet Oz, broadcast the death of a patient without his family’s consent. His widow won $2.2 million in a suit against the hospital.
Given that history, the question of how much to anonymize a patient in these tales is well-trod territory for medical ethicists. “As long as the physician doesn’t give any kind of identifying information, then it would be ethical. You want to always maintain the patient’s privacy,” says Ray. “But you also have to think about how minor information can be pieced together, where someone can figure out who this patient is.”
In Merritt’s case, the details provided to the press go like this: We know the patient’s age, her background medical conditions, the type of home she lives in, and that she was admitted in June. Kootenay Medical Center, where Merritt works, serves less than 4,000 patients. “That’s a lot of identifying information,” Ray said, when I told her the facts that had been publicly confirmed. “Small towns don’t tend to have a lot of physicians, so you could very well be one of three physicians.”
This feels increasingly important when a story is used in a way that might be construed as political —calling for action on something like racism or climate change. In a world where private citizens can be outed and harassed for being associated with a cause or a side, doctors who want to use a patient’s sickness to make an activist point might need to be a little more cautious. “I worry that the sensationalism of this story may encourage people like journalists to go seek this patient out,” says Ray. “And I also worry that because climate change is still very political and it still is considered a left-leaning idea, that it may encourage conservative media to go and find this person and pit them against each other.”
That hasn’t happened in this case. But Merritt says that if he were to do it over, he might have done things differently. As it unfolded, he didn’t tell the patient he was writing “climate change” in her chart. In fact, they didn’t discuss climate change at all. “If I had known when I had written that in the chart that it was something that I was doing to try and tell the story, I don’t know. I may have talked to the patient more about it and asked their permission,” he says. “But of course, at that time when I did it, I had no idea that it would ever become a story of any kind.” To this day, Merritt believes that the patient has no idea she is the one in the story.
Beyond the specifics of Merritt and his patient, the story raises big questions about how medicine can and should handle systemic impacts on health.
Merritt wrote “climate change” in a bout of frustration, wanting to document what he was seeing in real time. Other doctors have taken different approaches. Nyasha Spears, a physician at St. Luke’s Hospital in Duluth, Minnesota, takes nearly the opposite tack that Merritt did—rather than quietly writing in a chart to make a broader point, she talks to her patients constantly about climate change and the environment. “As a family doctor, my jam is habit change. This is what I do,” she says. “So my thought with climate change is, can I start peppering my conversations with patients all the time with an argument that habit change is good for them on a personal level, but also good for the environment?”
In the case of Merritt’s patient, this talk might not have done much. There was nothing she could do about her conditions, no habit change she could make to avoid the scorching heat. Like many in her community, she likely couldn’t afford to install air-conditioning in her trailer, and beyond that there was little to be done. In cases like these, Ray says that maybe a climate change talk isn’t warranted. “They can feel helpless because there’s nothing that they can do,” she says. “They are literally living, and just living is making them sick.”
This reality can make things feel bleak for both doctors and patients. And to address these connections between health and structural conditions like climate change and racism, doctors will need to ask not simply what they can do for each individual patient, but also what they can change about medicine to account for and reckon with these links. Today, there is no diagnostic code for climate change, no way to link these cases up or track them in any way, but perhaps there should be.
“There’s all sorts of ICD-10 codes that are completely inane,” says Spears. “If you ever want to entertain yourself, you just start looking at ICD 10 codes. ‘Fall from a spacecraft’ is one. And so it would make perfect sense that there would be an ICD-10 code for climate change illness.” Being able to track these additional, systemic determinants of health could make it easier to prove the links, and do something about them.
Having more data doesn’t always mean making change—the impact that race and income have on health have been well proven for years, but still haven’t adequately been addressed. And Ray says that adding these codes shouldn’t stop with climate. “If you live in a poor area, then you are likely living with more environmental impacts. Are we going to start now having a code for low income? Is there going to be a code for: You don’t have enough money to live in a safe home and so you are experiencing environmental toxins? Is improper housing also going to be coded? So I just wonder how far we are willing to take it.”
This might be the silver lining in the story of Merritt’s patient. When we spoke, he told me he had recently gotten an email from Health Canada, asking to talk to him about creating a diagnostic code for climate change that doctors could use to track these impacts.
Writing “climate change” in one patient’s chart isn’t going to save the world, or even a single life—Merritt is the first to admit that—but it can start a conversation about how much the medical system is willing to adapt to the threats that its patients truly face. “I’ve learned a lot about how big of an impact a story can make,” he says.
New antibody and antiviral treatments, and better vaccines, are on the way
The Economist – Nov 8th 2021
IN THE WELL-VACCINATED wealthier countries of the world, year three of the pandemic will be better than year two, and covid-19 will have much less impact on health and everyday activities. Vaccines have weakened the link between cases and deaths in countries such as Britain and Israel (see chart). But in countries that are poorer, less well vaccinated or both, the deleterious effects of the virus will linger. A disparity of outcomes between rich and poor countries will emerge. The Gates Foundation, one of the world’s largest charities, predicts that average incomes will return to their pre-pandemic levels in 90% of advanced economies, compared with only a third of low- and middle-income economies.
Although the supply of vaccines surged in the last quarter of 2021, many countries will remain under-vaccinated for much of 2022, as a result of distribution difficulties and vaccine hesitancy. This will lead to higher rates of death and illness and weaker economic recoveries. The “last mile” problem of vaccine delivery will become painfully apparent as health workers carry vaccines into the planet’s poorest and most remote places. But complaints about unequal distribution will start to abate during 2022 as access to patients’ arms becomes a larger limiting factor than access to jabs. Indeed, if manufacturers do not scale back vaccine production there will be a glut by the second half of the year, predicts Airfinity, a provider of life-sciences data.
Booster jabs will be more widely used in 2022 as countries develop an understanding of when they are needed. New variants will also drive uptake, says Stanley Plotkin of the University of Pennsylvania, inventor of the rubella vaccine. Dr Plotkin says current vaccines and tweaked versions will be used as boosters, enhancing protection against variants.
The vaccination of children will also expand, in some countries to those as young as six months. Where vaccine hesitancy makes it hard for governments to reach their targets they will be inclined to make life difficult for the unvaccinated—by requiring vaccine passports to attend certain venues, and making vaccination compulsory for groups such as health-care workers.
Immunity and treatments may be widespread enough by mid-2022 to drive down case numbers and reduce the risk of new variants. At this point, the virus will become endemic in many countries. But although existing vaccines may be able to suppress the virus, new ones are needed to cut transmission.
Stephane Bancel, the boss of Moderna, a maker of vaccines based on mRNA technology, says his firm is working on a “multivalent” vaccine that will protect against more than one variant of covid-19. Beyond that he is looking at a “pan-respiratory” vaccine combining protection against multiple coronaviruses, respiratory viruses and strains of influenza.
Other innovations in covid-19 vaccines will include freeze-dried formulations of mRNA jabs, and vaccines that are given via skin patches or inhalation. Freeze-dried mRNA vaccines are easy to transport. As the supply of vaccines grows in 2022, those based on mRNA will be increasingly preferred, because they offer higher levels of protection. That will crimp the global market for less effective vaccines, such as the Chinese ones.
In rich countries there will also be greater focus on antibody treatments for people infected with covid-19. America, Britain and other countries will rely more on cocktails such as those from Regeneron or AstraZeneca.
Most promising of all are new antiviral drugs. Pfizer is already manufacturing “significant quantities” of its protease inhibitor. In America, the government has agreed to buy 1.2bn courses of an antiviral drug being developed by Merck, known as molnupiravir. This has shown its efficacy in trials, and the company has licensed it for widespread, affordable production.
There are many other antivirals in the pipeline. Antiviral drugs that can be taken in pill form, after diagnosis, are likely to become blockbusters in 2022, helping make covid-19 an ever more treatable disease. That will lead, in turn, to new concerns about unequal access and of misuse fostering resistant strains.
The greatest risk to this more optimistic outlook is the emergence of a new variant capable of evading the protection provided by existing vaccines. The coronavirus remains a formidable foe.
Natasha Loder: Health-policy editor, The Economist■
This article appeared in the Science and Technology section of the print edition of The World Ahead 2022 under the headline “From pandemic to endemic”
But the taming of the coronavirus conceals failures in public health
The Economist – Nov 8th 2021
PANDEMICS DO NOT die—they fade away. And that is what covid-19 is likely to do in 2022. True, there will be local and seasonal flare-ups, especially in chronically undervaccinated countries. Epidemiologists will also need to watch out for new variants that might be capable of outflanking the immunity provided by vaccines. Even so, over the coming years, as covid settles into its fate as an endemic disease, like flu or the common cold, life in most of the world is likely to return to normal—at least, the post-pandemic normal.
Behind this prospect lie both a stunning success and a depressing failure. The success is that very large numbers of people have been vaccinated and that, at each stage of infection from mild symptoms to intensive care, new medicines can now greatly reduce the risk of death. It is easy to take for granted, but the rapid creation and licensing of so many vaccines and treatments for a new disease is a scientific triumph.
The polio vaccine took 20 years to go from early trials to its first American licence. By the end of 2021, just two years after SARS-CoV-2 was first identified, the world was turning out roughly 1.5bn doses of covid vaccine each month. Airfinity, a life-sciences data firm, predicts that by the end of June 2022 a total of 25bn doses could have been produced. At a summit in September President Joe Biden called for 70% of the world to be fully vaccinated within a year. Supply need not be a constraint.
Immunity has been acquired at a terrible cost
Vaccines do not offer complete protection, however, especially among the elderly. Yet here, too, medical science has risen to the challenge. For example, early symptoms can be treated with molnupiravir, a twice-daily antiviral pill that in trials cut deaths and admissions to hospital by half. The gravely ill can receive dexamethasone, a cheap corticosteroid, which reduces the risk of death by 20-30%. In between are drugs like remdesivir and an antibody cocktail made by Regeneron.
Think of the combination of vaccination and treatment as a series of walls, each of which blocks a proportion of viral attacks from becoming fatal. The erection of each new wall further reduces the lethality of covid.
However, alongside this success is that failure. One further reason why covid will do less harm in the future is that it has already done so much in the past. Very large numbers of people are protected from current variants of covid only because they have already been infected. And many more, particularly in the developing world, will remain unprotected by vaccines or medicines long into 2022.
This immunity has been acquired at terrible cost. The Economist has tracked excess deaths during the pandemic—the mortality over and above what you would have expected in a normal year. Our central estimate on October 22nd was of a global total of 16.5m deaths (with a range from 10.2m to 19.2m), which was 3.3 times larger than the official count. Working backwards using assumptions about the share of fatal infections, a very rough estimate suggests that these deaths are the result of 1.5bn-3.6bn infections—six to 15 times the recorded number.
The combination of infection and vaccination explains why in, say, Britain in the autumn, you could detect antibodies to covid in 93% of adults. People are liable to re-infection, as Britain shows, but with each exposure to the virus the immune system becomes better trained to repel it. Along with new treatments and the fact that more young people are being infected, that explains why the fatality rate in Britain is now only a tenth of what it was at the start of 2021. Other countries will also follow that trajectory on the road to endemicity.
All this could yet be upended by a dangerous new variant. The virus is constantly mutating and the more of it there is in circulation, the greater the chance that an infectious new strain will emerge. However, even if Omicron and Rho variants strike, they may be no more deadly than Delta is. In addition, existing treatments are likely to remain effective, and vaccines can rapidly be tweaked to take account of the virus’s mutations.
Just another endemic disease
Increasingly, therefore, people will die from covid because they are elderly or infirm, or they are unvaccinated or cannot afford medicines. Sometimes people will remain vulnerable because they refuse to have a jab when offered one—a failure of health education. But vaccine doses are also being hoarded by rich countries, and getting needles into arms in poor and remote places is hard. Livelihoods will be ruined and lives lost all for lack of a safe injection that costs just a few dollars.
Covid is not done yet. But by 2023, it will no longer be a life-threatening disease for most people in the developed world. It will still pose a deadly danger to billions in the poor world. But the same is, sadly, true of many other conditions. Covid will be well on the way to becoming just another disease.
Edward Carr: Deputy editor, The Economist■
This article appeared in the Leaders section of the print edition of The World Ahead 2022 under the headline “Burning out”
O Harvard Global Health Institute e o Center for Climate, Health, and the Global Environment, da escola de saúde pública de Harvard, reuniram pesquisadores para analisar a literatura científica disponível até o momento e apontar caminhos para prevenção de novas pandemias.
Um dos pontos citados diretamente pelo relatório é o desmatamento. Os cientistas apontam como exemplo o aumento, após processos de desmate na América Central, de roedores como reservatórios de hantavírus —que, em caso de contaminação de humanos, pode levar à síndrome pulmonar por hantavírus.
A expansão de áreas agricultáveis também está ligada ao surgimento de novas doenças. Isso ocorre, afirmam os pesquisadores, pelo potencial de tal ação aproximar humanos a rebanhos de animais silvestres.
“Cerca de 22% da área terrestre em hotspots de biodiversidade, muitas vezes sobrepostos a hotspots de doenças emergentes, é ameaçada por expansão agrícola”, afirma o documento.
O relatório aponta que processos de urbanização descontrolados e sem planejamento podem ter um papel no surgimento de doenças, pelas mudanças no uso de terra e por possíveis grandes concentrações de pessoas e condições de vida ruins.
Há ainda fazendas de animais como outro ponto importante em eventos de spillover, ou transbordamento, em tradução do inglês, de zoonoses —basicamente, quando um vírus salta de uma espécie para uma nova, como para humanos. Os pesquisadores apontam a baixa diversidade genética e o elevado número de animais mantidos em alguns desses locais.
Os cientistas dão como exemplo a transmissão —inicialmente entre suínos e depois para trabalhadores agrícolas— do vírus nipah, na Malásia, em fazendas de porcos com altas concentrações de animais.
Além disso, a caça, o consumo e o comércio de animais selvagens também podem provocar o spillover.
A crise climática é mais um fator que deve impactar nos riscos de aparecimento de novas doenças no mundo, considerando as alterações que ocorrerão em ecossistemas. Segundo os pesquisadores, existe a possibilidade de habitats adequados para espécies diminuírem, o que poderia promover mais encontros entre vida selvagem e humanos, e, com isso, mais eventos de spillover.
“A redução de habitats e disponibilidade de néctar para morcegos, por exemplo, têm pressionado esses animais a buscar fontes alternativas de alimento em áreas urbanas e arredores”, afirmam os cientistas no relatório.
Por fim, os pesquisadores convocados por Harvard apontam estratégias para evitar eventos de spillover. A conservação ambiental é a primeira a ser destacada no relatório.
Outras estratégias listadas são restrições ao consumo de animais selvagens, investigações sobre vírus na vida selvagem e uma rede global de vigilância de patógenos em humanos, animais criados para abate e vida silvestre, entre outras iniciativas.
Segundo o documento, são baixos os investimentos destinados a impedir spillover. “Não mais do que US$ 4 bilhões [R$ 21,5 bilhões] são gastos a cada ano em todo o mundo em atividades de prevenção de transbordamento. A Covid-19 sozinha resultou em uma perda de PIB global estimada em US$ 4 trilhões [R$ 21,5 trilhões], ou cerca de US$ 40 bilhões [R$ 215 bilhões] por ano durante um século”, aponta o relatório.
Jonathan R Goodman, The Conversation – 13 May 2021
A major debate during the pandemic, and in infectious disease research more broadly, is why infected people die. No virus “wants” to kill anyone, as an epidemiologist once said to me. Like any other form of life, a virus’s goal is only to survive and reproduce.
A growing body of evidence instead suggests that the human immune system – which the science writer Ed Yong says is “where intuition goes to die” – may itself be responsible for many people’s deaths.
In an effort to find and kill the invading virus, the body can harm major organs, including the lungs and heart. This has led some doctors to focus on attenuating an infected patient’s immune response to help save them.
This brings up an evolutionary puzzle: what’s the point of the immune system if its overzealousness can kill the same people it evolved to defend?
The answer may lie in humanity’s evolutionary history: immunity may be as much about communication and behavior as it is about cellular biology. And to the degree that researchers can understand these broad origins of the immune system, they may be better positioned to improve responses to it.
The concept of the behavioral immune system is not new. Almost all humans sometimes feel disgust or revulsion – usually because whatever has made us feel that way poses a threat to our health.
And we aren’t alone in these reactions. Research shows that some animals avoid others that are showing symptoms of illness.
Eliciting care
However, more recent theoretical research suggests something more: humans, in particular, are likely to show compassion to those showing symptoms of illness or injury.
There’s a reason, this thinking goes, why people tend to exclaim when in pain, rather than just silently pull away from whatever is hurting them, and why fevers are linked to sluggish behavior.
Some psychologists argue that this is because immune responses are as much about communication as they are about self-maintenance. People who received care, over humanity’s history, probably tended to do better than those who tried to survive on their own.
In the broader evolutionary literature, researchers refer to these kinds of displays as “signals”. And like many of the innumerable signals we see across the natural world, immune-related signals can be used – or faked – to exploit the world around us, and each other.
Some birds, for example, feign injury to distract predators from their nests; rats suppress disease symptoms so that potential mates won’t ignore them.
We also see many illustrations of immune-signal use and misuse in human cultures. In The Adventure of the Dying Detective(1913), for example, Sherlock Holmes starves himself for three days to elicit a confession from a murder suspect. The suspect confesses only when he is convinced that his attempt to infect Holmes with a rare disease has been successful, misreading Holmes’s signs of illness.
This is an extreme example, but people feign signals of pain or illness all the time to avoid obligations, to elicit support from others, or even to avoid submitting an article by an agreed deadline. And this is an essential element of any signalling system.
Once a signal, be it a wince or a jaundiced complexion, elicits a response from whoever sees it, that response will start to drive how and why the signal is used.
Even germs use – and abuse – immune signals for their own gain. In fact, some virusesactually hijack our own immune responses, such as coughs and sneezes, to pass themselves on to new hosts, using our own evolved functions to further their interests.
Other germs, like SARS-CoV-2 (the virus that causes COVID-19) and Yersinia pestis (the bacterium that causes plague), can prevent our signalling to others when we are sick and pass themselves on without anyone realizing.
This perspective of immunity – one that takes into account biology, behavior and the social effects of illness – paints a starkly different picture from the more traditional view of the immune system as a collection of biological and chemical defenses against sickness.
Germs use different strategies, just as animals do, to exploit immune signals for their own purposes. And perhaps that’s what has made asymptomatically transmitted COVID-19 so damaging: people can’t rely on reading other people’s immune signals to protect themselves.
Insofar as doctors can predict how a particular infection – whether SARS-CoV-2, influenza, malaria or the next pathogen with pandemic potential – will interact with a patient’s immune system, they’ll be better positioned to tailor treatments for it. Future research will help us sort through the germs that hijack our immune signals – or suppress them – for their own purposes.
Viewing immunity not just as biological, but as a broader signalling system, may help us to understand our complex relationships with pathogens more effectively.
Our model reveals the true course of the pandemic. Here is what to do next
May 15th 2021 8-10 minutos
THIS WEEK we publish our estimate of the true death toll from covid-19. It tells the real story of the pandemic. But it also contains an urgent warning. Unless vaccine supplies reach poorer countries, the tragic scenes now unfolding in India risk being repeated elsewhere. Millions more will die.
Using known data on 121 variables, from recorded deaths to demography, we have built a pattern of correlations that lets us fill in gaps where numbers are lacking. Our model suggests that covid-19 has already claimed 7.1m-12.7m lives. Our central estimate is that 10m people have died who would otherwise be living. This tally of “excess deaths” is over three times the official count, which nevertheless is the basis for most statistics on the disease, including fatality rates and cross-country comparisons.
The most important insight from our work is that covid-19 has been harder on the poor than anyone knew. Official figures suggest that the pandemic has struck in waves, and that the United States and Europe have been hit hard. Although South America has been ravaged, the rest of the developing world seemed to get off lightly.
Our modelling tells another story. When you count all the bodies, you see that the pandemic has spread remorselessly from the rich, connected world to poorer, more isolated places. As it has done so, the global daily death rate has climbed steeply.
Death rates have been very high in some rich countries, but the overwhelming majority of the 6.7m or so deaths that nobody counted were in poor and middle-income ones. In Romania and Iran excess deaths are more than double the number officially put down to covid-19. In Egypt they are 13 times as big. In America the difference is 7.1%.
India, where about 20,000 are dying every day, is not an outlier. Our figures suggest that, in terms of deaths as a share of population, Peru’s pandemic has been 2.5 times worse than India’s. The disease is working its way through Nepal and Pakistan. Infectious variants spread faster and, because of the tyranny of exponential growth, overwhelm health-care systems and fill mortuaries even if the virus is no more lethal.
Ultimately the way to stop this is vaccination. As an example of collaboration and pioneering science, covid-19 vaccines rank with the Apollo space programme. Within just a year of the virus being discovered, people could be protected from severe disease and death. Hundreds of millions of them have benefited.
However, in the short run vaccines will fuel the divide between rich and poor. Soon, the only people to die from covid-19 in rich countries will be exceptionally frail or exceptionally unlucky, as well as those who have spurned the chance to be vaccinated. In poorer countries, by contrast, most people will have no choice. They will remain unprotected for many months or years.
The world cannot rest while people perish for want of a jab costing as little as $4 for a two-dose course. It is hard to think of a better use of resources than vaccination. Economists’ central estimate for the direct value of a course is $2,900—if you include factors like long covid and the effect of impaired education, the total is much bigger. The benefit from an extra 1bn doses supplied by July would be worth hundreds of billions of dollars. Less circulating virus means less mutation, and so a lower chance of a new variant that reinfects the vaccinated.
Supplies of vaccines are already growing. By the end of April, according to Airfinity, an analytics firm, vaccine-makers produced 1.7bn doses, 700m more than the end of March and ten times more than January. Before the pandemic, annual global vaccine capacity was roughly 3.5bn doses. The latest estimates are that total output in 2021 will be almost 11bn. Some in the industry predict a global surplus in 2022.
And yet the world is right to strive to get more doses in more arms sooner. Hence President Joe Biden has proposed waiving intellectual-property claims on covid-19 vaccines. Many experts argue that, because some manufacturing capacity is going begging, millions more doses might become available if patent-owners shared their secrets, including in countries that today are at the back of the queue. World-trade rules allow for a waiver. When invoke them if not in the throes of a pandemic?
We believe that Mr Biden is wrong. A waiver may signal that his administration cares about the world, but it is at best an empty gesture and at worst a cynical one.
A waiver will do nothing to fill the urgent shortfall of doses in 2021. The head of the World Trade Organisation, the forum where it will be thrashed out, warns there may be no vote until December. Technology transfer would take six months or so to complete even if it started today. With the new mRNA vaccines made by Pfizer and Moderna, it may take longer. Supposing the tech transfer was faster than that, experienced vaccine-makers would be unavailable for hire and makers could not obtain inputs from suppliers whose order books are already bursting. Pfizer’s vaccine requires 280 inputs from suppliers in 19 countries. No firm can recreate that in a hurry.
In any case, vaccine-makers do not appear to be hoarding their technology—otherwise output would not be increasing so fast. They have struck 214 technology-transfer agreements, an unprecedented number. They are not price-gouging: money is not the constraint on vaccination. Poor countries are not being priced out of the market: their vaccines are coming through COVAX, a global distribution scheme funded by donors.
In the longer term, the effect of a waiver is unpredictable. Perhaps it will indeed lead to technology being transferred to poor countries; more likely, though, it will cause harm by disrupting supply chains, wasting resources and, ultimately, deterring innovation. Whatever the case, if vaccines are nearing a surplus in 2022, the cavalry will arrive too late.
A needle in time
If Mr Biden really wants to make a difference, he can donate vaccine right now through COVAX. Rich countries over-ordered because they did not know which vaccines would work. Britain has ordered more than nine doses for each adult, Canada more than 13. These will be urgently needed elsewhere. It is wrong to put teenagers, who have a minuscule risk of dying from covid-19, before the elderly and health-care workers in poor countries. The rich world should not stockpile boosters to cover the population many times over on the off-chance that they may be needed. In the next six months, this could yield billions of doses of vaccine.
Countries can also improve supply chains. The Serum Institute, an Indian vaccine-maker, has struggled to get parts such as filters from America because exports were gummed up by the Defence Production Act (DPA), which puts suppliers on a war-footing. Mr Biden authorised a one-off release, but he should be focusing the DPA on supplying the world instead. And better use needs to be made of finished vaccine. In some poor countries, vaccine languishes unused because of hesitancy and chaotic organisation. It makes sense to prioritise getting one shot into every vulnerable arm, before setting about the second.
Our model is not predictive. However it does suggest that some parts of the world are particularly vulnerable—one example is South-East Asia, home to over 650m people, which has so far been spared mass fatalities for no obvious reason. Covid-19 has not yet run its course. But vaccines have created the chance to save millions of lives. The world must not squander it. ■
Ecosystems with a diversity of mammals, including larger-bodies and longer lived creatures like foxes, are better for our health. Credit: Ali Rajabali / Flickr
A growing body of evidence suggests that biodiversity loss increases our exposure to both new and established zoonotic pathogens. Restoring and protecting nature is essential to preventing future pandemics. So reports a new Proceedings of the National Academy of Sciences (PNAS) paper that synthesizes current understanding about how biodiversity affects human health and provides recommendations for future research to guide management.
Lead author Felicia Keesing is a professor at Bard College and a Visiting Scientist at Cary Institute of Ecosystem Studies. She explains, “There’s a persistent myth that wild areas with high levels of biodiversity are hotspots for disease. More animal diversity must equal more dangerous pathogens. But this turns out to be wrong. Biodiversity isn’t a threat to us, it’s actually protecting us from the species most likely to make us sick.”
Zoonotic diseases like COVID-19, SARS, and Ebola are caused by pathogens that are shared between humans and other vertebrate animals. But animal species differ in their ability to pass along pathogens that make us sick.
Rick Ostfeld is a disease ecologist at Cary Institute and a co-author on the paper. He explains, “Research is mounting that species that thrive in developed and degraded landscapes are often much more efficient at harboring pathogens and transmitting them to people. In less-disturbed landscapes with more animal diversity, these risky reservoirs are less abundant and biodiversity has a protective effect.”
Rodents, bats, primates, cloven-hooved mammals like sheep and deer, and carnivores have been flagged as the mammal taxa most likely to transmit pathogens to humans. Keesing and Ostfeld note, “The next emerging pathogen is far more likely to come from a rat than a rhino.”
This is because animals with fast life histories tend to be more efficient at transmitting pathogens. Keesing explains, “Animals that live fast, die young, and have early sexual maturity with lots of offspring tend to invest less in their adaptive immune responses. They are often better at transmitting diseases, compared to longer-lived animals with stronger adaptive immunity.”
When biodiversity is lost from ecological communities, long-lived, larger-bodied species tend to disappear first, while smaller-bodied species with fast life histories tend to proliferate. Research has found that mammal hosts of zoonotic viruses are less likely to be species of conservation concern (i.e. they are more common), and that for both mammals and birds, human development tends to increase the abundance of zoonotic host species, bringing people and risky animals closer together.
“When we erode biodiversity, we favor species that are more likely to be zoonotic hosts, increasing our risk of spillover events,” Ostfeld notes. Adding that, “Managing this risk will require a better understanding of how things like habitat conversion, climate change, and overharvesting affect zoonotic hosts, and how restoring biodiversity to degraded areas might reduce their abundance.”
To predict and prevent spillover, Keesing and Ostfeld highlight the need to focus on host attributes associated with disease transmission rather than continuing to debate the prime importance of one taxon or another. Ostfeld explains, “We should stop assuming that there is a single animal source for each emerging pathogen. The pathogens that jump from animals to people tend to be found in many animal species, not just one. They’re jumpers, after all, and they typically move between species readily.”
Disentangling the characteristics of effective zoonotic hosts – such as their immune strategies, resilience to disturbance, and habitat preferences – is key to protecting public health. Forecasting the locations where these species thrive, and where pathogen transmission and emergence are likely, can guide targeted interventions.
Keesing notes, “Restoration of biodiversity is an important frontier in the management of zoonotic disease risk. Those pathogens that do spill over to infect humans–zoonotic pathogens–often proliferate as a result of human impacts.” Concluding, “As we rebuild our communities after COVID-19, we need to have firmly in mind that one of our best strategies to prevent future pandemics is to protect, preserve, and restore biodiversity.”
Reference: “Impacts of biodiversity and biodiversity loss on zoonotic diseases” by Felicia Keesing and Richard S. Ostfeld, 5 April 2021, Proceedings of National Academy of Sciences. DOI: 10.1073/pnas.2023540118
This research was supported by a National Science Foundation Grant OPUS 1948419 to Keesing.
Cary Institute of Ecosystem Studies is an independent nonprofit center for environmental research. Since 1983, our scientists have been investigating the complex interactions that govern the natural world and the impacts of climate change on these systems. Our findings lead to more effective management and policy actions and increased environmental literacy. Staff are global experts in the ecology of: cities, disease, forests, and freshwater.
This week, the C.D.C. acknowledged what scientists have been saying for months: The risk of catching the coronavirus from surfaces is low.
Credit: Celeste Noche for The New York Times
April 8, 2021
When the coronavirus began to spread in the United States last spring, many experts warned of the danger posed by surfaces. Researchers reported that the virus could survive for days on plastic or stainless steel, and the Centers for Disease Control and Prevention advised that if someone touched one of these contaminated surfaces — and then touched their eyes, nose or mouth — they could become infected.
Americans responded in kind, wiping down groceries, quarantining mail and clearing drugstore shelves of Clorox wipes. Facebook closed two of its offices for a “deep cleaning.” New York’s Metropolitan Transportation Authority began disinfecting subway cars every night.
“People can be affected with the virus that causes Covid-19 through contact with contaminated surfaces and objects,” Dr. Rochelle Walensky, the director of the C.D.C., said at a White House briefing on Monday. “However, evidence has demonstrated that the risk by this route of infection of transmission is actually low.”
The admission is long overdue, scientists say.
“Finally,” said Linsey Marr, an expert on airborne viruses at Virginia Tech. “We’ve known this for a long time and yet people are still focusing so much on surface cleaning.” She added, “There’s really no evidence that anyone has ever gotten Covid-19 by touching a contaminated surface.”
During the early days of the pandemic, many experts believed that the virus spread primarily through large respiratory droplets. These droplets are too heavy to travel long distances through the air but can fall onto objects and surfaces.
In this context, a focus on scrubbing down every surface seemed to make sense. “Surface cleaning is more familiar,” Dr. Marr said. “We know how to do it. You can see people doing it, you see the clean surface. And so I think it makes people feel safer.”
Credit: Hiroko Masuike/The New York Times
But over the last year, it has become increasingly clear that the virus spreads primarily through the air — in both large and small droplets, which can remain aloft longer — and that scouring door handles and subway seats does little to keep people safe.
“The scientific basis for all this concern about surfaces is very slim — slim to none,” said Emanuel Goldman, a microbiologist at Rutgers University, who wrote last summer that the risk of surface transmission had been overblown. “This is a virus you get by breathing. It’s not a virus you get by touching.”
The C.D.C. has previously acknowledged that surfaces are not the primary way that the virus spreads. But the agency’s statements this week went further.
“The most important part of this update is that they’re clearly communicating to the public the correct, low risk from surfaces, which is not a message that has been clearly communicated for the past year,” said Joseph Allen, a building safety expert at the Harvard T.H. Chan School of Public Health.
Catching the virus from surfaces remains theoretically possible, he noted. But it requires many things to go wrong: a lot of fresh, infectious viral particles to be deposited on a surface, and then for a relatively large quantity of them to be quickly transferred to someone’s hand and then to their face. “Presence on a surface does not equal risk,” Dr. Allen said.
In most cases, cleaning with simple soap and water — in addition to hand-washing and mask-wearing — is enough to keep the odds of surface transmission low, the C.D.C.’s updated cleaning guidelines say. In most everyday scenarios and environments, people do not need to use chemical disinfectants, the agency notes.
“What this does very usefully, I think, is tell us what we don’t need to do,” said Donald Milton, an aerosol scientist at the University of Maryland. “Doing a lot of spraying and misting of chemicals isn’t helpful.”
Still, the guidelines do suggest that if someone who has Covid-19 has been in a particular space within the last day, the area should be both cleaned and disinfected.
“Disinfection is only recommended in indoor settings — schools and homes — where there has been a suspected or confirmed case of Covid-19 within the last 24 hours,” Dr. Walensky said during the White House briefing. “Also, in most cases, fogging, fumigation and wide-area or electrostatic spraying is not recommended as a primary method of disinfection and has several safety risks to consider.”
And the new cleaning guidelines do not apply to health care facilities, which may require more intensive cleaning and disinfection.
Saskia Popescu, an infectious disease epidemiologist at George Mason University, said that she was happy to see the new guidance, which “reflects our evolving data on transmission throughout the pandemic.”
But she noted that it remained important to continue doing some regular cleaning — and maintaining good hand-washing practices — to reduce the risk of contracting not just the coronavirus but any other pathogens that might be lingering on a particular surface.
Dr. Allen said that the school and business officials he has spoken with this week expressed relief over the updated guidelines, which will allow them to pull back on some of their intensive cleaning regimens. “This frees up a lot of organizations to spend that money better,” he said.
Schools, businesses and other institutions that want to keep people safe should shift their attention from surfaces to air quality, he said, and invest in improved ventilation and filtration.
“This should be the end of deep cleaning,” Dr. Allen said, noting that the misplaced focus on surfaces has had real costs. “It has led to closed playgrounds, it has led to taking nets off basketball courts, it has led to quarantining books in the library. It has led to entire missed school days for deep cleaning. It has led to not being able to share a pencil. So that’s all that hygiene theater, and it’s a direct result of not properly classifying surface transmission as low risk.”
Alex Wong / Chet Strange/ Sarah Silbiger / Bloomberg / Getty / The Atlantic
When the polio vaccine was declared safe and effective, the news was met with jubilant celebration. Church bells rang across the nation, and factories blew their whistles. “Polio routed!” newspaper headlines exclaimed. “An historic victory,” “monumental,” “sensational,” newscasters declared. People erupted with joy across the United States. Some danced in the streets; others wept. Kids were sent home from school to celebrate.
One might have expected the initial approval of the coronavirus vaccines to spark similar jubilation—especially after a brutal pandemic year. But that didn’t happen. Instead, the steady drumbeat of good news about the vaccines has been met with a chorus of relentless pessimism.
The problem is not that the good news isn’t being reported, or that we should throw caution to the wind just yet. It’s that neither the reporting nor the public-health messaging has reflected the truly amazing reality of these vaccines. There is nothing wrong with realism and caution, but effective communication requires a sense of proportion—distinguishing between due alarm and alarmism; warranted, measured caution and doombait; worst-case scenarios and claims of impending catastrophe. We need to be able to celebrate profoundly positive news while noting the work that still lies ahead. However, instead of balanced optimism since the launch of the vaccines, the public has been offered a lot of misguided fretting over new virus variants, subjected to misleading debates about the inferiority of certain vaccines, and presented with long lists of things vaccinated people still cannot do, while media outlets wonder whether the pandemic will ever end.
This pessimism is sapping people of energy to get through the winter, and the rest of this pandemic. Anti-vaccination groups and those opposing the current public-health measures have been vigorously amplifying the pessimistic messages—especially the idea that getting vaccinated doesn’t mean being able to do more—telling their audiences that there is no point in compliance, or in eventual vaccination, because it will not lead to any positive changes. They are using the moment and the messaging to deepen mistrust of public-health authorities, accusing them of moving the goalposts and implying that we’re being conned. Either the vaccines aren’t as good as claimed, they suggest, or the real goal of pandemic-safety measures is to control the public, not the virus.
Five key fallacies and pitfalls have affected public-health messaging, as well as media coverage, and have played an outsize role in derailing an effective pandemic response. These problems were deepened by the ways that we—the public—developed to cope with a dreadful situation under great uncertainty. And now, even as vaccines offer brilliant hope, and even though, at least in the United States, we no longer have to deal with the problem of a misinformer in chief, some officials and media outlets are repeating many of the same mistakes in handling the vaccine rollout.
The pandemic has given us an unwelcome societal stress test, revealing the cracks and weaknesses in our institutions and our systems. Some of these are common to many contemporary problems, including political dysfunction and the way our public sphere operates. Others are more particular, though not exclusive, to the current challenge—including a gap between how academic research operates and how the public understands that research, and the ways in which the psychology of coping with the pandemic have distorted our response to it.
Recognizing all these dynamics is important, not only for seeing us through this pandemic—yes, it is going to end—but also to understand how our society functions, and how it fails. We need to start shoring up our defenses, not just against future pandemics but against all the myriad challenges we face—political, environmental, societal, and technological. None of these problems is impossible to remedy, but first we have to acknowledge them and start working to fix them—and we’re running out of time.
The past 12 months were incredibly challenging for almost everyone. Public-health officials were fighting a devastating pandemic and, at least in this country, an administration hell-bent on undermining them. The World Health Organization was not structured or funded for independence or agility, but still worked hard to contain the disease. Many researchers and experts noted the absence of timely and trustworthy guidelines from authorities, and tried to fill the void by communicating their findings directly to the public on social media. Reporters tried to keep the public informed under time and knowledge constraints, which were made more severe by the worsening media landscape. And the rest of us were trying to survive as best we could, looking for guidance where we could, and sharing information when we could, but always under difficult, murky conditions.
Despite all these good intentions, much of the public-health messaging has been profoundly counterproductive. In five specific ways, the assumptions made by public officials, the choices made by traditional media, the way our digital public sphere operates, and communication patterns between academic communities and the public proved flawed.
Risk Compensation
One of the most important problems undermining the pandemic response has been the mistrust and paternalism that some public-health agencies and experts have exhibited toward the public. A key reason for this stance seems to be that some experts feared that people would respond to something that increased their safety—such as masks, rapid tests, or vaccines—by behaving recklessly. They worried that a heightened sense of safety would lead members of the public to take risks that would not just undermine any gains, but reverse them.
The theory that things that improve our safety might provide a false sense of security and lead to reckless behavior is attractive—it’s contrarian and clever, and fits the “here’s something surprising we smart folks thought about” mold that appeals to, well, people who think of themselves as smart. Unsurprisingly, such fears have greeted efforts to persuade the public to adopt almost every advance in safety, including seat belts, helmets, and condoms.
But time and again, the numbers tell a different story: Even if safety improvements cause a few people to behave recklessly, the benefitsoverwhelmthe ill effects. In any case, most people are already interested in staying safe from a dangerous pathogen. Further, even at the beginning of the pandemic, sociological theory predictedthat wearing masks would be associated with increased adherence to other precautionary measures—people interested in staying safe are interested in staying safe—and empirical research quickly confirmedexactly that. Unfortunately, though, the theory of risk compensation—and its implicit assumptions—continue to haunt our approach, in part because there hasn’t been a reckoning with the initial missteps.
Rules in Place of Mechanisms and Intuitions
Much of the public messaging focused on offering a series of clear rules to ordinary people, instead of explaining in detail the mechanisms of viral transmission for this pathogen. A focus on explaining transmission mechanisms, and updating our understanding over time, would have helped empower people to make informed calculations about risk in different settings. Instead, both the CDC and the WHO chose to offer fixed guidelines that lent a false sense of precision.
In the United States, the public was initially told that “close contact” meant coming within six feet of an infected individual, for 15 minutes or more. This messaging led to ridiculous gaming of the rules; some establishments moved people around at the 14th minute to avoid passing the threshold. It also led to situations in which people working indoors with others, but just outside the cutoff of six feet, felt that they could take their mask off. None of this made any practical sense. What happened at minute 16? Was seven feet okay? Faux precision isn’t more informative; it’s misleading.
All of this was complicated by the fact that key public-health agencies like the CDC and the WHO were late to acknowledge the importance of some key infection mechanisms, such as aerosol transmission. Even when they did so, the shift happened without a proportional change in the guidelines or the messaging—it was easy for the general public to miss its significance.
Frustrated by the lack of public communication from health authorities, I wrote an article last July on what we then knew about the transmission of this pathogen—including how it could be spread via aerosols that can float and accumulate, especially in poorly ventilated indoor spaces. To this day, I’m contacted by people who describe workplaces that are following the formal guidelines, but in ways that defy reason: They’ve installed plexiglass, but barred workers from opening their windows; they’ve mandated masks, but only when workers are within six feet of one another, while permitting them to be taken off indoors during breaks.
Perhaps worst of all, our messaging and guidelines elided the difference between outdoor and indoor spaces, where, given the importance of aerosol transmission, the same precautions should not apply. This is especially important because this pathogen is overdispersed: Much of the spread is driven by a few people infecting many others at once, while most people do not transmit the virus at all.
After I wrote an article explaining how overdispersion and super-spreading were driving the pandemic, I discovered that this mechanism had also been poorly explained. I was inundated by messages from people, including elected officials around the world, saying they had no idea that this was the case. None of it was secret—numerous academic papers and articles had been written about it—but it had not been integrated into our messaging or our guidelines despite its great importance.
Crucially, super-spreading isn’t equally distributed; poorly ventilated indoor spaces can facilitate the spread of the virus over longer distances, and in shorter periods of time, than the guidelines suggested, and help fuel the pandemic.
Outdoors? It’s the opposite.
There is a solid scientific reason for the fact that there are relatively few documented cases of transmission outdoors, even after a year of epidemiological work: The open air dilutes the virus very quickly, and the sun helps deactivate it, providing further protection. And super-spreading—the biggest driver of the pandemic— appears to be an exclusively indoor phenomenon. I’ve been tracking every report I can find for the past year, and have yet to find a confirmed super-spreading event that occurred solely outdoors. Such events might well have taken place, but if the risk were great enough to justify altering our lives, I would expect at least a few to have been documented by now.
And yet our guidelines do not reflect these differences, and our messaging has not helped people understand these facts so that they can make better choices. I published my first article pleading for parks to be kept open on April 7, 2020—but outdoor activities are still banned by some authorities today, a full year after this dreaded virus began to spread globally.
We’d have been much better off if we gave people a realistic intuition about this virus’s transmission mechanisms. Our public guidelines should have been more like Japan’s, which emphasize avoiding the three C’s—closed spaces, crowded places, and close contact—that are driving the pandemic.
Scolding and Shaming
Throughout the past year, traditional and social media have been caught up in a cycle of shaming—made worse by being so unscientific and misguided. How dare you go to the beach? newspapers have scolded us for months, despite lacking evidence that this posed any significant threat to public health. It wasn’t just talk: Many cities closed parks and outdoor recreational spaces, even as they kept open indoor dining and gyms. Just this month, UC Berkeley and the University of Massachusetts at Amherst both banned students from taking even solitary walks outdoors.
Even when authorities relax the rules a bit, they do not always follow through in a sensible manner. In the United Kingdom, after some locales finally started allowing children to play on playgrounds—something that was already way overdue—they quickly ruled that parents must not socialize while their kids have a normal moment. Why not? Who knows?
On social media, meanwhile, pictures of people outdoors without masks draw reprimands, insults, and confident predictions of super-spreading—and yet few note when super-spreading fails to follow.
While visible but low-risk activities attract the scolds, other actual risks—in workplaces and crowded households, exacerbated by the lack of testing or paid sick leave—are not as easily accessible to photographers. Stefan Baral, an associate epidemiology professor at the Johns Hopkins Bloomberg School of Public Health, says that it’s almost as if we’ve “designed a public-health response most suitable for higher-income” groups and the “Twitter generation”—stay home; have your groceries delivered; focus on the behaviors you can photograph and shame online—rather than provide the support and conditionsnecessary for more people to keep themselves safe.
And the viral videos shaming people for failing to take sensible precautions, such as wearing masks indoors, do not necessarily help. For one thing, fretting over the occasional person throwing a tantrum while going unmasked in a supermarket distorts the reality: Most of the public has been complying with mask wearing. Worse, shaming is often an ineffective way of getting people to change their behavior, and it entrenches polarization and discourages disclosure, making it harder to fight the virus. Instead, we should be emphasizing safer behavior and stressing how many people are doing their part, while encouraging others to do the same.
Harm Reduction
Amidst all the mistrust and the scolding, a crucial public-health concept fell by the wayside. Harm reduction is the recognition that if there is an unmet and yet crucial human need, we cannot simply wish it away; we need to advise people on how to do what they seek to do more safely. Risk can never be completely eliminated; life requires more than futile attempts to bring risk down to zero. Pretending we can will away complexities and trade-offs with absolutism is counterproductive. Consider abstinence-only education: Not letting teenagers know about ways to have safer sex results in more of them having sex with no protections.
As Julia Marcus, an epidemiologist and associate professor at Harvard Medical School, told me, “When officials assume that risks can be easily eliminated, they might neglect the other things that matter to people: staying fed and housed, being close to loved ones, or just enjoying their lives. Public health works best when it helps people find safer ways to get what they need and want.””
Another problem with absolutism is the “abstinence violation” effect, Joshua Barocas, an assistant professor at the Boston University School of Medicine and Infectious Diseases, told me. When we set perfection as the only option, it can cause people who fall short of that standard in one small, particular way to decide that they’ve already failed, and might as well give up entirely. Most people who have attempted a diet or a new exercise regimen are familiar with this psychological state. The better approach is encouraging risk reduction and layered mitigation—emphasizing that every little bit helps—while also recognizing that a risk-free life is neither possible nor desirable.
Socializing is not a luxury—kids need to play with one another, and adults need to interact. Your kids can play together outdoors, and outdoor time is the best chance to catch up with your neighbors is not just a sensible message; it’s a way to decrease transmission risks. Some kids will play and some adults will socialize no matter what the scolds say or public-health officials decree, and they’ll do it indoors, out of sight of the scolding.
And if they don’t? Then kids will be deprived of an essential activity, and adults will be deprived of human companionship. Socializing is perhaps the most important predictor of health and longevity, after not smoking and perhaps exercise and a healthy diet. We need to help people socialize more safely, not encourage them to stop socializing entirely.
The Balance Between Knowledge And Action
Last but not least, the pandemic response has been distorted by a poor balance between knowledge, risk, certainty, and action.
Sometimes, public-health authorities insisted that we did not know enough to act, when the preponderance of evidence already justified precautionary action. Wearing masks, for example, posed few downsides, and held the prospect of mitigating the exponential threat we faced. The wait for certainty hampered our response to airborne transmission, even though there was almost no evidence for—and increasing evidence against—the importance of fomites, or objects that can carry infection. And yet, we emphasized the risk of surface transmission while refusing to properly address the risk of airborne transmission, despite increasing evidence. The difference lay not in the level of evidence and scientific support for either theory—which, if anything, quickly tilted in favor of airborne transmission, and not fomites, being crucial—but in the fact that fomite transmission had been a key part of the medical canon, and airborne transmission had not.
Sometimes, experts and the public discussion failed to emphasize that we were balancing risks, as in the recurring cycles of debate over lockdowns or school openings. We should have done more to acknowledge that there were no good options, only trade-offs between different downsides. As a result, instead of recognizing the difficulty of the situation, too many people accused those on the other side of being callous and uncaring.
And sometimes, the way that academics communicate clashed with how the public constructs knowledge. In academia, publishing is the coin of the realm, and it is often done through rejecting the null hypothesis—meaning that many papers do not seek to prove something conclusively, but instead, to reject the possibility that a variable has no relationship with the effect they are measuring (beyond chance). If that sounds convoluted, it is—there are historical reasons for this methodology and big arguments within academia about its merits, but for the moment, this remains standard practice.
At crucial points during the pandemic, though, this resulted in mistranslations and fueled misunderstandings, which were further muddled by differing stances toward prior scientific knowledge and theory. Yes, we faced a novel coronavirus, but we should have started by assuming that we could make some reasonable projections from prior knowledge, while looking out for anything that might prove different. That prior experience should have made us mindful of seasonality, the key role of overdispersion, and aerosol transmission. A keen eye for what was different from the past would have alerted us earlier to the importance of presymptomatic transmission.
Thus, on January 14, 2020, the WHO stated that there was “no clear evidence of human-to-human transmission.” It should have said, “There is increasing likelihood that human-to-human transmission is taking place, but we haven’t yet proven this, because we have no access to Wuhan, China.” (Cases were already popping up around the world at that point.) Acting as if there was human-to-human transmission during the early weeks of the pandemic would have been wise and preventive.
Later that spring, WHO officials stated that there was “currently no evidence that people who have recovered from COVID-19 and have antibodies are protected from a second infection,” producing many articles laden with panic and despair. Instead, it should have said: “We expect the immune system to function against this virus, and to provide some immunity for some period of time, but it is still hard to know specifics because it is so early.”
Similarly, since the vaccines were announced, too many statements have emphasized that we don’t yet know if vaccines prevent transmission. Instead, public-health authorities should have said that we have many reasons to expect, and increasing amounts of data to suggest, that vaccines will blunt infectiousness, but that we’re waiting for additional data to be more precise about it. That’s been unfortunate, because while many, many things have gone wrong during this pandemic, the vaccines are one thing that has gone very, very right.
As late as April 2020, Anthony Fauci was slammed for being too optimistic for suggesting we might plausibly have vaccines in a year to 18 months. We had vaccines much, much sooner than that: The first two vaccine trials concluded a mere eight months after the WHO declared a pandemic in March 2020.
Moreover, they have delivered spectacular results. In June 2020, the FDA said a vaccine that was merely 50 percent efficacious in preventing symptomatic COVID-19 would receive emergency approval—that such a benefit would be sufficient to justify shipping it out immediately. Just a few months after that, the trials of the Moderna and Pfizer vaccines concluded by reporting not just a stunning 95 percent efficacy, but also a complete elimination of hospitalization or death among the vaccinated. Even severe disease was practically gone: The lone case classified as “severe” among 30,000 vaccinated individuals in the trials was so mild that the patient needed no medical care, and her case would not have been considered severe if her oxygen saturation had been a single percent higher.
These are exhilarating developments, because global, widespread, and rapid vaccination is our way out of this pandemic. Vaccines that drastically reduce hospitalizations and deaths, and that diminish even severe disease to a rare event, are the closest things we have had in this pandemic to a miracle—though of course they are the product of scientific research, creativity, and hard work. They are going to be the panacea and the endgame.
And yet, two months into an accelerating vaccination campaign in the United States, it would be hard to blame people if they missed the news that things are getting better.
Yes, there are new variants of the virus, which may eventually require booster shots, but at least so far, the existing vaccines are standing up to them well—very, very well. Manufacturers are already working on new vaccines or variant-focused booster versions, in case they prove necessary, and the authorizing agencies are ready for a quick turnaround if and when updates are needed. Reports from places that have vaccinated large numbers of individuals, and even trials in places where variants are widespread, are exceedingly encouraging, with dramatic reductions in cases and, crucially, hospitalizations and deaths among the vaccinated. Global equity and access to vaccines remain crucial concerns, but the supply is increasing.
Here in the United States, despite the rocky rollout and the need to smooth access and ensure equity, it’s become clear that toward the end of spring 2021, supply will be more than sufficient. It may sound hard to believe today, as many who are desperate for vaccinations await their turn, but in the near future, we may have to discuss what to do with excess doses.
So why isn’t this story more widely appreciated?
Part of the problem with the vaccines was the timing—the trials concluded immediately after the U.S. election, and their results got overshadowed in the weeks of political turmoil. The first, modest headline announcing the Pfizer-BioNTech results in The New York Times was a single column, “Vaccine Is Over 90% Effective, Pfizer’s Early Data Says,” below a banner headline spanning the page: “BIDEN CALLS FOR UNITED FRONT AS VIRUS RAGES.” That was both understandable—the nation was weary—and a loss for the public.
Just a few days later, Moderna reported a similar 94.5 percent efficacy. If anything, that provided even more cause for celebration, because it confirmed that the stunning numbers coming out of Pfizer weren’t a fluke. But, still amid the political turmoil, the Moderna report got a mere two columns on The New York Times’ front page with an equally modest headline: “Another Vaccine Appears to Work Against the Virus.”
So we didn’t get our initial vaccine jubilation.
But as soon as we began vaccinating people, articles started warning the newly vaccinated about all they could not do. “COVID-19 Vaccine Doesn’t Mean You Can Party Like It’s 1999,” one headline admonished. And the buzzkill has continued right up to the present. “You’re fully vaccinated against the coronavirus—now what? Don’t expect to shed your mask and get back to normal activities right away,” began a recent Associated Press story.
People might well want to party after being vaccinated. Those shots will expand what we can do, first in our private lives and among other vaccinated people, and then, gradually, in our public lives as well. But once again, the authorities and the media seem more worried about potentially reckless behavior among the vaccinated, and about telling them what not to do, than with providing nuanced guidance reflecting trade-offs, uncertainty, and a recognition that vaccination can change behavior. No guideline can cover every situation, but careful, accurate, and updated information can empower everyone.
Take the messaging and public conversation around transmission risks from vaccinated people. It is, of course, important to be alert to such considerations: Many vaccines are “leaky” in that they prevent disease or severe disease, but not infection and transmission. In fact, completely blocking all infection—what’s often called “sterilizing immunity”—is a difficult goal, and something even many highly effective vaccines don’t attain, but that doesn’t stop them from being extremely useful.
As Paul Sax, an infectious-disease doctor at Boston’s Brigham & Women’s Hospital, put it in early December, it would be enormously surprising “if these highly effective vaccines didn’t also make people less likely to transmit.” From multiple studies, we already knew that asymptomatic individuals—those who never developed COVID-19 despite being infected—were much less likely to transmit the virus. The vaccine trials were reporting 95 percent reductions in any form of symptomatic disease. In December, we learned that Moderna had swabbed some portion of trial participants to detect asymptomatic, silent infections, and found an almost two-thirds reduction even in such cases. The good news kept pouring in. Multiple studies found that, even in those few cases where breakthrough disease occurred in vaccinated people, their viral loads were lower—which correlates with lower rates of transmission. Data from vaccinated populations further confirmed what many experts expected all along: Of course these vaccines reduce transmission.
And yet, from the beginning, a good chunk of the public-facing messaging and news articles implied or claimed that vaccines won’t protect you against infecting other people or that we didn’t know if they would, when both were false. I found myself trying to convince people in my own social network that vaccines weren’t useless against transmission, and being bombarded on social media with claims that they were.
What went wrong? The same thing that’s going wrong right now with the reporting on whether vaccines will protect recipients against the new viral variants. Some outlets emphasize the worst or misinterpret the research. Some public-health officials are wary of encouraging the relaxation of any precautions. Some prominent experts on social media—even those with seemingly solid credentials—tend to respond to everything with alarm and sirens. So the message that got heard was that vaccines will not prevent transmission, or that they won’t work against new variants, or that we don’t know if they will. What the public needs to hear, though, is that based on existing data, we expect them to work fairly well—but we’ll learn more about precisely how effective they’ll be over time, and that tweaks may make them even better.
A year into the pandemic, we’re still repeating the same mistakes.
The top-down messaging is not the only problem. The scolding, the strictness, the inability to discuss trade-offs, and the accusations of not caring about people dying not only have an enthusiastic audience, but portions of the public engage in these behaviors themselves. Maybe that’s partly because proclaiming the importance of individual actions makes us feel as if we are in the driver’s seat, despite all the uncertainty.
Psychologists talk about the “locus of control”—the strength of belief in control over your own destiny. They distinguish between people with more of an internal-control orientation—who believe that they are the primary actors—and those with an external one, who believe that society, fate, and other factors beyond their control greatly influence what happens to us. This focus on individual control goes along with something called the “fundamental attribution error”—when bad things happen to other people, we’re more likely to believe that they are personally at fault, but when they happen to us, we are more likely to blame the situation and circumstances beyond our control.
An individualistic locus of control is forged in the U.S. mythos—that we are a nation of strivers and people who pull ourselves up by our bootstraps. An internal-control orientation isn’t necessarily negative; it can facilitate resilience, rather than fatalism, by shifting the focus to what we can do as individuals even as things fall apart around us. This orientation seems to be common among children who not only survive but sometimes thrive in terrible situations—they take charge and have a go at it, and with some luck, pull through. It is probably even more attractive to educated, well-off people who feel that they have succeeded through their own actions.
You can see the attraction of an individualized, internal locus of control in a pandemic, as a pathogen without a cure spreads globally, interrupts our lives, makes us sick, and could prove fatal.
There have been very few things we could do at an individual level to reduce our risk beyond wearing masks, distancing, and disinfecting. The desire to exercise personal control against an invisible, pervasive enemy is likely why we’ve continued to emphasize scrubbing and cleaning surfaces, in what’s appropriately called “hygiene theater,” long after it became clear that fomites were not a key driver of the pandemic. Obsessive cleaning gave us something to do, and we weren’t about to give it up, even if it turned out to be useless. No wonder there was so much focus on telling others to stay home—even though it’s not a choice available to those who cannot work remotely—and so much scolding of those who dared to socialize or enjoy a moment outdoors.
And perhaps it was too much to expect a nation unwilling to release its tight grip on the bottle of bleach to greet the arrival of vaccines—however spectacular—by imagining the day we might start to let go of our masks.
The focus on individual actions has had its upsides, but it has also led to a sizable portion of pandemic victims being erased from public conversation. If our own actions drive everything, then some other individuals must be to blame when things go wrong for them. And throughout this pandemic, the mantra many of us kept repeating—“Wear a mask, stay home; wear a mask, stay home”—hid many of the real victims.
Study after study, in country after country, confirms that this disease has disproportionately hit the poor and minority groups, along with the elderly, who are particularly vulnerable to severe disease. Even among the elderly, though, those who are wealthier and enjoy greater access to health care have fared better.
The poor and minority groups are dying in disproportionately large numbers for the same reasons that they suffer from many other diseases: a lifetime of disadvantages, lack of access to health care, inferior working conditions, unsafe housing, and limited financial resources.
Many lacked the option of staying home precisely because they were working hard to enable others to do what they could not, by packing boxes, delivering groceries, producing food. And even those who could stay home faced other problems born of inequality: Crowded housing is associatedwith higher rates of COVID-19 infection and worse outcomes, likely because many of the essential workers who live in such housing bring the virus home to elderly relatives.
Individual responsibility certainly had a large role to play in fighting the pandemic, but many victims had little choice in what happened to them. By disproportionately focusing on individual choices, not only did we hide the real problem, but we failed to do more to provide safe working and living conditions for everyone.
For example, there has been a lot of consternation about indoor dining, an activity I certainly wouldn’t recommend. But even takeout and delivery can impose a terrible cost: One study of California found that line cooks are the highest-risk occupation for dying of COVID-19. Unless we provide restaurants with funds so they can stay closed, or provide restaurant workers with high-filtration masks, better ventilation, paid sick leave, frequent rapid testing, and other protections so that they can safely work, getting food to go can simply shift the risk to the most vulnerable. Unsafe workplaces may be low on our agenda, but they do pose a real danger. Bill Hanage, associate professor of epidemiology at Harvard, pointed me to a paper he co-authored: Workplace-safety complaints to OSHA—which oversees occupational-safety regulations—during the pandemic were predictive of increases in deaths 16 days later.
New data highlight the terrible toll of inequality: Life expectancy has decreased dramatically over the past year, with Black people losing the most from this disease, followed by members of the Hispanic community. Minorities are also more likely to die of COVID-19 at a younger age. But when the new CDC director, Rochelle Walensky, noted this terrible statistic, she immediately followed up by urging people to “continue to use proven prevention steps to slow the spread—wear a well-fitting mask, stay 6 ft away from those you do not live with, avoid crowds and poorly ventilated places, and wash hands often.”
Those recommendations aren’t wrong, but they are incomplete. None of these individual acts do enough to protect those to whom such choices aren’t available—and the CDC has yet to issue sufficient guidelines for workplace ventilation or to make higher-filtration masks mandatory, or even available, for essential workers. Nor are these proscriptions paired frequently enough with prescriptions: Socialize outdoors, keep parks open, and let children play with one another outdoors.
Vaccines are the tool that will end the pandemic. The story of their rollout combines some of our strengths and our weaknesses, revealing the limitations of the way we think and evaluate evidence, provide guidelines, and absorb and react to an uncertain and difficult situation.
But also, after a weary year, maybe it’s hard for everyone—including scientists, journalists, and public-health officials—to imagine the end, to have hope. We adjust to new conditions fairly quickly, even terrible new conditions. During this pandemic, we’ve adjusted to things many of us never thought were possible. Billions of people have led dramatically smaller, circumscribed lives, and dealt with closed schools, the inability to see loved ones, the loss of jobs, the absence of communal activities, and the threat and reality of illness and death.
Hope nourishes us during the worst times, but it is also dangerous. It upsets the delicate balance of survival—where we stop hoping and focus on getting by—and opens us up to crushing disappointment if things don’t pan out. After a terrible year, many things are understandably making it harder for us to dare to hope. But, especially in the United States, everything looks better by the day. Tragically, at least 28 million Americans have been confirmed to have been infected, but the real number is certainly much higher. By one estimate, as many as 80 million have already been infected with COVID-19, and many of those people now have some level of immunity. Another 46 million people have already received at least one dose of a vaccine, and we’re vaccinating millions more each day as the supply constraints ease. The vaccines are poised to reduce or nearly eliminate the things we worry most about—severe disease, hospitalization, and death.
Not all our problems are solved. We need to get through the next few months, as we race to vaccinate against more transmissible variants. We need to do more to address equity in the United States—because it is the right thing to do, and because failing to vaccinate the highest-risk people will slow the population impact. We need to make sure that vaccines don’t remain inaccessible to poorer countries. We need to keep up our epidemiological surveillance so that if we do notice something that looks like it may threaten our progress, we can respond swiftly.
And the public behavior of the vaccinated cannot change overnight—even if they are at much lower risk, it’s not reasonable to expect a grocery store to try to verify who’s vaccinated, or to have two classes of people with different rules. For now, it’s courteous and prudent for everyone to obey the same guidelines in many public places. Still, vaccinated people can feel more confident in doing things they may have avoided, just in case—getting a haircut, taking a trip to see a loved one, browsing for nonessential purchases in a store.
But it is time to imagine a better future, not just because it’s drawing nearer but because that’s how we get through what remains and keep our guard up as necessary. It’s also realistic—reflecting the genuine increased safety for the vaccinated.
Public-health agencies should immediately start providing expanded information to vaccinated people so they can make informed decisions about private behavior. This is justified by the encouraging data, and a great way to get the word out on how wonderful these vaccines really are. The delay itself has great human costs, especially for those among the elderly who have been isolated for so long.
Public-health authorities should also be louder and more explicit about the next steps, giving us guidelines for when we can expect easing in rules for public behavior as well. We need the exit strategy spelled out—but with graduated, targeted measures rather than a one-size-fits-all message. We need to let people know that getting a vaccine will almost immediately change their lives for the better, and why, and also when and how increased vaccination will change more than their individual risks and opportunities, and see us out of this pandemic.
We should encourage people to dream about the end of this pandemic by talking about it more, and more concretely: the numbers, hows, and whys. Offering clear guidance on how this will end can help strengthen people’s resolve to endure whatever is necessary for the moment—even if they are still unvaccinated—by building warranted and realistic anticipation of the pandemic’s end.
Hope will get us through this. And one day soon, you’ll be able to hop off the subway on your way to a concert, pick up a newspaper, and find the triumphant headline: “COVID Routed!”
Zeynep Tufekci is a contributing writer at The Atlantic and an associate professor at the University of North Carolina. She studies the interaction between digital technology, artificial intelligence, and society.
Lincoln Park in Chicago. Scientists are hopeful, as vaccinations continue and despite the emergence of variants, that we’re past the worst of the pandemic. Credit: Lyndon French for The New York Times
Many scientists are expecting another rise in infections. But this time the surge will be blunted by vaccines and, hopefully, widespread caution. By summer, Americans may be looking at a return to normal life.
Published Feb. 25, 2021Updated Feb. 26, 2021, 12:07 a.m. ET
Across the United States, and the world, the coronavirus seems to be loosening its stranglehold. The deadly curve of cases, hospitalizations and deaths has yo-yoed before, but never has it plunged so steeply and so fast.
Is this it, then? Is this the beginning of the end? After a year of being pummeled by grim statistics and scolded for wanting human contact, many Americans feel a long-promised deliverance is at hand.
Americans will win against the virus and regain many aspects of their pre-pandemic lives, most scientists now believe. Of the 21 interviewed for this article, all were optimistic that the worst of the pandemic is past. This summer, they said, life may begin to seem normal again.
But — of course, there’s always a but — researchers are also worried that Americans, so close to the finish line, may once again underestimate the virus.
So far, the two vaccines authorized in the United States are spectacularly effective, and after a slow start, the vaccination rollout is picking up momentum. A third vaccine is likely to be authorized shortly, adding to the nation’s supply.
But it will be many weeks before vaccinations make a dent in the pandemic. And now the virus is shape-shifting faster than expected, evolving into variants that may partly sidestep the immune system.
The latest variant was discovered in New York City only this week, and another worrisome version is spreading at a rapid pace through California. Scientists say a contagious variant first discovered in Britain will become the dominant form of the virus in the United States by the end of March.
The road back to normalcy is potholed with unknowns: how well vaccines prevent further spread of the virus; whether emerging variants remain susceptible enough to the vaccines; and how quickly the world is immunized, so as to halt further evolution of the virus.
But the greatest ambiguity is human behavior. Can Americans desperate for normalcy keep wearing masks and distancing themselves from family and friends? How much longer can communities keep businesses, offices and schools closed?
Covid-19 deaths will most likely never rise quite as precipitously as in the past, and the worst may be behind us. But if Americans let down their guard too soon — many states are already lifting restrictions — and if the variants spread in the United States as they have elsewhere, another spike in cases may well arrive in the coming weeks.
Scientists call it the fourth wave. The new variants mean “we’re essentially facing a pandemic within a pandemic,” said Adam Kucharski, an epidemiologist at the London School of Hygiene and Tropical Medicine.
The declines are real, but they disguise worrying trends.
Credit: Daniel Dreifuss for The New York Times
The United States has now recorded 500,000 deaths amid the pandemic, a terrible milestone. As of Wednesday morning, at least 28.3 million people have been infected.
But the rate of new infections has tumbled by 35 percent over the past two weeks, according to a database maintained by The New York Times. Hospitalizations are down 31 percent, and deaths have fallen by 16 percent.
Yet the numbers are still at the horrific highs of November, scientists noted. At least 3,210 people died of Covid-19 on Wednesday alone. And there is no guarantee that these rates will continue to decrease.
“Very, very high case numbers are not a good thing, even if the trend is downward,” said Marc Lipsitch, an epidemiologist at the Harvard T.H. Chan School of Public Health in Boston. “Taking the first hint of a downward trend as a reason to reopen is how you get to even higher numbers.”
In late November, for example, Gov. Gina Raimondo of Rhode Island limited social gatherings and some commercial activities in the state. Eight days later, cases began to decline. The trend reversed eight days after the state’s pause lifted on Dec. 20.
The virus’s latest retreat in Rhode Island and most other states, experts said, results from a combination of factors: growing numbers of people with immunity to the virus, either from having been infected or from vaccination; changes in behavior in response to the surges of a few weeks ago; and a dash of seasonality — the effect of temperature and humidity on the survival of the virus.
The vaccines were first rolled out to residents of nursing homes and to the elderly, who are at highest risk of severe illness and death. That may explain some of the current decline in hospitalizations and deaths.
Credit: Joao Silva/The New York Times
But young people drive the spread of the virus, and most of them have not yet been inoculated. And the bulk of the world’s vaccine supply has been bought up by wealthy nations, which have amassed one billion more doses than needed to immunize their populations.
Vaccination cannot explain why cases are dropping even in countries where not a single soul has been immunized, like Honduras, Kazakhstan or Libya. The biggest contributor to the sharp decline in infections is something more mundane, scientists say: behavioral change.
Leaders in the United States and elsewhere stepped up community restrictions after the holiday peaks. But individual choices have also been important, said Lindsay Wiley, an expert in public health law and ethics at American University in Washington.
“People voluntarily change their behavior as they see their local hospital get hit hard, as they hear about outbreaks in their area,” she said. “If that’s the reason that things are improving, then that’s something that can reverse pretty quickly, too.”
The downward curve of infections with the original coronavirus disguises an exponential rise in infections with B.1.1.7, the variant first identified in Britain, according to many researchers.
“We really are seeing two epidemic curves,” said Ashleigh Tuite, an infectious disease modeler at the University of Toronto.
The B.1.1.7 variant is thought to be more contagious and more deadly, and it is expected to become the predominant form of the virus in the United States by late March. The number of cases with the variant in the United States has risen from 76 in 12 states as of Jan. 13 to more than 1,800 in 45 states now. Actual infections may be much higher because of inadequate surveillance efforts in the United States.
Buoyed by the shrinking rates over all, however, governors are lifting restrictions across the United States and are under enormous pressure to reopen completely. Should that occur, B.1.1.7 and the other variants are likely to explode.
“Everybody is tired, and everybody wants things to open up again,” Dr. Tuite said. “Bending to political pressure right now, when things are really headed in the right direction, is going to end up costing us in the long term.”
Another wave may be coming, but it can be minimized.
Credit: Lyndon French for The New York Times
Looking ahead to late March or April, the majority of scientists interviewed by The Times predicted a fourth wave of infections. But they stressed that it is not an inevitable surge, if government officials and individuals maintain precautions for a few more weeks.
A minority of experts were more sanguine, saying they expected powerful vaccines and an expanding rollout to stop the virus. And a few took the middle road.
“We’re at that crossroads, where it could go well or it could go badly,” said Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases.
The vaccines have proved to be more effective than anyone could have hoped, so far preventing serious illness and death in nearly all recipients. At present, about 1.4 million Americans are vaccinated each day. More than 45 million Americans have received at least one dose.
A team of researchers at Fred Hutchinson Cancer Research Center in Seattle tried to calculate the number of vaccinations required per day to avoid a fourth wave. In a model completed before the variants surfaced, the scientists estimated that vaccinating just one million Americans a day would limit the magnitude of the fourth wave.
“But the new variants completely changed that,” said Dr. Joshua T. Schiffer, an infectious disease specialist who led the study. “It’s just very challenging scientifically — the ground is shifting very, very quickly.”
Natalie Dean, a biostatistician at the University of Florida, described herself as “a little more optimistic” than many other researchers. “We would be silly to undersell the vaccines,” she said, noting that they are effective against the fast-spreading B.1.1.7 variant.
But Dr. Dean worried about the forms of the virus detected in South Africa and Brazil that seem less vulnerable to the vaccines made by Pfizer and Moderna. (On Wednesday, Johnson & Johnson reported that its vaccine was relatively effective against the variant found in South Africa.)
Credit: Pete Kiehart for The New York Times
About 50 infections with those two variants have been identified in the United States, but that could change. Because of the variants, scientists do not know how many people who were infected and had recovered are now vulnerable to reinfection.
South Africa and Brazil have reported reinfections with the new variants among people who had recovered from infections with the original version of the virus.
“That makes it a lot harder to say, ‘If we were to get to this level of vaccinations, we’d probably be OK,’” said Sarah Cobey, an evolutionary biologist at the University of Chicago.
Yet the biggest unknown is human behavior, experts said. The sharp drop in cases now may lead to complacency about masks and distancing, and to a wholesale lifting of restrictions on indoor dining, sporting events and more. Or … not.
“The single biggest lesson I’ve learned during the pandemic is that epidemiological modeling struggles with prediction, because so much of it depends on human behavioral factors,” said Carl Bergstrom, a biologist at the University of Washington in Seattle.
Taking into account the counterbalancing rises in both vaccinations and variants, along with the high likelihood that people will stop taking precautions, a fourth wave is highly likely this spring, the majority of experts told The Times.
Kristian Andersen, a virologist at the Scripps Research Institute in San Diego, said he was confident that the number of cases will continue to decline, then plateau in about a month. After mid-March, the curve in new cases will swing upward again.
In early to mid-April, “we’re going to start seeing hospitalizations go up,” he said. “It’s just a question of how much.”
Summer will feel like summer again, sort of.
Credit: Kendrick Brinson for The New York Times
Now the good news.
Despite the uncertainties, the experts predict that the last surge will subside in the United States sometime in the early summer. If the Biden administration can keep its promise to immunize every American adult by the end of the summer, the variants should be no match for the vaccines.
Combine vaccination with natural immunity and the human tendency to head outdoors as weather warms, and “it may not be exactly herd immunity, but maybe it’s sufficient to prevent any large outbreaks,” said Youyang Gu, an independent data scientist, who created some of the most prescient models of the pandemic.
Infections will continue to drop. More important, hospitalizations and deaths will fall to negligible levels — enough, hopefully, to reopen the country.
“Sometimes people lose vision of the fact that vaccines prevent hospitalization and death, which is really actually what most people care about,” said Stefan Baral, an epidemiologist at the Johns Hopkins Bloomberg School of Public Health.
Even as the virus begins its swoon, people may still need to wear masks in public places and maintain social distance, because a significant percent of the population — including children — will not be immunized.
“Assuming that we keep a close eye on things in the summer and don’t go crazy, I think that we could look forward to a summer that is looking more normal, but hopefully in a way that is more carefully monitored than last summer,” said Emma Hodcroft, a molecular epidemiologist at the University of Bern in Switzerland.
Imagine: Groups of vaccinated people will be able to get together for barbecues and play dates, without fear of infecting one another. Beaches, parks and playgrounds will be full of mask-free people. Indoor dining will return, along with movie theaters, bowling alleys and shopping malls — although they may still require masks.
The virus will still be circulating, but the extent will depend in part on how well vaccines prevent not just illness and death, but also transmission. The data on whether vaccines stop the spread of the disease are encouraging, but immunization is unlikely to block transmission entirely.
Credit: Pete Kiehart for The New York Times
“It’s not zero and it’s not 100 — exactly where that number is will be important,” said Shweta Bansal, an infectious disease modeler at Georgetown University. “It needs to be pretty darn high for us to be able to get away with vaccinating anything below 100 percent of the population, so that’s definitely something we’re watching.”
Over the long term — say, a year from now, when all the adults and children in the United States who want a vaccine have received them — will this virus finally be behind us?
Every expert interviewed by The Times said no. Even after the vast majority of the American population has been immunized, the virus will continue to pop up in clusters, taking advantage of pockets of vulnerability. Years from now, the coronavirus may be an annoyance, circulating at low levels, causing modest colds.
Many scientists said their greatest worry post-pandemic was that new variants may turn out to be significantly less susceptible to the vaccines. Billions of people worldwide will remain unprotected, and each infection gives the virus new opportunities to mutate.
“We won’t have useless vaccines. We might have slightly less good vaccines than we have at the moment,” said Andrew Read, an evolutionary microbiologist at Penn State University. “That’s not the end of the world, because we have really good vaccines right now.”
For now, every one of us can help by continuing to be careful for just a few more months, until the curve permanently flattens.
“Just hang in there a little bit longer,” Dr. Tuite said. “There’s a lot of optimism and hope, but I think we need to be prepared for the fact that the next several months are likely to continue to be difficult.”
But some things are improving, and it will not go on for ever
Sep 26th 2020
AS THE AUTUMNAL equinox passed, Europe was battening down the hatches for a gruelling winter. Intensive-care wards and hospital beds were filling up in Madrid and Marseille—a city which, a few months ago, thought it had more or less eliminated covid-19. Governments were implementing new restrictions, sometimes, as in England, going back on changes made just a few months ago. The al-fresco life of summer was returning indoors. Talk of a second wave was everywhere.
Across the Atlantic the United States saw its official covid-19 death toll—higher than that of all western Europe put together—break the 200,000 barrier. India, which has seen more than half a million new cases a week for four weeks running, will soon take America’s unenviable laurels as the country with the largest official case count.
The world looks set to see its millionth officially recorded death from covid-19 before the beginning of October. That is more than the World Health Organisation (WHO) recorded as having died from malaria (620,000), suicide (794,000) or HIV/AIDS (954,000) over the whole of 2017, the most recent year for which figures are available.
Those deaths represent just over 3% of the recorded covid-19 cases, which now number over 32m. That tally is itself an underestimate of the number who have actually been infected by SARS–CoV-2, the virus which causes covid 19. Many of the infected do not get sick. Many who do are never seen by any health system.
A better, if still imperfect, sense of how many infections have taken place since the outbreak began at the end of last year can be gleaned from “serosurveys” which scientists and public-health officials have undertaken around the world. These look for antibodies against SARS–CoV-2 in blood samples which may have been taken for other purposes. Their presence reveals past exposure to the virus.
Various things make these surveys inaccurate. They can pick up antibodies against other viruses, inflating their totals—an effect which can differ from place to place, as there are more similar-looking viruses circulating in some regions than in others. They can mislead in the other direction, too. Some tests miss low levels of antibody. Some people (often young ones) fight off the virus without ever producing antibodies and will thus not be recorded as having been infected. As a result, estimates based on serosurveys have to be taken with more than a grain of salt.
But in many countries it would take a small sea’s worth of the stuff to bring the serosurvey figures into line with the official number of cases. The fact that serosurvey data are spotty—there is very little, for example, openly available from China—means it is not possible to calculate the global infection rate directly from the data at hand. But by constructing an empirical relationship between death rates, case rates, average income—a reasonable proxy for intensity of testing—and seropositivity it is possible to impute rates for countries where data are not available and thus estimate a global total.
The graphic on this page shows such an estimate based on 279 serosurveys in 19 countries. It suggests that infections were already running at over 1m a day by the end of January—when the world at large was only just beginning to hear of the virus’s existence. In May the worldwide rate appears to have been more than 5m a day. The uncertainties in the estimate are large, and become greater as you draw close to the present, but all told it finds that somewhere between 500m and 730m people worldwide have been infected—from 6.4% to 9.3% of the world’s population. The WHO has not yet released serosurvey-based estimates of its own, though such work is under way; but it has set an upper bound at 10% of the global population.
As the upper part of the following data panel shows, serosurvey results which can be directly compared with the diagnosed totals are often a great deal bigger. In Germany, where cases have been low and testing thorough, the seropositivity rate was 4.5 times the diagnosed rate in August. In Minnesota a survey carried out in July found a multiplier of seven. A survey completed on August 23rd found a 6.02% seropositivity rate in England, implying a multiplier of 12. A national serosurvey of India conducted from the middle of May to early June found that 0.73% were infected, suggesting a national total of 10m. The number of registered cases at that time was 226,713, giving a multiplier of 44. Such results suggest that a global multiplier of 20 or so is quite possible.
If the disease is far more widespread than it appears, is it proportionately less deadly than official statistics, mainly gathered in rich countries, have made it look? Almost certainly. On the basis of British figures David Spiegelhalter, who studies the public understanding of risk at Cambridge University, has calculated that the risk of death from covid increases by about 13% for every year of age, which means a 65-year-old is 100 times more likely to die than a 25-year-old. And 65-year-olds are not evenly distributed around the world. Last year 20.5% of the EU’s population was over 65, as opposed to just 3% of sub-Saharan Africa’s.
But it is also likely that the number of deaths, like the number of cases, is being seriously undercounted, because many people will have died of the disease without having had a positive test for the virus. One way to get around this is by comparing the number of deaths this year with that which would be predicted on the basis of years past. This “excess mortality” method relies on the idea that, though official statistics may often be silent or misleading as to the cause of death, they are rarely wrong about a death actually having taken place.
The excessive force of destiny
The Economist has gathered all-cause mortality data from countries which report them weekly or monthly, a group which includes most of western Europe, some of Latin America, and a few other large countries, including the United States, Russia and South Africa (see lower part of data panel). Between March and August these countries recorded 580,000 covid-19 deaths but 900,000 excess deaths; the true toll of their share of the pandemic appears to have been 55% greater than the official one. This analysis suggests that America’s official figures underestimate the death toll by 30% or more (America’s Centres for Disease Control and Prevention have provided a similar estimate). This means that the real number of deaths to date is probably a lot closer to 300,000 than 200,000. That is about 10% of the 2.8m Americans who die each year—or, put another way, half the number who succumb to cancer. And there is plenty of 2020 still to go.
Add to all this excess mortality unreported deaths from countries where record keeping is not good enough to allow such assessments and the true death toll for the pandemic may be as high as 2m.
What can be done to slow its further rise? The response to the virus’s original vertiginous ascent was an avalanche of lockdowns; at its greatest extent, around April 10th, at least 3.5bn people were being ordered to stay at home either by national governments or regional ones. The idea was to stop the spread of the disease before health-care systems collapsed beneath its weight, and in this the lockdowns were largely successful. But in themselves they were never a solution. They severely slowed the spread of the disease while they were in place, but they could not stay in place for ever.
Stopping people interacting with each other at all, as lockdowns and limits on the size of gatherings do, is the first of three ways to lower a disease’s reproduction number, R—the number of new cases caused by each existing case. The second is reducing the likelihood that interactions lead to infection; it requires mandated levels of social distancing, hygiene measures and barriers to transmission such as face masks and visors. The third is reducing the time during which an infectious person can interact with people under any conditions. This is achieved by finding people who may recently have been infected and getting them to isolate themselves.
Ensuring that infectious people do not have time to do much infecting requires a fast and thorough test-and-trace system. Some countries, including Canada, China, Germany, Italy, Japan, Singapore and Taiwan, have successfully combined big testing programmes which provide rapid results with a well developed capacity for contact tracing and effective subsequent action. Others have foundered.
Networks and herds
Israel provides a ready example. An early and well-enforced lockdown had the expected effect of reducing new infections. But the time thus bought for developing a test-and-trace system was not well used, and the country’s emergence from lockdown was ill-thought-through. This was in part because the small circle around prime minister Binyamin Netanyahu into which power has been concentrated includes no one with relevant expertise; the health ministry is weak and politicised.
Things have been made worse by the fact that social distancing and barrier methods are being resisted by some parts of society. Synagogues and Torah seminaries in the ultra-Orthodox community and large tribal weddings in the Arab-Israeli community have been major centres of infection. While unhappy countries, like Tolstoy’s unhappy families, all differ, the elements of Israel’s dysfunction have clear parallels elsewhere.
Getting to grips with “superspreader” events is crucial to keeping R low. Close gatherings in confined spaces allow people to be infected dozens at a time. In March almost 100 were infected at a biotech conference in Boston. Many of them spread the virus on: genetic analysis subsequently concluded that 20,000 cases could be traced to that conference.
Nipping such blooms in the bud requires lots of contact tracing. Taiwan’s system logs 15-20 contacts for each person with a positive test. Contact tracers in England register four to five close contacts per positive test; those in France and Spain get just three. It also requires that people be willing to get tested in the first place. In England only 10-30% of people with covid-like symptoms ask for a test through the National Health Service. One of the reasons is that a positive test means self-isolation. Few want to undergo such restrictions, and few are good at abiding by them. In early May a survey in England found that only a fifth of those with covid symptoms had self-isolated as fully as required. The government is now seeking to penalise such breaches with fines of up to £10,000 ($12,800). That will reduce the incentive to get tested in the first place yet further.
As much of Europe comes to terms with the fact that its initial lockdowns have not put an end to its problems, there is increased interest in the Swedish experience. Unlike most of Europe, Sweden never instigated a lockdown, preferring to rely on social distancing. This resulted in a very high death rate compared with that seen in its Nordic neighbours; 58.1 per 100,000, where the rate in Denmark is 11.1, in Finland 6.19 and in Norway 4.93. It is not clear that this high death rate bought Sweden any immediate economic advantage. Its GDP dropped in the second quarter in much the same way as GDPs did elsewhere.
It is possible that by accepting so many deaths upfront Sweden may see fewer of them in the future, for two reasons. One is the phenomenon known, in a rather macabre piece of jargon, as “harvesting”. Those most likely to succumb do so early on, reducing the number of deaths seen later. The other possibility is that Sweden will benefit from a level of herd immunity: once the number of presumably immune survivors in the population grows high enough, the spread of the disease slows down because encounters between the infected and the susceptible become rare. Avoiding lockdown may conceivably have helped with this.
On the other hand, one of the advantages of lockdowns was that they provided time not just for the development of test-and-trace systems but also for doctors to get better at curing the sick. In places with good health systems, getting covid-19 is less risky today than it was six months ago. ISARIC, which researches infectious diseases, has analysed the outcomes for 68,000 patients hospitalised with covid-19; their survival rate increased from 66% in March to 84% in August. The greatest relative gains have been made among the most elderly patients. Survival rates among British people 60 and over who needed intensive care have risen from 39% to 58%.
This is largely a matter of improved case management. Putting patients on oxygen earlier helps. So does reticence about using mechanical ventilators and a greater awareness of the disease’s effects beyond the lungs, such as its tendency to provoke clotting disorders.
Nouvelle vague
As for treatments, two already widely available steroids, dexamethasone and hydrocortisone, increase survival by reducing inflammation. Avigan, a Japanese flu drug, has been found to hasten recovery. Remdesivir, a drug designed to fight other viruses, and convalescent plasma, which provides patients with antibodies from people who have already recovered from the disease, seem to offer marginal benefits.
Many consider antibodies tailor-made for the job by biotech companies a better bet; over the past few years they have provided a breakthrough in the treatment of Ebola. The American government has paid $450m for supplies of a promising two-antibody treatment being developed by Regeneron. That will be enough for between 70,000 and 300,000 doses, depending on what stage of the disease the patients who receive it have reached. Regeneron is now working with Roche, another drug company, to crank up production worldwide. But antibodies will remain expensive, and the need to administer them intravenously limits their utility.
It is tempting to look to better treatment for the reason why, although diagnosed cases in Europe have been climbing steeply into what is being seen as a second wave, the number of deaths has not followed: indeed it has, as yet, barely moved. The main reason, though, is simpler. During the first wave little testing was being done, and so many infections were being missed. Now lots of testing is being done, and vastly more infections are being picked up. Correct for this distortion and you see that the first wave was far larger than what is being seen today, which makes today’s lower death rate much less surprising (see data panel).
The coming winter is nevertheless worrying. Exponential growth can bring change quickly when R gets significantly above one. There is abundant evidence of what Katrine Bach Habersaat of the WHO calls “pandemic fatigue” eating away at earlier behavioural change, as well as increasing resentment of other public-health measures. YouGov, a pollster, has been tracking opinion on such matters in countries around the world. It has seen support for quarantining people who have had contact with someone infected fall a bit in Asia and rather more in the West, where it is down from 78% to 63%. In America it has fallen to 55%.
It is true that infection rates are currently climbing mostly among the young. But the young do not live in bubbles. Recent figures from Bouches-du-Rhône, the French department which includes Marseille, show clearly how a spike of cases in the young becomes, in a few weeks, an increase in cases at all ages.
As the fear of such spikes increases, though, so does the hope that they will not be recurring all that much longer. Pfizer, which has promising vaccine candidate in efficacy trials, has previously said that it will seek regulatory review of preliminary results in October, though new standards at the Food and Drug Administration may not allow it to do so in America quite that soon. Three other candidates, from AstraZeneca, Moderna and J&J, are nipping at Pfizer’s heels. The J&J vaccine is a newcomer; it entered efficacy trials only on September 23rd. But whereas the other vaccines need a booster a month after the first jab, the J&J vaccine is administered just once, which will make the trial quicker; it could have preliminary results in November.
None of the companies will have all the trial data they are planning for until the first quarter of next year. But in emergencies regulators can authorise a vaccine’s use based on interim analysis if it meets a minimum standard (in this case, protection of half those who are vaccinated). Authorisation for use under such conditions would still make such a vaccine more credible than those already in use in China and Russia, neither of which was tested for efficacy at all. But there have been fears that American regulators may, in the run up to the presidential election, set the bar too low. Making an only-just-good-enough vaccine available might see social-distancing collapse and infections increase; alternatively, a perfectly decent vaccine approved in a politically toxic way might not be taken up as widely as it should be.
In either case, though, the practical availability of a vaccine will lag behind any sort of approval. In the long run, billions of doses could be needed. A global coalition of countries known as Covax wants to distribute 2bn by the end of 2021—which will only be enough for 1bn people if the vaccine in question, like Pfizer’s or AstraZeneca’s, needs to be administered twice. The world’s largest manufacturer of vaccines, the Serum Institute in India, recently warned that there will not be enough supplies for universal inoculation until 2024 at the earliest.
Even if everything goes swimmingly, it is hard to see distribution extending beyond a small number of front-line health and care workers this year. But the earlier vaccines are pushed out, the better. The data panel on this page looks at the results of vaccinating earlier versus later in a hypothetical population not that unlike Britain’s. Vaccination at a slower rate which starts earlier sees fewer eventual infections than a much more ambitious campaign started later. At the same time increases in R—which might come about if social distancing and similar measures fall away as vaccination becomes real—make all scenarios worse.
By next winter the covid situation in developed countries should be improved. What level of immunity the vaccines will provide, and for how long, remains to be seen. But few expect none of them to work at all.
Access to the safety thus promised will be unequal, both within countries and between them. Some will see loved ones who might have been vaccinated die because they were not. Minimising such losses will require getting more people vaccinated more quickly than has ever been attempted before. It is a prodigious organisational challenge—and one which, judging by this year’s experience, some governments will handle considerably better than others. ■
This article appeared in the Briefing section of the print edition under the headline “Grim tallies”
Earlier this summer, the Summit supercomputer at Oak Ridge National Lab in Tennessee set about crunching data on more than 40,000 genes from 17,000 genetic samples in an effort to better understand Covid-19. Summit is the second-fastest computer in the world, but the process — which involved analyzing 2.5 billion genetic combinations — still took more than a week.
When Summit was done, researchers analyzed the results. It was, in the words of Dr. Daniel Jacobson, lead researcher and chief scientist for computational systems biology at Oak Ridge, a “eureka moment.” The computer had revealed a new theory about how Covid-19 impacts the body: the bradykinin hypothesis. The hypothesis provides a model that explains many aspects of Covid-19, including some of its most bizarre symptoms. It also suggests 10-plus potential treatments, many of which are already FDA approved. Jacobson’s group published their results in a paper in the journal eLife in early July.
According to the team’s findings, a Covid-19 infection generally begins when the virus enters the body through ACE2 receptors in the nose, (The receptors, which the virus is known to target, are abundant there.) The virus then proceeds through the body, entering cells in other places where ACE2 is also present: the intestines, kidneys, and heart. This likely accounts for at least some of the disease’s cardiac and GI symptoms.
But once Covid-19 has established itself in the body, things start to get really interesting. According to Jacobson’s group, the data Summit analyzed shows that Covid-19 isn’t content to simply infect cells that already express lots of ACE2 receptors. Instead, it actively hijacks the body’s own systems, tricking it into upregulating ACE2 receptors in places where they’re usually expressed at low or medium levels, including the lungs.
In this sense, Covid-19 is like a burglar who slips in your unlocked second-floor window and starts to ransack your house. Once inside, though, they don’t just take your stuff — they also throw open all your doors and windows so their accomplices can rush in and help pillage more efficiently.
The renin–angiotensin system (RAS) controls many aspects of the circulatory system, including the body’s levels of a chemical called bradykinin, which normally helps to regulate blood pressure. According to the team’s analysis, when the virus tweaks the RAS, it causes the body’s mechanisms for regulating bradykinin to go haywire. Bradykinin receptors are resensitized, and the body also stops effectively breaking down bradykinin. (ACE normally degrades bradykinin, but when the virus downregulates it, it can’t do this as effectively.)
The end result, the researchers say, is to release a bradykinin storm — a massive, runaway buildup of bradykinin in the body. According to the bradykinin hypothesis, it’s this storm that is ultimately responsible for many of Covid-19’s deadly effects. Jacobson’s team says in their paper that “the pathology of Covid-19 is likely the result of Bradykinin Storms rather than cytokine storms,” which had been previously identified in Covid-19 patients, but that “the two may be intricately linked.” Other papers had previously identified bradykinin storms as a possible cause of Covid-19’s pathologies.
Covid-19 is like a burglar who slips in your unlocked second-floor window and starts to ransack your house.
As bradykinin builds up in the body, it dramatically increases vascular permeability. In short, it makes your blood vessels leaky. This aligns with recent clinical data, which increasingly views Covid-19 primarily as a vascular disease, rather than a respiratory one. But Covid-19 still has a massive effect on the lungs. As blood vessels start to leak due to a bradykinin storm, the researchers say, the lungs can fill with fluid. Immune cells also leak out into the lungs, Jacobson’s team found, causing inflammation.
And Covid-19 has another especially insidious trick. Through another pathway, the team’s data shows, it increases production of hyaluronic acid (HLA) in the lungs. HLA is often used in soaps and lotions for its ability to absorb more than 1,000 times its weight in fluid. When it combines with fluid leaking into the lungs, the results are disastrous: It forms a hydrogel, which can fill the lungs in some patients. According to Jacobson, once this happens, “it’s like trying to breathe through Jell-O.”
This may explain why ventilators have proven less effective in treating advanced Covid-19 than doctors originally expected, based on experiences with other viruses. “It reaches a point where regardless of how much oxygen you pump in, it doesn’t matter, because the alveoli in the lungs are filled with this hydrogel,” Jacobson says. “The lungs become like a water balloon.” Patients can suffocate even while receiving full breathing support.
The bradykinin hypothesis also extends to many of Covid-19’s effects on the heart. About one in five hospitalized Covid-19 patients have damage to their hearts, even if they never had cardiac issues before. Some of this is likely due to the virus infecting the heart directly through its ACE2 receptors. But the RAS also controls aspects of cardiac contractions and blood pressure. According to the researchers, bradykinin storms could create arrhythmias and low blood pressure, which are often seen in Covid-19 patients.
The bradykinin hypothesis also accounts for Covid-19’s neurological effects, which are some of the most surprising and concerning elements of the disease. These symptoms (which include dizziness, seizures, delirium, and stroke) are present in as many as half of hospitalized Covid-19 patients. According to Jacobson and his team, MRI studies in France revealed that many Covid-19 patients have evidence of leaky blood vessels in their brains.
Bradykinin — especially at high doses — can also lead to a breakdown of the blood-brain barrier. Under normal circumstances, this barrier acts as a filter between your brain and the rest of your circulatory system. It lets in the nutrients and small molecules that the brain needs to function, while keeping out toxins and pathogens and keeping the brain’s internal environment tightly regulated.
If bradykinin storms cause the blood-brain barrier to break down, this could allow harmful cells and compounds into the brain, leading to inflammation, potential brain damage, and many of the neurological symptoms Covid-19 patients experience. Jacobson told me, “It is a reasonable hypothesis that many of the neurological symptoms in Covid-19 could be due to an excess of bradykinin. It has been reported that bradykinin would indeed be likely to increase the permeability of the blood-brain barrier. In addition, similar neurological symptoms have been observed in other diseases that result from an excess of bradykinin.”
Increased bradykinin levels could also account for other common Covid-19 symptoms. ACE inhibitors — a class of drugs used to treat high blood pressure — have a similar effect on the RAS system as Covid-19, increasing bradykinin levels. In fact, Jacobson and his team note in their paper that “the virus… acts pharmacologically as an ACE inhibitor” — almost directly mirroring the actions of these drugs.
By acting like a natural ACE inhibitor, Covid-19 may be causing the same effects that hypertensive patients sometimes get when they take blood pressure–lowering drugs. ACE inhibitors are known to cause a dry cough and fatigue, two textbook symptoms of Covid-19. And they can potentially increase blood potassium levels, which has also been observed in Covid-19 patients. The similarities between ACE inhibitor side effects and Covid-19 symptoms strengthen the bradykinin hypothesis, the researchers say.
ACE inhibitors are also known to cause a loss of taste and smell. Jacobson stresses, though, that this symptom is more likely due to the virus “affecting the cells surrounding olfactory nerve cells” than the direct effects of bradykinin.
Though still an emerging theory, the bradykinin hypothesis explains several other of Covid-19’s seemingly bizarre symptoms. Jacobson and his team speculate that leaky vasculature caused by bradykinin storms could be responsible for “Covid toes,” a condition involving swollen, bruised toes that some Covid-19 patients experience. Bradykinin can also mess with the thyroid gland, which could produce the thyroid symptoms recently observed in some patients.
The bradykinin hypothesis could also explain some of the broader demographic patterns of the disease’s spread. The researchers note that some aspects of the RAS system are sex-linked, with proteins for several receptors (such as one called TMSB4X) located on the X chromosome. This means that “women… would have twice the levels of this protein than men,” a result borne out by the researchers’ data. In their paper, Jacobson’s team concludes that this “could explain the lower incidence of Covid-19 induced mortality in women.” A genetic quirk of the RAS could be giving women extra protection against the disease.
The bradykinin hypothesis provides a model that “contributes to a better understanding of Covid-19” and “adds novelty to the existing literature,” according to scientists Frank van de Veerdonk, Jos WM van der Meer, and Roger Little, who peer-reviewed the team’s paper. It predicts nearly all the disease’s symptoms, even ones (like bruises on the toes) that at first appear random, and further suggests new treatments for the disease.
As Jacobson and team point out, several drugs target aspects of the RAS and are already FDA approved to treat other conditions. They could arguably be applied to treating Covid-19 as well. Several, like danazol, stanozolol, and ecallantide, reduce bradykinin production and could potentially stop a deadly bradykinin storm. Others, like icatibant, reduce bradykinin signaling and could blunt its effects once it’s already in the body.
Interestingly, Jacobson’s team also suggests vitamin D as a potentially useful Covid-19 drug. The vitamin is involved in the RAS system and could prove helpful by reducing levels of another compound, known as REN. Again, this could stop potentially deadly bradykinin storms from forming. The researchers note that vitamin D has already been shown to help those with Covid-19. The vitamin is readily available over the counter, and around 20% of the population is deficient. If indeed the vitamin proves effective at reducing the severity of bradykinin storms, it could be an easy, relatively safe way to reduce the severity of the virus.
Other compounds could treat symptoms associated with bradykinin storms. Hymecromone, for example, could reduce hyaluronic acid levels, potentially stopping deadly hydrogels from forming in the lungs. And timbetasin could mimic the mechanism that the researchers believe protects women from more severe Covid-19 infections. All of these potential treatments are speculative, of course, and would need to be studied in a rigorous, controlled environment before their effectiveness could be determined and they could be used more broadly.
Covid-19 stands out for both the scale of its global impact and the apparent randomness of its many symptoms. Physicians have struggled to understand the disease and come up with a unified theory for how it works. Though as of yet unproven, the bradykinin hypothesis provides such a theory. And like all good hypotheses, it also provides specific, testable predictions — in this case, actual drugs that could provide relief to real patients.
The researchers are quick to point out that “the testing of any of these pharmaceutical interventions should be done in well-designed clinical trials.” As to the next step in the process, Jacobson is clear: “We have to get this message out.” His team’s finding won’t cure Covid-19. But if the treatments it points to pan out in the clinic, interventions guided by the bradykinin hypothesis could greatly reduce patients’ suffering — and potentially save lives.
HUMANS ARE lucky to live a hundred years. Oak trees may live a thousand; mayflies, in their adult form, a single day. But they are all alive in the same way. They are made up of cells which embody flows of energy and stores of information. Their metabolisms make use of that energy, be it from sunlight or food, to build new molecules and break down old ones, using mechanisms described in the genes they inherited and may, or may not, pass on.
It is this endlessly repeated, never quite perfect reproduction which explains why oak trees, humans, and every other plant, fungus or single-celled organism you have ever seen or felt the presence of are all alive in the same way. It is the most fundamental of all family resemblances. Go far enough up any creature’s family tree and you will find an ancestor that sits in your family tree, too. Travel further and you will find what scientists call the last universal common ancestor, LUCA. It was not the first living thing. But it was the one which set the template for the life that exists today.
And then there are viruses. In viruses the link between metabolism and genes that binds together all life to which you are related, from bacteria to blue whales, is broken. Viral genes have no cells, no bodies, no metabolism of their own. The tiny particles, “virions”, in which those genes come packaged—the dot-studded disks of coronaviruses, the sinister, sinuous windings of Ebola, the bacteriophages with their science-fiction landing-legs that prey on microbes—are entirely inanimate. An individual animal, or plant, embodies and maintains the restless metabolism that made it. A virion is just an arrangement of matter.
The virus is not the virion. The virus is a process, not a thing. It is truly alive only in the cells of others, a virtual organism running on borrowed hardware to produce more copies of its genome. Some bide their time, letting the cell they share the life of live on. Others immediately set about producing enough virions to split their hosts from stem to stern.
The virus has no plan or desire. The simplest purposes of the simplest life—to maintain the difference between what is inside the cell and what is outside, to move towards one chemical or away from another—are entirely beyond it. It copies itself in whatever way it does simply because it has copied itself that way before, in other cells, in other hosts.
That is why, asked whether viruses are alive, Eckard Wimmer, a chemist and biologist who works at the State University of New York, Stony Brook, offers a yes-and-no. Viruses, he says, “alternate between nonliving and living phases”. He should know. In 2002 he became the first person in the world to take an array of nonliving chemicals and build a virion from scratch—a virion which was then able to get itself reproduced by infecting cells.
The fact that viruses have only a tenuous claim to being alive, though, hardly reduces their impact on things which are indubitably so. No other biological entities are as ubiquitous, and few as consequential. The number of copies of their genes to be found on Earth is beyond astronomical. There are hundreds of billions of stars in the Milky Way galaxy and a couple of trillion galaxies in the observable universe. The virions in the surface waters of any smallish sea handily outnumber all the stars in all the skies that science could ever speak of.
Back on Earth, viruses kill more living things than any other type of predator. They shape the balance of species in ecosystems ranging from those of the open ocean to that of the human bowel. They spur evolution, driving natural selection and allowing the swapping of genes.
They may have been responsible for some of the most important events in the history of life, from the appearance of complex multicellular organisms to the emergence of DNA as a preferred genetic material. The legacy they have left in the human genome helps produce placentas and may shape the development of the brain. For scientists seeking to understand life’s origin, they offer a route into the past separate from the one mapped by humans, oak trees and their kin. For scientists wanting to reprogram cells and mend metabolisms they offer inspiration—and powerful tools.
II A lifestyle for genes
THE IDEA of a last universal common ancestor provides a plausible and helpful, if incomplete, answer to where humans, oak trees and their ilk come from. There is no such answer for viruses. Being a virus is not something which provides you with a place in a vast, coherent family tree. It is more like a lifestyle—a way of being which different genes have discovered independently at different times. Some viral lineages seem to have begun quite recently. Others have roots that comfortably predate LUCA itself.
Disparate origins are matched by disparate architectures for information storage and retrieval. In eukaryotes—creatures, like humans, mushrooms and kelp, with complex cells—as in their simpler relatives, the bacteria and archaea, the genes that describe proteins are written in double-stranded DNA. When a particular protein is to be made, the DNA sequence of the relevant gene acts as a template for the creation of a complementary molecule made from another nucleic acid, RNA. This messenger RNA (mRNA) is what the cellular machinery tasked with translating genetic information into proteins uses in order to do so.
Because they, too, need to have proteins made to their specifications, viruses also need to produce mRNAs. But they are not restricted to using double-stranded DNA as a template. Viruses store their genes in a number of different ways, all of which require a different mechanism to produce mRNAs. In the early 1970s David Baltimore, one of the great figures of molecular biology, used these different approaches to divide the realm of viruses into seven separate classes (see diagram).
In four of these seven classes the viruses store their genes not in DNA but in RNA. Those of Baltimore group three use double strands of RNA. In Baltimore groups four and five the RNA is single-stranded; in group four the genome can be used directly as an mRNA; in group five it is the template from which mRNA must be made. In group six—the retroviruses, which include HIV—the viral RNA is copied into DNA, which then provides a template for mRNAs.
Because uninfected cells only ever make RNA on the basis of a DNA template, RNA-based viruses need distinctive molecular mechanisms those cells lack. Those mechanisms provide medicine with targets for antiviral attacks. Many drugs against HIV take aim at the system that makes DNA copies of RNA templates. Remdesivir (Veklury), a drug which stymies the mechanism that the simpler RNA viruses use to recreate their RNA genomes, was originally developed to treat hepatitis C (group four) and subsequently tried against the Ebola virus (group five). It is now being used against SARS–CoV-2 (group four), the covid-19 virus.
Studies of the gene for that RNA-copying mechanism, RdRp, reveal just how confusing virus genealogy can be. Some viruses in groups three, four and five seem, on the basis of their RdRp-gene sequence, more closely related to members of one of the other groups than they are to all the other members of their own group. This may mean that quite closely related viruses can differ in the way they store their genomes; it may mean that the viruses concerned have swapped their RdRp genes. When two viruses infect the same cell at the same time such swaps are more or less compulsory. They are, among other things, one of the mechanisms by which viruses native to one species become able to infect another.
How do genes take on the viral lifestyle in the first place? There are two plausible mechanisms. Previously free-living creatures could give up metabolising and become parasitic, using other creatures’ cells as their reproductive stage. Alternatively genes allowed a certain amount of independence within one creature could have evolved the means to get into other creatures.
Living creatures contain various apparently independent bits of nucleic acid with an interest in reproducing themselves. The smallest, found exclusively in plants, are tiny rings of RNA called viroids, just a few hundred genetic letters long. Viroids replicate by hijacking a host enzyme that normally makes mRNAs. Once attached to a viroid ring, the enzyme whizzes round and round it, unable to stop, turning out a new copy of the viroid with each lap.
Viroids describe no proteins and do no good. Plasmids—somewhat larger loops of nucleic acid found in bacteria—do contain genes, and the proteins they describe can be useful to their hosts. Plasmids are sometimes, therefore, regarded as detached parts of a bacteria’s genome. But that detachment provides a degree of autonomy. Plasmids can migrate between bacterial cells, not always of the same species. When they do so they can take genetic traits such as antibiotic resistance from their old host to their new one.
Recently, some plasmids have been implicated in what looks like a progression to true virus-hood. A genetic analysis by Mart Krupovic of the Pasteur Institute suggests that the Circular Rep-Encoding Single-Strand-DNA (CRESS–DNA) viruses, which infect bacteria, evolved from plasmids. He thinks that a DNA copy of the genes that another virus uses to create its virions, copied into a plasmid by chance, provided it with a way out of the cell. The analysis strongly suggests that CRESS–DNA viruses, previously seen as a pretty closely related group, have arisen from plasmids this way on three different occasions.
Such jailbreaks have probably been going on since very early on in the history of life. As soon as they began to metabolise, the first proto-organisms would have constituted a niche in which other parasitic creatures could have lived. And biology abhors a vacuum. No niche goes unfilled if it is fillable.
It is widely believed that much of the evolutionary period between the origin of life and the advent of LUCA was spent in an “RNA world”—one in which that versatile substance both stored information, as DNA now does, and catalysed chemical reactions, as proteins now do. Set alongside the fact that some viruses use RNA as a storage medium today, this strongly suggests that the first to adopt the viral lifestyle did so too. Patrick Forterre, an evolutionary biologist at the Pasteur Institute with a particular interest in viruses (and the man who first popularised the term LUCA) thinks that the “RNA world” was not just rife with viruses. He also thinks they may have brought about its end.
The difference between DNA and RNA is not large: just a small change to one of the “letters” used to store genetic information and a minor modification to the backbone to which these letters are stuck. And DNA is a more stable molecule in which to store lots of information. But that is in part because DNA is inert. An RNA-world organism which rewrote its genes into DNA would cripple its metabolism, because to do so would be to lose the catalytic properties its RNA provided.
An RNA-world virus, having no metabolism of its own to undermine, would have had no such constraints if shifting to DNA offered an advantage. Dr Forterre suggests that this advantage may have lain in DNA’s imperviousness to attack. Host organisms today have all sorts of mechanisms for cutting up viral nucleic acids they don’t like the look of—mechanisms which biotechnologists have been borrowing since the 1970s, most recently in the form of tools based on a bacterial defence called CRISPR. There is no reason to imagine that the RNA-world predecessors of today’s cells did not have similar shears at their disposal. And a virus that made the leap to DNA would have been impervious to their blades.
Genes and the mechanisms they describe pass between viruses and hosts, as between viruses and viruses, all the time. Once some viruses had evolved ways of writing and copying DNA, their hosts would have been able to purloin them in order to make back-up copies of their RNA molecules. And so what began as a way of protecting viral genomes would have become the way life stores all its genes—except for those of some recalcitrant, contrary viruses.
III The scythes of the seas
IT IS A general principle in biology that, although in terms of individual numbers herbivores outnumber carnivores, in terms of the number of species carnivores outnumber herbivores. Viruses, however, outnumber everything else in every way possible.
This makes sense. Though viruses can induce host behaviours that help them spread—such as coughing—an inert virion boasts no behaviour of its own that helps it stalk its prey. It infects only that which it comes into contact with. This is a clear invitation to flood the zone. In 1999 Roger Hendrix, a virologist, suggested that a good rule of thumb might be ten virions for every living individual creature (the overwhelming majority of which are single-celled bacteria and archaea). Estimates of the number of such creatures on the planet come out in the region of 1029-1030. If the whole Earth were broken up into pebbles, and each of those pebbles smashed into tens of thousands of specks of grit, you would still have fewer pieces of grit than the world has virions. Measurements, as opposed to estimates, produce numbers almost as arresting. A litre of seawater may contain more than 100bn virions; a kilogram of dried soil perhaps a trillion.
Metagenomics, a part of biology that looks at all the nucleic acid in a given sample to get a sense of the range of life forms within it, reveals that these tiny throngs are highly diverse. A metagenomic analysis of two surveys of ocean life, the Tara Oceans and Malaspina missions, by Ahmed Zayed of Ohio State University, found evidence of 200,000 different species of virus. These diverse species play an enormous role in the ecology of the oceans.
A litre of seawater may contain 100bn virions; a kilogram of dried soil perhaps a trillion
On land, most of the photosynthesis which provides the biomass and energy needed for life takes place in plants. In the oceans, it is overwhelmingly the business of various sorts of bacteria and algae collectively known as phytoplankton. These creatures reproduce at a terrific rate, and viruses kill them at a terrific rate, too. According to work by Curtis Suttle of the University of British Columbia, bacterial phytoplankton typically last less than a week before being killed by viruses.
This increases the overall productivity of the oceans by helping bacteria recycle organic matter (it is easier for one cell to use the contents of another if a virus helpfully lets them free). It also goes some way towards explaining what the great mid-20th-century ecologist G. Evelyn Hutchinson called “the paradox of the plankton”. Given the limited nature of the resources that single-celled plankton need, you would expect a few species particularly well adapted to their use to dominate the ecosystem. Instead, the plankton display great variety. This may well be because whenever a particular form of plankton becomes dominant, its viruses expand with it, gnawing away at its comparative success.
It is also possible that this endless dance of death between viruses and microbes sets the stage for one of evolution’s great leaps forward. Many forms of single-celled plankton have molecular mechanisms that allow them to kill themselves. They are presumably used when one cell’s sacrifice allows its sister cells—which are genetically identical—to survive. One circumstance in which such sacrifice seems to make sense is when a cell is attacked by a virus. If the infected cell can kill itself quickly (a process called apoptosis) it can limit the number of virions the virus is able to make. This lessens the chances that other related cells nearby will die. Some bacteria have been shown to use this strategy; many other microbes are suspected of it.
There is another situation where self-sacrifice is becoming conduct for a cell: when it is part of a multicellular organism. As such organisms grow, cells that were once useful to them become redundant; they have to be got rid of. Eugene Koonin of America’s National Institutes of Health and his colleagues have explored the idea that virus-thwarting self-sacrifice and complexity-permitting self-sacrifice may be related, with the latter descended from the former. Dr Koonin’s model also suggests that the closer the cells are clustered together, the more likely this act of self-sacrifice is to have beneficial consequences.
For such profound propinquity, move from the free-flowing oceans to the more structured world of soil, where potential self-sacrificers can nestle next to each other. Its structure makes soil harder to sift for genes than water is. But last year Mary Firestone of the University of California, Berkeley, and her colleagues used metagenomics to count 3,884 new viral species in a patch of Californian grassland. That is undoubtedly an underestimate of the total diversity; their technique could see only viruses with RNA genomes, thus missing, among other things, most bacteriophages.
Metagenomics can also be applied to biological samples, such as bat guano in which it picks up viruses from both the bats and their food. But for the most part the finding of animal viruses requires more specific sampling. Over the course of the 2010s PREDICT, an American-government project aimed at finding animal viruses, gathered over 160,000 animal and human tissue samples from 35 countries and discovered 949 novel viruses.
The people who put together PREDICT now have grander plans. They want a Global Virome Project to track down all the viruses native to the world’s 7,400 species of mammals and waterfowl—the reservoirs most likely to harbour viruses capable of making the leap into human beings. In accordance with the more-predator-species-than-prey rule they expect such an effort would find about 1.5m viruses, of which around 700,000 might be able to infect humans. A planning meeting in 2018 suggested that such an undertaking might take ten years and cost $4bn. It looked like a lot of money then. Today those arguing for a system that can provide advance warning of the next pandemic make it sound pretty cheap.
IV Leaving their mark
THE TOLL which viruses have exacted throughout history suggests that they have left their mark on the human genome: things that kill people off in large numbers are powerful agents of natural selection. In 2016 David Enard, then at Stanford University and now at the University of Arizona, made a stab at showing just how much of the genome had been thus affected.
He and his colleagues started by identifying almost 10,000 proteins that seemed to be produced in all the mammals that had had their genomes sequenced up to that point. They then made a painstaking search of the scientific literature looking for proteins that had been shown to interact with viruses in some way or other. About 1,300 of the 10,000 turned up. About one in five of these proteins was connected to the immune system, and thus could be seen as having a professional interest in viral interaction. The others appeared to be proteins which the virus made use of in its attack on the host. The two cell-surface proteins that SARS–CoV-2 uses to make contact with its target cells and inveigle its way into them would fit into this category.
The researchers then compared the human versions of the genes for their 10,000 proteins with those in other mammals, and applied a statistical technique that distinguishes changes that have no real impact from the sort of changes which natural selection finds helpful and thus tries to keep. Genes for virus-associated proteins turned out to be evolutionary hotspots: 30% of all the adaptive change was seen in the genes for the 13% of the proteins which interacted with viruses. As quickly as viruses learn to recognise and subvert such proteins, hosts must learn to modify them.
A couple of years later, working with Dmitri Petrov at Stanford, Dr Enard showed that modern humans have borrowed some of these evolutionary responses to viruses from their nearest relatives. Around 2-3% of the DNA in an average European genome has Neanderthal origins, a result of interbreeding 50,000 to 30,000 years ago. For these genes to have persisted they must be doing something useful—otherwise natural selection would have removed them. Dr Enard and Dr Petrov found that a disproportionate number described virus-interacting proteins; of the bequests humans received from their now vanished relatives, ways to stay ahead of viruses seem to have been among the most important.
Viruses do not just shape the human genome through natural selection, though. They also insert themselves into it. At least a twelfth of the DNA in the human genome is derived from viruses; by some measures the total could be as high as a quarter.
Retroviruses like HIV are called retro because they do things backwards. Where cellular organisms make their RNA from DNA templates, retroviruses do the reverse, making DNA copies of their RNA genomes. The host cell obligingly makes these copies into double-stranded DNA which can be stitched into its own genome. If this happens in a cell destined to give rise to eggs or sperm, the viral genes are passed from parent to offspring, and on down the generations. Such integrated viral sequences, known as endogenous retroviruses (ERVs), account for 8% of the human genome.
This is another example of the way the same viral trick can be discovered a number of times. Many bacteriophages are also able to stitch copies of their genome into their host’s DNA, staying dormant, or “temperate”, for generations. If the cell is doing well and reproducing regularly, this quiescence is a good way for the viral genes to make more copies of themselves. When a virus senses that its easy ride may be coming to an end, though—for example, if the cell it is in shows signs of stress—it will abandon ship. What was latent becomes “lytic” as the viral genes produce a sufficient number of virions to tear the host apart.
Though some of their genes are associated with cancers, in humans ERVs do not burst back into action in later generations. Instead they have proved useful resources of genetic novelty. In the most celebrated example, at least ten different mammalian lineages make use of a retroviral gene for one of their most distinctively mammalian activities: building a placenta.
The placenta is a unique organ because it requires cells from the mother and the fetus to work together in order to pass oxygen and sustenance in one direction and carbon dioxide and waste in the other. One way this intimacy is achieved safely is through the creation of a tissue in which the membranes between cells are broken down to form a continuous sheet of cellular material.
The protein that allows new cells to merge themselves with this layer, syncytin-1, was originally used by retroviruses to join the external membranes of their virions to the external membranes of cells, thus gaining entry for the viral proteins and nucleic acids. Not only have different sorts of mammals co-opted this membrane-merging trick—other creatures have made use of it, too. The mabuya, a long-tailed skink which unusually for a lizard nurtures its young within its body, employs a retroviral syncytin protein to produce a mammalian-looking placenta. The most recent shared ancestor of mabuyas and mammals died out 80m years before the first dinosaur saw the light of day, but both have found the same way to make use of the viral gene.
You put your line-1 in, you take your line-1 out
This is not the only way that animals make use of their ERVs. Evidence has begun to accumulate that genetic sequences derived from ERVs are quite frequently used to regulate the activity of genes of more conventional origin. In particular, RNA molecules transcribed from an ERV called HERV-K play a crucial role in providing the stem cells found in embryos with their “pluripotency”—the ability to create specialised daughter cells of various different types. Unfortunately, when expressed in adults HERV-K can also be responsible for cancers of the testes.
As well as containing lots of semi-decrepit retroviruses that can be stripped for parts, the human genome also holds a great many copies of a “retrotransposon” called LINE-1. This a piece of DNA with a surprisingly virus-like way of life; it is thought by some biologists to have, like ERVs, a viral origin. In its full form, LINE-1 is a 6,000-letter sequence of DNA which describes a “reverse transcriptase” of the sort that retroviruses use to make DNA from their RNA genomes. When LINE-1 is transcribed into an mRNA and that mRNA subsequently translated to make proteins, the reverse transcriptase thus created immediately sets to work on the mRNA used to create it, using it as the template for a new piece of DNA which is then inserted back into the genome. That new piece of DNA is in principle identical to the piece that acted as the mRNA’s original template. The LINE-1 element has made a copy of itself.
In the 100m years or so that this has been going on in humans and the species from which they are descended the LINE-1 element has managed to pepper the genome with a staggering 500,000 copies of itself. All told, 17% of the human genome is taken up by these copies—twice as much as by the ERVs.
Most of the copies are severely truncated and incapable of copying themselves further. But some still have the knack, and this capability may be being put to good use. Fred Gage and his colleagues at the Salk Institute for Biological Studies, in San Diego, argue that LINE-1 elements have an important role in the development of the brain. In 2005 Dr Gage discovered that in mouse embryos—specifically, in the brains of those embryos—about 3,000 LINE-1 elements are still able to operate as retrotransposons, putting new copies of themselves into the genome of a cell and thus of all its descendants.
Brains develop through proliferation followed by pruning. First, nerve cells multiply pell-mell; then the cell-suicide process that makes complex life possible prunes them back in a way that looks a lot like natural selection. Dr Gage suspects that the movement of LINE-1 transposons provides the variety in the cell population needed for this selection process. Choosing between cells with LINE-1 in different places, he thinks, could be a key part of the process from which the eventual neural architecture emerges. What is true in mice is, as he showed in 2009, true in humans, too. He is currently developing a technique for looking at the process in detail by comparing, post mortem, the genomes of different brain cells from single individuals to see if their LINE-1 patterns vary in the ways that his theory would predict.
V Promised lands
HUMAN EVOLUTION may have used viral genes to make big-brained live-born life possible; but viral evolution has used them to kill off those big brains on a scale that is easily forgotten. Compare the toll to that of war. In the 20th century, the bloodiest in human history, somewhere between 100m and 200m people died as a result of warfare. The number killed by measles was somewhere in the same range; the number who died of influenza probably towards the top of it; and the number killed by smallpox—300m-500m—well beyond it. That is why the eradication of smallpox from the wild, achieved in 1979 by a globally co-ordinated set of vaccination campaigns, stands as one of the all-time-great humanitarian triumphs.
Other eradications should eventually follow. Even in their absence, vaccination has led to a steep decline in viral deaths. But viruses against which there is no vaccine, either because they are very new, like SARS–CoV-2, or peculiarly sneaky, like HIV, can still kill millions.
Reducing those tolls is a vital aim both for research and for public-health policy. Understandably, a far lower priority is put on the benefits that viruses can bring. This is mostly because they are as yet much less dramatic. They are also much less well understood.
The viruses most prevalent in the human body are not those which infect human cells. They are those which infect the bacteria that live on the body’s surfaces, internal and external. The average human “microbiome” harbours perhaps 100trn of these bacteria. And where there are bacteria, there are bacteriophages shaping their population.
The microbiome is vital for good health; when it goes wrong it can mess up a lot else. Gut bacteria seem to have a role in maintaining, and possibly also causing, obesity in the well-fed and, conversely, in tipping the poorly fed into a form of malnutrition called kwashiorkor. Ill-regulated gut bacteria have also been linked, if not always conclusively, with diabetes, heart disease, cancers, depression and autism. In light of all this, the question “who guards the bacterial guardians?” is starting to be asked.
The viruses that prey on the bacteria are an obvious answer. Because the health of their host’s host—the possessor of the gut they find themselves in—matters to these phages, they have an interest in keeping the microbiome balanced. Unbalanced microbiomes allow pathogens to get a foothold. This may explain a curious detail of a therapy now being used as a treatment of last resort against Clostridium difficile, a bacterium that causes life-threatening dysentery. The therapy in question uses a transfusion of faecal matter, with its attendant microbes, from a healthy individual to reboot the patient’s microbiome. Such transplants, it appears, are more likely to succeed if their phage population is particularly diverse.
Medicine is a very long way from being able to use phages to fine-tune the microbiome. But if a way of doing so is found, it will not in itself be a revolution. Attempts to use phages to promote human health go back to their discovery in 1917, by Félix d’Hérelle, a French microbiologist, though those early attempts at therapy were not looking to restore balance and harmony. On the basis that the enemy of my enemy is my friend, doctors simply treated bacterial infections with phages thought likely to kill the bacteria.
The arrival of antibiotics saw phage therapy abandoned in most places, though it persisted in the Soviet Union and its satellites. Various biotechnology companies think they may now be able to revive the tradition—and make it more effective. One option is to remove the bits of the viral genome that let phages settle down to a temperate life in a bacterial genome, leaving them no option but to keep on killing. Another is to write their genes in ways that avoid the defences with which bacteria slice up foreign DNA.
The hope is that phage therapy will become a backup in difficult cases, such as infection with antibiotic-resistant bugs. There have been a couple of well-publicised one-off successes outside phage therapy’s post-Soviet homelands. In 2016 Tom Patterson, a researcher at the University of California, San Diego, was successfully treated for an antibiotic-resistant bacterial infection with specially selected (but un-engineered) phages. In 2018 Graham Hatfull of the University of Pittsburgh used a mixture of phages, some engineered so as to be incapable of temperance, to treat a 16-year-old British girl who had a bad bacterial infection after a lung transplant. Clinical trials are now getting under way for phage treatments aimed at urinary-tract infections caused by Escherichia coli, Staphylococcus aureus infections that can lead to sepsis and Pseudomonas aeruginosa infections that cause complications in people who have cystic fibrosis.
Viruses which attack bacteria are not the only ones genetic engineers have their eyes on. Engineered viruses are of increasing interest to vaccine-makers, to cancer researchers and to those who want to treat diseases by either adding new genes to the genome or disabling faulty ones. If you want to get a gene into a specific type of cell, a virion that recognises something about such cells may often prove a good tool.
The vaccine used to contain the Ebola outbreak in the Democratic Republic of Congo over the past two years was made by engineering Indiana vesiculovirus, which infects humans but cannot reproduce in them, so that it expresses a protein found on the surface of the Ebola virus; thus primed, the immune system responds to Ebola much more effectively. The World Health Organisation’s current list of 29 covid-19 vaccines in clinical trials features six versions of other viruses engineered to look a bit like SARS-CoV-2. One is based on a strain of measles that has long been used as a vaccine against that disease.
Viruses engineered to engender immunity against pathogens, to kill cancer cells or to encourage the immune system to attack them, or to deliver needed genes to faulty cells all seem likely to find their way into health care. Other engineered viruses are more worrying. One way to understand how viruses spread and kill is to try and make particularly virulent ones. In 2005, for example, Terrence Tumpey of America’s Centres for Disease Control and Prevention and his colleagues tried to understand the deadliness of the influenza virus responsible for the pandemic of 1918-20 by taking a more benign strain, adding what seemed to be distinctive about the deadlier one and trying out the result on mice. It was every bit as deadly as the original, wholly natural version had been.
The use of engineered pathogens as weapons of war is of dubious utility, completely illegal and repugnant to almost all
Because such “gain of function” research could, if ill-conceived or poorly implemented, do terrible damage, it requires careful monitoring. And although the use of engineered pathogens as weapons of war is of dubious utility—such weapons are hard to aim and hard to stand down, and it is not easy to know how much damage they have done—as well as being completely illegal and repugnant to almost all, such possibilities will and should remain a matter of global concern.
Information which, for billions of years, has only ever come into its own within infected cells can now be inspected on computer screens and rewritten at will. The power that brings is sobering. It marks a change in the history of both viruses and people—a change which is perhaps as important as any of those made by modern biology. It is constraining a small part of the viral world in a way which, so far, has been to people’s benefit. It is revealing that world’s further reaches in a way which cannot but engender awe. ■
Editor’s note: Some of our covid-19 coverage is free for readers of The Economist Today, our daily newsletter. For more stories and our pandemic tracker, see our hub
This article appeared in the Essay section of the print edition under the headline “The outsiders inside”
HUMANS THINK of themselves as the world’s apex predators. Hence the silence of sabre-tooth tigers, the absence of moas from New Zealand and the long list of endangered megafauna. But SARS–CoV-2 shows how people can also end up as prey. Viruses have caused a litany of modern pandemics, from covid-19, to HIV/AIDS to the influenza outbreak in 1918-20, which killed many more people than the first world war. Before that, the colonisation of the Americas by Europeans was abetted—and perhaps made possible—by epidemics of smallpox, measles and influenza brought unwittingly by the invaders, which annihilated many of the original inhabitants.
The influence of viruses on life on Earth, though, goes far beyond the past and present tragedies of a single species, however pressing they seem. Though the study of viruses began as an investigation into what appeared to be a strange subset of pathogens, recent research puts them at the heart of an explanation of the strategies of genes, both selfish and otherwise.
Viruses are unimaginably varied and ubiquitous. And it is becoming clear just how much they have shaped the evolution of all organisms since the very beginnings of life. In this, they demonstrate the blind, pitiless power of natural selection at its most dramatic. And—for one group of brainy bipedal mammals that viruses helped create—they also present a heady mix of threat and opportunity.
As our essay in this week’s issue explains, viruses are best thought of as packages of genetic material that exploit another organism’s metabolism in order to reproduce. They are parasites of the purest kind: they borrow everything from the host except the genetic code that makes them what they are. They strip down life itself to the bare essentials of information and its replication. If the abundance of viruses is anything to go by, that is a very successful strategy indeed.
The world is teeming with them. One analysis of seawater found 200,000 different viral species, and it was not setting out to be comprehensive. Other research suggests that a single litre of seawater may contain more than 100bn virus particles, and a kilo of dried soil ten times that number. Altogether, according to calculations on the back of a very big envelope, the world might contain 1031 of the things—that is one followed by 31 zeros, far outnumbering all other forms of life on the planet.
As far as anyone can tell, viruses—often of many different sorts—have adapted to attack every organism that exists. One reason they are powerhouses of evolution is that they oversee a relentless and prodigious slaughter, mutating as they do so. This is particularly clear in the oceans, where a fifth of single-celled plankton are killed by viruses every day. Ecologically, this promotes diversity by scything down abundant species, thus making room for rarer ones. The more common an organism, the more likely it is that a local plague of viruses specialised to attack it will develop, and so keep it in check.
This propensity to cause plagues is also a powerful evolutionary stimulus for prey to develop defences, and these defences sometimes have wider consequences. For example, one explanation for why a cell may deliberately destroy itself is if its sacrifice lowers the viral load on closely related cells nearby. That way, its genes, copied in neighbouring cells, are more likely to survive. It so happens that such altruistic suicide is a prerequisite for cells to come together and form complex organisms, such as pea plants, mushrooms and human beings.
The other reason viruses are engines of evolution is that they are transport mechanisms for genetic information. Some viral genomes end up integrated into the cells of their hosts, where they can be passed down to those organisms’ descendants. Between 8% and 25% of the human genome seems to have such viral origins. But the viruses themselves can in turn be hijacked, and their genes turned to new uses. For example, the ability of mammals to bear live young is a consequence of a viral gene being modified to permit the formation of placentas. And even human brains may owe their development in part to the movement within them of virus-like elements that create genetic differences between neurons within a single organism.
Evolution’s most enthralling insight is that breathtaking complexity can emerge from the sustained, implacable and nihilistic competition within and between organisms. The fact that the blind watchmaker has equipped you with the capacity to read and understand these words is in part a response to the actions of swarms of tiny, attacking replicators that have been going on, probably, since life first emerged on Earth around 4bn years ago. It is a startling example of that principle in action—and viruses have not finished yet.
Humanity’s unique, virus-chiselled consciousness opens up new avenues to deal with the viral threat and to exploit it. This starts with the miracle of vaccination, which defends against a pathogenic attack before it is launched. Thanks to vaccines, smallpox is no more, having taken some 300m lives in the 20th century. Polio will one day surely follow. New research prompted by the covid-19 pandemic will enhance the power to examine the viral realm and the best responses to it that bodies can muster—taking the defence against viruses to a new level.
Another avenue for progress lies in the tools for manipulating organisms that will come from an understanding of viruses and the defences against them. Early versions of genetic engineering relied on restriction enzymes—molecular scissors with which bacteria cut up viral genes and which biotechnologists employ to move genes around. The latest iteration of biotechnology, gene editing letter by letter, which is known as CRISPR, makes use of a more precise antiviral mechanism.
From the smallest beginnings
The natural world is not kind. A virus-free existence is an impossibility so deeply unachievable that its desirability is meaningless. In any case, the marvellous diversity of life rests on viruses which, as much as they are a source of death, are also a source of richness and of change. Marvellous, too, is the prospect of a world where viruses become a source of new understanding for humans—and kill fewer of them than ever before. ■
Correction: An earlier version of this article got its maths wrong. 1031 is one followed by 31 zeroes, not ten followed by 31 zeroes as we first wrote. Sorry.
Here’s the most depressing map you’re likely to see this week, courtesy of Anthony Fauci, head of the U.S. National Institute of Allergy and Infectious Diseases. The map, packaged in a recent paper co-written by Fauci, showcases the many other emerging diseases besides covid-19 that pose a threat to our health.
The paper, released over the weekend as a preprint in the journal Cell (meaning it may be revised before its final publication), is intended to lay out the environmental and human factors that led to covid-19 erupting on the world stage in late 2019. Fauci’s co-author is David Morens, senior scientific advisor at Office of the Director at NIAID. It’s an educational read, delving into how newly emerging diseases like covid-19 and familiar enemies like influenza can become so dangerous to humankind.
A map showing newly emerging and reemerging infectious diseases that have recently or could someday pose a serious threat to people’s health. The dots indicate where they were discovered or are most relevant currently. Image: Anthony Fauci, David Morens/Cell
Viruses like the flu, for instance, quickly mutate into new strains that can easily swap genes with other flu viruses and pick up just the right assortment of genetic tricks that make them more lethal than the seasonal flu and help them spread widely from person to person. Coronaviruses aren’t quite so erratic, but their ability to infect a wide variety of host species makes them more likely to spill over into people—and that’s the leading theory behind how covid-19 entered the picture.
In fact, it’s more than possible, Fauci and Morens note, that the common cold coronaviruses we have today once caused major and deadly epidemics in the past. Though that could provide some comfort, seeing as these viruses are now relatively harmless, not all dangerous viruses become more tame over time, and those that do often take a long time to mellow out.
That brings us to the aforementioned map, an exhaustive but by no means complete illustration of the emerging and reemerging diseases that have recently caused us trouble or are still plaguing us (the danger of weaponized anthrax is highlighted as a “deliberately emerging” disease). Many of these aren’t particularly likely to become a pandemic, at least at the moment. Ebola, for instance, is highly fatal but remains relatively hard to transmit between people. Bacterial diseases like gonorrhea are worrisome because they’re becoming resistant to antibiotics, but they’re not especially lethal.
Far from being a vanishingly rare event, though, humankind has experienced a pandemic on average every 20 years in the last hundred years, with the last, the H1N1 flu, showing up 10 years ago.
None of this is to say that we’re powerless against the coming germ tide—there’s much we can do to prepare, and in fact, many people predicted something like covid-19 happening as recently as last October. But without learning from our mistakes this time around, there’s no telling just how bad the next pandemic will be.
“Science will surely bring us many life-saving drugs, vaccines, and diagnostics; however, there is no reason to think that these alone can overcome the threat of ever more frequent and deadly emergencies of infectious diseases,” Fauci and Morens wrote. “Covid-19 is among the most vivid wake-up calls in over a century. It should force us to begin to think in earnest and collectively about living in more thoughtful and creative harmony with nature, even as we plan for nature’s inevitable, and always unexpected, surprises.”
Por Aluizio Marino², Danielle Klintowitz³, Gisele Brito², Raquel Rolnik¹, Paula Santoro¹, Pedro Mendonça²
Foto: Roberto Moreyra (Agência O Globo)
Desde o início da pandemia no Brasil muito tem se debatido acerca dos impactos nos diferentes territórios e segmentos sociais. Algo fundamental tanto para encontrar os melhores meios de prevenir a difusão da doença como de proteger aqueles que estão mais vulneráveis. Entretanto, a forma como as informações e os dados têm sido divulgados não auxilia na análise dos impactos territoriais e da difusão espacial da pandemia, dificultando também o seu devido enfrentamento.
Na cidade de São Paulo, a escala de análise da pandemia ainda são os distritos, que correspondem a porções enormes do território e com população maior do que muitas cidades de porte médio. Essa visão simplificadora ignora as heterogeneidades e desigualdades territoriais existentes na cidade. Conforme apontamos anteriormente, infelizmente a dimensão territorial não é considerada de forma adequada, prevalecendo uma leitura simplificada e, até mesmo, estigmatizada, como por exemplo quando se afirma “onde tem favela tem pandemia”.
Em artigo anterior, apresentamos o resultado de pesquisa em outra escala, a da rua. Para tanto, mapeamos as hospitalizações e óbitos pós internação por Covid-19 a partir do CEP – informação fornecida nas fichas dos pacientes hospitalizados com Síndrome Respiratória Aguda e Grave (SRAG) incluindo Covid-19 e disponibilizadas pelo DATASUS até aquele momento (18 de maio de 2020). Esse procedimento permitiu olhar mais detalhadamente para a distribuição territorial da pandemia, e assim evidenciar a complexidade de questões que explicam a sua difusão espacial, não apenas a precariedade habitacional e a presença de favelas.
A partir desta constatação passamos a investigar outros possíveis elementos explicativos, entre eles, a mobilidade urbana durante o período da pandemia, especificamente compreendendo o fluxo de circulação das pessoas na cidade e como isso influencia na difusão espacial da Covid-19. Com base nos dados disponibilizados pela SPTrans sobre dados de GPS dos ônibus, e a partir do roteamento de viagens selecionadas da Pesquisa Origem Destino de 2017, buscamos identificar de onde saíram e para onde foram as pessoas que circularam de transporte coletivo no dia 5 de junho, dia em que, segundo a SPTrans, cerca de 3 milhões de viagens foram realizadas usando os ônibus municipais. Ao mesmo tempo, fizemos uma leitura territorial sobre a origem das viagens durante o período de pandemia. Para esta análise identificou-se na Pesquisa Origem Destino (2017) as pessoas que usam transporte público como modo principal para chegar ao seu destino, motivadas pela ida ao local de trabalho. Consideramos apenas as viagens realizadas por pessoas sem ensino superior e em cargos não executivos. Esse perfil foi selecionado considerando que pessoas com ensino superior, em cargos executivos e profissionais liberais tenham aderido ao teletrabalho e que viagens com outras motivações, como educação e compras, pararam de ocorrer. Esses dados de mobilidade foram correlacionados com os dados de hospitalizações por SRAG não identificada, e Covid-19, até o dia 18 de maio, última data para qual o dado do CEP no DATASUS estava disponibilizado pelo Ministério da Saúde.
Desta forma produzimos um mapa que ilustra a distribuição dos lugares de origem das viagens diárias, a partir de uma distribuição que considera número de viagens nas zonas origem-destino e distribuição populacional dentro dessas zonas. O resultado mostra uma forte associação entre os locais que mais concentraram as origens das viagens com as manchas de concentração do local de residência de pessoas hospitalizadas com Covid-19 e Síndrome Respiratória Grave (SRAG) sem identificação, possivelmente casos de Covid-19, mas que não foram testados ou não tiveram resultado confirmado.
Mapa: Pedro Mendonça/ LabCidade
Com base neste estudo, pode-se dizer que, em síntese, quem está sendo mais atingido pela Covid-19 são as pessoas que tiveram que sair para trabalhar. Embora tenhamos mapeado os locais que concentram os maiores números de origens ou destinos dos fluxos de circulação por transporte coletivo, não é possível ainda afirmar se o contágio ocorreu no percurso do transporte, no local de trabalho ou no local de moradia, o que vai exigir análises futuras, que serão realizadas no âmbito desta pesquisa. Mas o que está evidente é que quem saiu para trabalhar e realizou percursos longos de transporte coletivo é que quem foi mais impactado pelos óbitos ocorridos. Enquanto esse fator mostrou associação forte com os casos de hospitalizações por SRAG não identificada e Covid-19, a densidade demográfica — frequentemente associada a áreas favelizadas e bairros populares — apresentou associação fraca.
Ainda que preliminares, esses dados apontam para a incoerência e inconsequência da abertura planejada pelas prefeituras e governo do estado. A reabertura de comércios e restaurantes implica em aumentar significativamente o número de áreas de origens com mais densidades de viagens e maior circulação de pessoas no transporte público. Se o maior número de óbitos está nos territórios que tiveram mais pessoas saindo para trabalhar durante o período de isolamento, temos que pensar tanto em políticas que as protejam em seus percursos como ampliar o direito ao isolamento paras as pessoas que não estão envolvidas com serviços essenciais mais precisam trabalhar para garantir seu sustento, o que reforça a importância de políticas de garantia de renda e segurança alimentar, subsídios de aluguel e outras despesas, e ações articuladas a coletivos e organizações locais para a proteção dos que mais estão ameaçados durante a pandemia.
Embora esses dados sejam públicos, nos parece que estão sendo ignorados para a definição de estratégias de enfrentamento a pandemia. É urgente repensar a forma como a política de mobilidade na cidade tem sido pensada, já que foram cometidos equívocos tal como o mega rodízio para veículos individuais, que durou apenas alguns dias e provocou uma superlotação nos transportes públicos ampliando os riscos das pessoas que precisavam sair para trabalhar. Ainda não foram implementadas medidas que garantam condições seguras para que as pessoas dos serviços essenciais pudessem fazer as viagens necessárias para exercer seus trabalhos sem ampliar a difusão da infecção do coronavírus. Bem como não existe uma leitura sobre a mobilidade metropolitana — inclusive não existem dados abertos sobre isso — ignorando as dinâmicas pendulares de pessoas que moram e trabalham em municípios diferentes da região metropolitana.
¹ Coordenadoras do LabCidade e professoras da Faculdade de Arquitetura e Urbanismo (FAU) da USP ² Pesquisadores do LabCidade ³ Pesquisadora do Instituto Pólis
Death Table from Tuberculosis in the United States, prepared for the International Congress on Tuberculosis, September 21 to October 12, 1908. Image: U.S. National Library of Medicine
Contrary to hopes for a tidy conclusion to the COVID-19 pandemic, history shows that outbreaks of infectious disease often have much murkier outcomes—including simply being forgotten about, or dismissed as someone else’s problem.
Recent history tells us a lot about how epidemics unfold, how outbreaks spread, and how they are controlled. We also know a good deal about beginnings—those first cases of pneumonia in Guangdong marking the SARS outbreak of 2002–3, the earliest instances of influenza in Veracruz leading to the H1N1 influenza pandemic of 2009–10, the outbreak of hemorrhagic fever in Guinea sparking the Ebola pandemic of 2014–16. But these stories of rising action and a dramatic denouement only get us so far in coming to terms with the global crisis of COVID-19. The coronavirus pandemic has blown past many efforts at containment, snapped the reins of case detection and surveillance across the world, and saturated all inhabited continents. To understand possible endings for this epidemic, we must look elsewhere than the neat pattern of beginning and end—and reconsider what we mean by the talk of “ending” epidemics to begin with.
The social lives of epidemics show them to be not just natural phenomena but also narrative ones: deeply shaped by the stories we tell about their beginnings, their middles, their ends.
Historians have long been fascinated by epidemics in part because, even where they differ in details, they exhibit a typical pattern of social choreography recognizable across vast reaches of time and space. Even though the biological agents of the sixth-century Plague of Justinian, the fourteenth-century Black Death, and the early twentieth-century Manchurian Plague were almost certainly not identical, the epidemics themselves share common features that link historical actors to present experience. “As a social phenomenon,” the historian Charles Rosenberg has argued, “an epidemic has a dramaturgic form. Epidemics start at a moment in time, proceed on a stage limited in space and duration, following a plot line of increasing and revelatory tension, move to a crisis of individual and collective character, then drift towards closure.” And yet not all diseases fit so neatly into this typological structure. Rosenberg wrote these words in 1992, nearly a decade into the North American HIV/AIDS epidemic. His words rang true about the origins of that disease—thanks in part to the relentless, overzealous pursuit of its “Patient Zero”—but not so much about its end, which was, as for COVID-19, nowhere in sight.
In the case of the new coronavirus, we have now seen an initial fixation on origins give way to the question of endings. In March The Atlantic offered four possible “timelines for life returning to normal,” all of which depended the biological basis of a sufficient amount of the population developing immunity (perhaps 60 to 80 percent) to curb further spread. This confident assertion derived from models of infectious outbreaks formalized by epidemiologists such as W. H. Frost a century earlier. If the world can be defined into those susceptible (S), infected (I) and resistant (R) to a disease, and a pathogen has a reproductive number R0 (pronounced R-naught) describing how many susceptible people can be infected by a single infected person, the end of the epidemic begins when the proportion of susceptible people drops below the reciprocal, 1/R0. When that happens, one person would infect, on average, less than one other person with the disease.
These formulas reassure us, perhaps deceptively. They conjure up a set of natural laws that give order to the cadence of calamities. The curves produced by models, which in better times belonged to the arcana of epidemiologists, are now common figures in the lives of billions of people learning to live with contractions of civil society promoted in the name of “bending,” “flattening,” or “squashing” them. At the same time, as David Jones and Stefan Helmreich recently wrote in these pages, the smooth lines of these curves are far removed from jagged realities of the day-to-day experience of an epidemic—including the sharp spikes in those “reopening” states where modelers had predicted continued decline.
In other words, epidemics are not merely biological phenomena. They are inevitably framed and shaped by our social responses to them, from beginning to end (whatever that may mean in any particular case). The questions now being asked of scientists, clinicians, mayors, governors, prime ministers, and presidents around the world is not merely “When will the biological phenomenon of this epidemic resolve?” but rather “When, if ever, will the disruption to our social life caused in the name of coronavirus come to an end?” As peak incidence nears, and in many places appears to have passed, elected officials and think tanks from opposite ends of the political spectrum provide “roadmaps” and “frameworks” for how an epidemic that has shut down economic, civic, and social life in a manner not seen globally in at least a century might eventually recede and allow resumption of a “new normal.”
To understand possible endings for this epidemic, we must look elsewhere than the neat pattern of beginning and end—and reconsider what we mean by the talk of “ending” epidemics to begin with.
These two faces of an epidemic, the biological and the social, are closely intertwined, but they are not the same. The biological epidemic can shut down daily life by sickening and killing people, but the social epidemic also shuts down daily life by overturning basic premises of sociality, economics, governance, discourse, interaction—and killing people in the process as well. There is a risk, as we know from both the Spanish influenza of 1918–19 and the more recent swine flu of 2008–9, of relaxing social responses before the biological threat has passed. But there is also a risk in misjudging a biological threat based on faulty models or bad data and in disrupting social life in such a way that the restrictions can never properly be taken back. We have seen in the case of coronavirus the two faces of the epidemic escalating on local, national, and global levels in tandem, but the biological epidemic and the social epidemic don’t necessarily recede on the same timeline.
For these sorts of reasons we must step back and reflect in detail on what we mean by ending in the first place. The history of epidemic endings has taken many forms, and only a handful of them have resulted in the elimination of a disease.
History reminds us that the interconnections between the timing of the biological and social epidemics are far from obvious. In some cases, like the yellow fever epidemics of the eighteenth century and the cholera epidemics of the nineteenth century, the dramatic symptomatology of the disease itself can make its timing easy to track. Like a bag of popcorn popping in the microwave, the tempo of visible case-events begins slowly, escalates to a frenetic peak, and then recedes, leaving a diminishing frequency of new cases that eventually are spaced far enough apart to be contained and then eliminated. In other examples, however, like the polio epidemics of the twentieth century, the disease process itself is hidden, often mild in presentation, threatens to come back, and ends not on a single day but over different timescales and in different ways for different people.
Campaigns against infectious diseases are often discussed in military terms, and one result of that metaphor is to suggest that epidemics too must have a singular endpoint. We approach the infection peak as if it were a decisive battle like Waterloo, or a diplomatic arrangement like the Armistice at Compiègne in November 1918. Yet the chronology of a single, decisive ending is not always true even for military history, of course. Just as the clear ending of a military war does not necessarily bring a close to the experience of war in everyday life, so too the resolution of the biological epidemic does not immediately undo the effects of the social epidemic. The social and economic effects of the 1918–1919 pandemic, for example, were felt long after the end of the third and putatively final wave of the virus. While the immediate economic effect on many local businesses caused by shutdowns appears to have resolved in a matter of months, the broader economic effects of the epidemic on labor-wage relations were still visible in economic surveys in 1920, again in 1921, and in several areas as far as 1930.
The history of epidemic endings has taken many forms, and only a handful of them have resulted in the elimination of a disease.
And yet, like World War One with which its history was so closely intertwined, the influenza pandemic of 1918–19 appeared at first to have a singular ending. In individual cities the epidemic often produced dramatic spikes and falls in equally rapid tempo. In Philadelphia, as John Barry notes in The Great Influenza (2004), after an explosive and deadly rise in October 1919 that peaked at 4,597 deaths in a single week, cases suddenly dropped so precipitously that the public gathering ban could be lifted before the month was over, with almost no new cases in following weeks. A phenomenon whose destructive potential was limited by material laws, “the virus burned through available fuel, then it quickly faded away.”
As Barry reminds us, however, scholars have since learned to differentiate at least three different sequences of epidemics within the broader pandemic. The first wave blazed through military installations in the spring of 1918, the second wave caused the devastating mortality spikes in the summer and fall of 1918, and the third wave began in December 1918 and lingered long through the summer of 1919. Some cities, like San Francisco, passed through the first and second waves relatively unscathed only to be devastated by the third wave. Nor was it clear to those still alive in 1919 that the pandemic was over after the third wave receded. Even as late as 1922, a bad flu season in Washington State merited a response from public health officials to enforce absolute quarantine as they had during 1918–19. It is difficult, looking back, to say exactly when this prototypical pandemic of the twentieth century was really over.
Who can tell when a pandemic has ended? Today, strictly speaking, only the World Health Organization (WHO). The Emergency Committee of the WHO is responsible for the global governance of health and international coordination of epidemic response. After the SARS coronavirus pandemic of 2002–3, this body was granted sole power to declare the beginnings and endings of Public Health Emergencies of International Concern (PHEIC). While SARS morbidity and mortality—roughly 8,000 cases and 800 deaths in 26 countries—has been dwarfed by the sheer scale of COVID-19, the pandemic’s effect on national and global economies prompted revisions to the International Health Regulations in 2005, a body of international law that had remained unchanged since 1969. This revision broadened the scope of coordinated global response from a handful of diseases to any public health event that the WHO deemed to be of international concern and shifted from a reactive response framework to a pro-active one based on real-time surveillance and detection and containment at the source rather than merely action at international borders.
This social infrastructure has important consequences, not all of them necessarily positive. Any time the WHO declares a public health event of international concern—and frequently when it chooses not to declare one—the event becomes a matter of front-page news. Since the 2005 revision, the group has been criticized both for declaring a PHEIC too hastily (as in the case of H1N1) or too late (in the case of Ebola). The WHO’s decision to declare the end of a PHEIC, by contrast, is rarely subject to the same public scrutiny. When an outbreak is no longer classified as an “extraordinary event” and no longer is seen to pose a risk at international spread, the PHEIC is considered not to be justified, leading to a withdrawal of international coordination. Once countries can grapple with the disease within their own borders, under their own national frameworks, the PHEIC is quietly de-escalated.
At their worst, epidemic endings are a form of collective amnesia, transmuting the disease that remains into merely someone else’s problem.
As the response to the 2014–16 Ebola outbreak in West Africa demonstrates, however, the act of declaring the end of a pandemic can be just as powerful as the act of declaring its beginning—in part because emergency situations can continue even after a return to “normal” has been declared. When WHO Director General Margaret Chan announced in March 2016 that the Ebola outbreak was no longer a public health event of international concern, international donors withdrew funds and care to the West African countries devastated by the outbreak, even as these struggling health systems continued to be stretched beyond their means by the needs of Ebola survivors. NGOs and virologists expressed concern that efforts to fund Ebola vaccine development would likewise fade without a sense of global urgency pushing research forward.
Part of the reason that the role of the WHO in proclaiming and terminating the state of pandemic is subject to so much scrutiny is that it can be. The WHO is the only global health body that is accountable to all governments of the world; its parliamentary World Health Assembly contains health ministers from every nation. Its authority rests not so much on its battered budget as its access to epidemic intelligence and pool of select individuals, technical experts with vast experience in epidemic response. But even though internationally sourced scientific and public health authority is key to its role in pandemic crises, WHO guidance is ultimately carried out in very different ways and on very different time scales in different countries, provinces, states, counties, and cities. One state might begin to ease up restrictions to movement and industry just as another implements more and more stringent measures. If each country’s experience of “lockdown” has already been heterogeneous, the reconnection between them after the PHEIC is ended will likely show even more variance.
So many of our hopes for the termination of the present PHEIC now lie in the promise of a COVID-19 vaccine. Yet a closer look at one of the central vaccine success stories of the twentieth century shows that technological solutions rarely offer resolution to pandemics on their own. Contrary to our expectations, vaccines are not universal technologies. They are always deployed locally, with variable resources and commitments to scientific expertise. International variations in research, development, and dissemination of effective vaccines are especially relevant in the global fight against epidemic polio.
The development of the polio vaccine is relatively well known, usually told as a story of an American tragedy and triumph. Yet while polio epidemics that swept the globe in the postwar decades did not respect national borders or the Iron Curtain, the Cold War provided context for both collaboration and antagonism. Only a few years after the licensing of Jonas Salk’s inactivated vaccine in the United States, his technique became widely used across the world, although its efficacy outside of the United States was questioned. The second, live oral vaccine developed by Albert Sabin, however, involved extensive collaboration in with Eastern European and Soviet colleagues. As the success of the Soviet polio vaccine trials marked a rare landmark of Cold War cooperation, Basil O’Connor, president of the March of Dimes movement, speaking at the Fifth International Poliomyelitis Conference in 1960, proclaimed that “in search for the truth that frees man from disease, there is no cold war.”
Two faces of an epidemic, the biological and the social, are closely intertwined, but they are not the same.
Yet the differential uptake of this vaccine retraced the divisions of Cold War geography. The Soviet Union, Hungary, and Czechoslovakia were the first countries in the world to begin nationwide immunization with the Sabin vaccine, soon followed by Cuba, the first country in the Western Hemisphere to eliminate the disease. By the time the Sabin vaccine was licensed in the United States in 1963, much of Eastern Europe had done away with epidemics and was largely polio-free. The successful ending of this epidemic within the communist world was immediately held up as proof of the superiority of their political system.
Western experts who trusted the Soviet vaccine trials, including the Yale virologist and WHO envoy Dorothy Horstmann, nonetheless emphasized that their results were possible because of the military-like organization of the Soviet health care system. Yet these enduring concerns that authoritarianism itself was the key tool for ending epidemics—a concern reflected in current debates over China’s heavy-handed interventions in Wuhan this year—can also be overstated. The Cold War East was united not only by authoritarianism and heavy hierarchies in state organization and society, but also by a powerful shared belief in the integration of paternal state, biomedical research, and socialized medicine. Epidemic management in these countries combined an emphasis on prevention, easily mobilized health workers, top-down organization of vaccinations, and a rhetoric of solidarity, all resting on a health care system that aimed at access to all citizens.
Still, authoritarianism as a catalyst for controlling epidemics can be singled out and pursued with long-lasting consequences. Epidemics can be harbingers of significant political changes that go well beyond their ending, significantly reshaping a new “normal” after the threat passes. Many Hungarians, for example, have watched with alarm the complete sidelining of parliament and the introduction of government by decree at the end of March this year. The end of any epidemic crisis, and thus the end of the need for the significantly increased power of Viktor Orbán, would be determined by Orbán himself. Likewise, many other states, urging the mobilization of new technologies as a solution to end epidemics, are opening the door to heightened state surveillance of their citizens. The apps and trackers now being designed to follow the movement and exposure of people in order to enable the end of epidemic lockdowns can collect data and establish mechanisms that reach well beyond the original intent. The digital afterlives of these practices raise new and unprecedented questions about when and how epidemics end.
Like infectious agents on an agar plate, epidemics colonize our social lives and force us to learn to live with them, in some way or another, for the foreseeable future.
Although we want to believe that a single technological breakthrough will end the present crisis, the application of any global health technology is always locally determined. After its dramatic successes in managing polio epidemics in the late 1950s and early 1960s, the oral poliovirus vaccine became the tool of choice for the Global Polio Eradication Initiative in the late 1980s, as it promised an end to “summer fears” globally. But since vaccines are in part technologies of trust, ending polio outbreaks depends on maintaining confidence in national and international structures through which vaccines are delivered. Wherever that often fragile trust is fractured or undermined, vaccination rates can drop to a critical level, giving way to vaccine-derived polio, which thrives in partially vaccinated populations.
In Kano, Nigeria, for example, a ban on polio vaccination between 2000 and 2004 resulted in a new national polio epidemic that soon spread to neighboring countries. As late as December 2019 polio outbreaks were still reported in fifteen African countries, including Angola and the Democratic Republic of the Congo. Nor is it clear that polio can fully be regarded as an epidemic at this point: while polio epidemics are now a thing of the past for Hungary—and the rest of Europe, the Americas, Australia, and East Asia as well—the disease is still endemic to parts of Africa and South Asia. A disease once universally epidemic is now locally endemic: this, too, is another way that epidemics end.
Indeed, many epidemics have only “ended” through widespread acceptance of a newly endemic state. Consider the global threat of HIV/AIDS. From a strictly biological perspective, the AIDS epidemic has never ended; the virus continues to spread devastation through the world, infecting 1.7 million people and claiming an estimated 770,000 lives in the year 2018 alone. But HIV is not generally described these days with the same urgency and fear that accompanied the newly defined AIDS epidemic in the early 1980s. Like coronavirus today, AIDS at that time was a rapidly spreading and unknown emerging threat, splayed across newspaper headlines and magazine covers, claiming the lives of celebrities and ordinary citizens alike. Nearly forty years later it has largely become a chronic disease endemic, at least in the Global North. Like diabetes, which claimed an estimated 4.9 million lives in 2019, HIV/AIDS became a manageable condition—if one had access to the right medications.
Those who are no longer directly threatened by the impact of the disease have a hard time continuing to attend to the urgency of an epidemic that has been rolling on for nearly four decades. Even in the first decade of the AIDS epidemic, activists in the United States fought tooth and nail to make their suffering visible in the face of both the Reagan administration’s dogged refusal to talk publicly about the AIDS crisis and the indifference of the press after the initial sensation of the newly discovered virus had become common knowledge. In this respect, the social epidemic does not necessarily end when biological transmission has ended, or even peaked, but rather when, in the attention of the general public and in the judgment of certain media and political elites who shape that attention, the disease ceases to be newsworthy.
Though we like to think of science as universal and objective, crossing borders and transcending differences, it is in fact deeply contingent upon local practices.
Polio, for its part, has not been newsworthy for a while, even as thousands around the world still live with polio with ever-decreasing access to care and support. Soon after the immediate threat of outbreaks passed, so did support for those whose lives were still bound up with the disease. For others, it became simply a background fact of life—something that happens elsewhere. The polio problem was “solved,” specialized hospitals were closed, fundraising organizations found new causes, and poster children found themselves in an increasingly challenging world. Few medical professionals are trained today in the treatment of the disease. As intimate knowledge of polio and its treatment withered away with time, people living with polio became embodied repositories of lost knowledge.
History tells us public attention is much more easily drawn to new diseases as they emerge rather than sustained over the long haul. Well before AIDS shocked the world into recognizing the devastating potential of novel epidemic diseases, a series of earlier outbreaks had already signaled the presence of emerging infectious agents. When hundreds of members of the American Legion fell ill after their annual meeting in Philadelphia in 1976, the efforts of epidemiologists from the Centers for Disease Control to explain the spread of this mysterious disease and its newly discovered bacterial agent, Legionella, occupied front-page headlines. In the years since, however, as the 1976 incident faded from memory, Legionella infections have become everyday objects of medical care, even though incidence in the U.S. has grown ninefold since 2000, tracing a line of exponential growth that looks a lot like COVID-19’s on a longer time scale. Yet few among us pause in our daily lives to consider whether we are living through the slowly ascending limb of a Legionella epidemic.
Nor do most people living in the United States stop to consider the ravages of tuberculosis as a pandemic, even though an estimated 10 million new cases of tuberculosis were reported around the globe in 2018, and an estimated 1.5 million people died from the disease. The disease seems to only receive attention in relation to newer scourges: in the late twentieth century TB coinfection became a leading cause of death in emerging HIV/AIDS pandemic, while in the past few months TB coinfection has been invoked as a rising cause of mortality in COVID-19 pandemic. Amidst these stories it is easy to miss that on its own, tuberculosis has been and continues to be the leading cause of death worldwide from a single infectious agent. And even though tuberculosis is not an active concern of middle-class Americans, it is still not a thing of the past even in this country. More than 9,000 cases of tuberculosis were reported in the United States in 2018—overwhelmingly affecting racial and ethnic minority populations—but they rarely made the news.
There will be no simple return to the way things were: whatever normal we build will be a new one—whether many of us realize it or not.
While tuberculosis is the target of concerted international disease control efforts, and occasionally eradication efforts, the time course of this affliction has been spread out so long—and so clearly demarcated in space as a problem of “other places”—that it is no longer part of the epidemic imagination of the Global North. And yet history tells a very different story. DNA lineage studies of tuberculosis now show that the spread of tuberculosis in sub-Saharan Africa and Latin America was initiated by European contact and conquest from the fifteenth century through the nineteenth. In the early decades of the twentieth century, tuberculosis epidemics accelerated throughout sub-Saharan Africa, South Asia, and Southeast Asia due to the rapid urbanization and industrialization of European colonies. Although the wave of decolonizations that swept these regions between the 1940s and the 1980s established autonomy and sovereignty for newly post-colonial nations, this movement did not send tuberculosis back to Europe.
These features of the social lives of epidemics—how they live on even when they seem, to some, to have disappeared—show them to be not just natural phenomena but also narrative ones: deeply shaped by the stories we tell about their beginnings, their middles, their ends. At their best, epidemic endings are a form of relief for the mainstream “we” that can pick up the pieces and reconstitute a normal life. At their worst, epidemic endings are a form of collective amnesia, transmuting the disease that remains into merely someone else’s problem.
What are we to conclude from these complex interactions between the social and the biological faces of epidemics, past and present? Like infectious agents on an agar plate, epidemics colonize our social lives and force us to learn to live with them, in some way or another, for the foreseeable future. Just as the postcolonial period continued to be shaped by structures established under colonial rule, so too are our post-pandemic futures indelibly shaped by what we do now. There will be no simple return to the way things were: whatever normal we build will be a new one—whether many of us realize it or not. Like the world of scientific facts after the end of a critical experiment, the world that we find after an the end of an epidemic crisis—whatever we take that to be—looks in many ways like the world that came before, but with new social truths established. How exactly these norms come into being depends a great deal on particular circumstances: current interactions among people, the instruments of social policy as well as medical and public health intervention with which we apply our efforts, and the underlying response of the material which we applied that apparatus against (in this case, the coronavirus strain SARS-CoV-2). While we cannot know now how the present epidemic will end, we can be confident that it in its wake it will leave different conceptions of normal in realms biological and social, national and international, economic and political.
Though we like to think of science as universal and objective, crossing borders and transcending differences, it is in fact deeply contingent upon local practices—including norms that are easily thrown over in an emergency, and established conventions that do not always hold up in situations of urgency. Today we see civic leaders jumping the gun in speaking of access to treatments, antibody screens, and vaccines well in advance of any scientific evidence, while relatively straightforward attempts to estimate the true number of people affected by the disease spark firestorms over the credibility of medical knowledge. Arduous work is often required to achieve scientific consensus, and when the stakes are high—especially when huge numbers of lives are at risk—heterogeneous data give way to highly variable interpretations. As data moves too quickly in some domains and too slowly in others, and sped-up time pressures are placed on all investigations the projected curve of the epidemic is transformed into an elaborate guessing game, in which different states rely on different kinds of scientific claims to sketch out wildly different timetables for ending social restrictions.
The falling action of an epidemic is perhaps best thought of as asymptotic: never disappearing, but rather fading to the point where signal is lost in the noise of the new normal—and even allowed to be forgotten.
These varied endings of the epidemic across local and national settings will only be valid insofar as they are acknowledged as such by others—especially if any reopening of trade and travel is to be achieved. In this sense, the process of establishing a new normal in global commerce will continue to be bound up in practices of international consensus. What the new normal in global health governance will look like, however, is more uncertain than ever. Long accustomed to the role of international scapegoat, the WHO Secretariat seems doomed to be accused either of working beyond its mandate or not acting fast enough. Moreover, it can easily become a target of scapegoating, as the secessionist posturing of Donald Trump demonstrates. Yet the U.S. president’s recent withdrawal from this international body is neither unprecedented nor unsurmountable. Although Trump’s voting base might not wish to be grouped together with the only other global power to secede from the WHO, after the Soviet Union’s 1949 departure from the group it ultimately brought all Eastern Bloc back to task of international health leadership in 1956. Much as the return of the Soviets to the WHO resulted in the global eradication of smallpox—the only human disease so far to have been intentionally eradicated—it is possible that some future return of the United States to the project of global health governance might also result in a more hopeful post-pandemic future.
As the historians at the University of Oslo have recently noted, in epidemic periods “the present moves faster, the past seems further removed, and the future seems completely unpredictable.” How, then, are we to know when epidemics end? How does the act of looking back aid us in determining a way forward? Historians make poor futurologists, but we spend a lot of time thinking about time. And epidemics produce their own kinds of time, in both biological and social domains, disrupting our individual senses of passing days as well as conventions for collective behavior. They carry within them their own tempos and rhythms: the slow initial growth, the explosive upward limb of the outbreak, the slowing of transmission that marks the peak, plateau, and the downward limb. This falling action is perhaps best thought of as asymptotic: rarely disappearing, but rather fading to the point where signal is lost in the noise of the new normal—and even allowed to be forgotten.
Students at a university in Germany evaluate data from COVID-19 patients [Reuters]
Have you heard the axiom “In war, truth is the first casualty?”
As healthcare providers around the world wage war against the COVID-19 pandemic, national governments have taken to brawling with researchers, the media and each other over the veracity of the data used to monitor and track the disease’s march across the globe.
Allegations of deliberate data tampering carry profound public health implications. If a country knowingly misleads the World Health Organization (WHO) about the emergence of an epidemic or conceals the severity of an outbreak within its borders, precious time is lost. Time that could be spent mobilising resources around the globe to contain the spread of the disease. Time to prepare health systems for a coming tsunami of infections. Time to save more lives.
No one country has claimed that their science or data is perfect: French and US authorities confirmed they had their first coronavirus cases weeks earlier than previously thought.
Still, coronavirus – and the data used to benchmark it – has become grist for the political mill. But if we tune out the voices of politicians and pundits, and listen to those of good governance experts, data scientists and epidemiological specialists, what does the most basic but consequential data – the number of confirmed cases per country – tell us about how various governments around the globe are crunching coronavirus numbers and spinning corona-narratives?
What the good governance advocates say
Similar to how meteorologists track storms, data scientists use models to express how epidemics progress, and to predict where the next hurricane of new infections will batter health systems.
This data is fed by researchers into computer modelling programmes that national authorities and the WHO use to advise countries and aid organisations on where to send medical professionals and equipment, and when to take actions such as issuing lockdown orders.
The WHO also harnesses this data to produce a daily report that news organisations use to provide context around policy decisions related to the pandemic. But, unlike a hurricane, which cannot be hidden, epidemic data can be fudged and manipulated.
“The WHO infection numbers are based on reporting from its member states. The WHO cannot verify these numbers,” said Michael Meyer-Resende, Democracy Reporting International’s executive director.
To date, more than 8 million people have been diagnosed as confirmed cases of COVID-19. Of that number, more than 443,000 have died from the virus, according to Johns Hopkins University.
Those numbers are commonly quoted, but what is often not explained is that they both ultimately hinge on two factors: how many people are being tested, and the accuracy of the tests being administered. These numbers we “fetishise”, said Meyer-Resende, “depend on testing, on honesty of governments and on size of the population”.
“Many authoritarian governments are not transparent with their data generally, and one should not expect that they are transparent in this case,” he said. To test Meyer-Resende’s theory that less government transparency equals less transparent COVID-19 case data, Al Jazeera used Transparency International’s Corruption Perceptions Index and the Economist Intelligence Unit’s Democracy Index as lenses through which to view the number of reported cases of the coronavirus.
The examination revealed striking differences in the number of confirmed COVID-19 cases that those nations deemed transparent and democratic reported compared to the numbers reported by nations perceived to be corrupt and authoritarian.
Denmark, with a population of roughly six million, is ranked in the top 10 of the most transparent and democratic countries. The country reported on May 1 that it had 9,158 confirmed cases of COVID-19, a ratio of 1,581 confirmed cases per million. That was more than triple the world average for that day – 412 cases per million people – according to available data.
Meanwhile, Turkmenistan, a regular in the basement of governance and corruption indexes, maintains that not one of its roughly six million citizens has been infected with COVID-19, even though it borders and has extensive trade with Iran, a regional epicentre of the pandemic.
Also on May 1, Myanmar, with a population of more than 56 million, reported just 151 confirmed cases of infection, a rate of 2.8 infections per million. That is despite the fact that every day, roughly 10,000 workers cross the border into China, where the pandemic first began.
On February 4, Myanmar suspended its air links with Chinese cities, including Wuhan, where COVID-19 is said to have originated last December (however, a recent study reported that the virus may have hit the city as early as August 2019).
“That just seems abnormal, out of the ordinary. Right?” said Roberto Kukutschka, Transparency International’s research coordinator, in reference to the numbers of reported cases.
“In these countries where you have high levels of corruption, there are high levels of discretion as well,” he told Al Jazeera. “It’s counter-intuitive that these countries are reporting so few cases, when all countries that are more open about these things are reporting way more. It’s very strange.”
While Myanmar has started taking steps to address the pandemic, critics say a month of preparation was lost to jingoistic denial. Ten days before the first two cases were confirmed, government spokesman Zaw Htay claimed the country was protected by its lifestyle and diet, and because cash is used instead of credit cards to make purchases.
Turkmenistan’s authorities have reportedly removed almost all mentions of the coronavirus from official publications, including a read-out of a March 27 phone call between Uzbek President Shavkat Mirziyoyev and Turkmen President Gurbanguly Berdimuhamedov.
It is unclear if Turkmenistan even has a testing regime.
Russia, on the other hand, touts the number of tests it claims to have performed, but not how many people have been tested – and that is a key distinction because the same person can be tested more than once. Transparency International places Russia in the bottom third of its corruption index.
On May 1, Russia, with a population just above 145 million, reported that it had confirmed 106,498 cases of COVID-19 after conducting an astounding 3.72 million “laboratory tests”. Just 2.9 percent of the tests produced a positive result.
Remember, Denmark’s population is six million, or half that of Moscow’s. Denmark had reportedly tested 206,576 people by May 1 and had 9,158 confirmed coronavirus cases, a rate of 4.4 percent. Finland, another democracy at the top of the transparency index, has a population of 5.5 million and a positive test result rate of 4.7 percent.
This discrepancy spurred the editors of PCR News, a Moscow-based Russian-language molecular diagnostics journal, to take a closer look at the Russian test. They reported that in order to achieve a positive COVID-19 result, the sample tested must contain a much higher volume of the virus, or viral load, as compared to the amount required for a positive influenza test result.
In terms of sensitivity or ability to detect COVID-19, the authors wrote: “Is it high or low? By modern standards – low.”
They later added, “The test will not reveal the onset of the disease, or it will be decided too early that the recovering patient no longer releases viruses and cannot infect anyone. And he walks along the street, and he is contagious.”
Ostensibly, if that person then dies, COVID-19 will not be certified as the cause of death.
Good governance experts see a dynamic at play.
Countries who test less will be shown as less of a problem. Countries that test badly will seem as if they don’t have a problem. Numbers are very powerful.
Michael Meyer-Resende, Democracy Reporting International
“In many of these countries, the legitimacy of the state depends on not going into crisis,” said Kukutschka, adding that he counts countries with world-class health systems among them.
“Countries who test less will be shown as less of a problem. Countries that test badly will seem as if they don’t have a problem,” said Meyer-Resende. “Numbers are very powerful. They seem objective.”
Meyer-Resende highlighted the case of China. “The Chinese government said for a while that it had zero new cases. That’s a very powerful statement. It says it all with a single digit: ‘We have solved the problem’. Except, it hadn’t. It had changed the way of counting cases.”
China – where the pandemic originated – recently escaped a joint US-Australian-led effort at the World Health Assembly to investigate whether Beijing had for weeks concealed a deadly epidemic from the WHO.
China alerted the WHO about the epidemic on December 31, 2019. Researchers at the University of Hong Kong estimated that the actual number of COVID-19 cases in China, where the coronavirus first appeared, could have been four times greater in the beginning of this year than what Chinese authorities had been reporting to the WHO.
“We estimated that by Feb 20, 2020, there would have been 232,000 confirmed cases in China as opposed to the 55,508 confirmed cases reported,” said the researchers’ report published by the Lancet.
The University of Hong Kong researchers attribute the discrepancy to ever-changing case definitions, the official guidance that tells doctors which symptoms – and therefore patients – can be diagnosed and recorded as COVID-19. China’s National Health Commission issued no less than seven versions of these guidelines between January 15 and March 3.
All of which adds to the confusion.
“Essentially, we are moving in a thick fog, and the numbers we have are no more than a small flashlight,” said Meyer-Resende.
What the epidemiological expert thinks
Dr Ghassan Aziz monitors epidemics in the Middle East. He is the Health Surveillance Program manager at the Doctors Without Borders (MSF) Middle East Unit. He spoke to Al Jazeera in his own capacity and not on behalf of the NGO.
“I think Iran, they’re not reporting everything,” he told Al Jazeera. “It’s fair to assume that [some countries] are underreporting because they are under-diagnosing. They report what they detect.”
“Maybe [it’s] on purpose, and maybe because of the sanctions and the lack of testing capacities,” said Aziz.
Once China shared the novel coronavirus genome on January 24, many governments began in earnest to test their populations. Others have placed limits on who can be tested.
In Brazil, due to a sustained lack of available tests, patients using the public health network in April were tested only if they were hospitalised with severe symptoms. On April 1, Brazil reported that 201 people had died from the virus. That number was challenged by doctors and relatives of the dead. A month later, after one minister of health was fired and another resigned after a week on the job, the testing protocols had not changed.
On May 1, Brazil reported that COVID-19 was the cause of death for 5,901 people. On June 5, Brazil’s health ministry took down the website that reported cumulative coronavirus numbers – only to be ordered by the country’s Supreme Court to reinstate the information.
Right-wing President Jair Bolsonaro has repeatedly played down the severity of the coronavirus pandemic, calling it “a little flu”. Brazilian Supreme Court Justice Gilmar Mendes accused the government of attempting to manipulate statistics, calling it “a manoeuvre of totalitarian regimes”.
Brazil currently has the dubious distinction of having the second-highest number of COVID-19 deaths in the world, behind the US. By June 15, the COVID-19 death toll in the country had surpassed 43,300 people.
Dr Aziz contends that even with testing, many countries customarily employ a “denial policy”. He said in his native country, Iraq, health authorities routinely obfuscate health emergencies by changing the names of outbreaks such as cholera to “endemic diarrhoea”, or Crimean-Congo hemorrhagic fever to “epidemic fever”.
“In Iraq, they give this idea to the people that ‘We did our best. We controlled it,'” Dr Aziz said. “When someone dies, ‘Oh. It’s not COVID-19. He was sick. He was old. This is God’s will. It was Allah.’ This is what I find so annoying.”
What the data scientist says
Sarah Callaghan, a data scientist and the editor-in-chief of Patterns, a data-science medical journal, told Al Jazeera the numbers of confirmed cases countries report reflect “the unique testing and environmental challenges that each country is facing”.
But, she cautioned: “Some countries have the resources and infrastructure to carry out widespread testing, others simply don’t. Some countries might have the money and the ability to test, but other local issues come into play, like politics.”
According to Callaghan, even in the best of times under the best circumstances, collecting data on an infectious disease is both difficult and expensive. But despite the difficulties presented by some countries’ data, she remains confident that the data and modelling that is available will indeed contribute much to understanding how COVID-19 spreads, how the virus reacts to different environmental conditions, and discovering the questions that need answers.
Her advice is: “When looking at the numbers, think about them. Ask yourself if you trust the source. Ask yourself if the source is trying to push a political or economic agenda.”
“There’s a lot about this situation that we don’t know, and a lot more misinformation that’s being spread, accidentally or deliberately.”
Many mass immunization efforts worldwide were halted this spring to prevent spread of the virus at crowded inoculation sites. The consequences have been alarming.
Three-year-old Allay Ngandema, who contracted measles, ate lunch with his mother, Maboa Alpha, in the measles isolation ward in Boso-Manzi hospital in the Democratic Republic of Congo in late February. Credit: Hereward Holland/Reuters.
As poor countries around the world struggle to beat back the coronavirus, they are unintentionally contributing to fresh explosions of illness and death from other diseases — ones that are readily prevented by vaccines.
This spring, after the World Health Organization and UNICEF warned that the pandemic could spread swiftly when children gathered for shots, many countries suspended their inoculation programs. Even in countries that tried to keep them going, cargo flights with vaccine supplies were halted by the pandemic and health workers diverted to fight it.
Now, diphtheria is appearing in Pakistan, Bangladesh and Nepal.
Cholera is in South Sudan, Cameroon, Mozambique, Yemen and Bangladesh.
A mutated strain of poliovirus has been reported in more than 30 countries.
And measles is flaring around the globe, including in Bangladesh, Brazil, Cambodia, Central African Republic, Iraq, Kazakhstan, Nepal, Nigeria and Uzbekistan.
Of 29 countries that have currently suspended measles campaigns because of the pandemic, 18 are reporting outbreaks. An additional 13 countries are considering postponement. According to the Measles and Rubella Initiative, 178 million people are at risk of missing measles shots in 2020.
The risk now is “an epidemic in a few months’ time that will kill more children than Covid,” said Chibuzo Okonta, the president of Doctors Without Borders in West and Central Africa.
As the pandemic lingers, the W.H.O. and other international public health groups are now urging countries to carefully resume vaccination while contending with the coronavirus.
A Doctors Without Borders motorcycle convoy carrying measles vaccine crossed a log bridge in Mongala Province of the Democratic Republic of Congo in February. Credit: Hereward Holland/Reuters.
“Immunization is one of the most powerful and fundamental disease prevention tools in the history of public health,” said Dr. Tedros Adhanom Ghebreyesus, director general of the W.H.O., in a statement. “Disruption to immunization programs from the Covid-19 pandemic threatens to unwind decades of progress against vaccine-preventable diseases like measles.”
But the obstacles to restarting are considerable. Vaccine supplies are still hard to come by. Health care workers are increasingly working full time on Covid-19, the infection caused by the coronavirus. And a new wave of vaccine hesitancy is keeping parents from clinics.
Many countries have yet to be hit with the full force of the pandemic itself, which will further weaken their capabilities to handle outbreaks of other diseases.
“We will have countries trying to recover from Covid and then facing measles. It would stretch their health systems further and have serious economic and humanitarian consequences,” said Dr. Robin Nandy, chief of immunization for UNICEF, which supplies vaccines to 100 countries, reaching 45 percent of children under 5.
The breakdown of vaccine delivery also has stark implications for protecting against the coronavirus itself.
At a global summit earlier this month, Gavi, the Vaccine Alliance, a health partnership founded by the Bill and Melinda Gates Foundation, announced it had received pledges of $8.8 billion for basic vaccines to children in poor and middle-income countries, and was beginning a drive to deliver Covid-19 vaccines, once they’re available.
But as services collapse under the pandemic, “they are the same ones that will be needed to send out a Covid vaccine,” warned Dr. Katherine O’Brien, the W.H.O.’s director of immunization, vaccines and biologicals, during a recent webinar on immunization challenges.
Battling Measles in Congo
Children waited to be registered for the measles vaccine in Mbata-Siala, in western Democratic Republic of Congo, in March. Credit: Junior Kannah/Agence France-Presse — Getty Images.
Three health care workers with coolers full of vaccines and a support team of town criers and note-takers recently stepped into a motorized wooden canoe to set off down the wide Tshopo River in the Democratic Republic of Congo.
Although measles was breaking out in all of the country’s 26 provinces, the pandemic had shut down many inoculation programs weeks earlier.
The crew in the canoe needed to strike a balance between preventing the transmission of a new virus that is just starting to hit Africa hard and stopping an old, known killer. But when the long, narrow canoe pulled in at riverside communities, the crew’s biggest challenge turned out not to be the mechanics of vaccinating children while observing the pandemic’s new safety strictures. Instead, the crew found themselves working hard just to persuade villagers to allow their children to be immunized at all.
Many parents were convinced that the team was lying about the vaccine — that it was not for measles but, secretly, an experimental coronavirus vaccine, for which they would be unwitting guinea pigs.
In April, French-speaking Africa had been outraged by a French television interview in which two researchers said coronavirus vaccines should be tested in Africa — a remark that reignited memories of a long history of such abuses. And in Congo, the virologist in charge of the coronavirus response said that the country had indeed agreed to take part in clinical vaccine trials this summer. Later, he clarified that any vaccine would not be tested in Congo until it had been tested elsewhere. But pernicious rumors had already spread.
The team cajoled parents as best they could. Although vaccinators throughout Tshopo ultimately immunized 16,000 children, 2,000 others eluded them.
This had been the year that Congo, the second-largest country in Africa, was to launch a national immunization program. The urgency could not have been greater. The measles epidemic in the country, which started in 2018, has run on and on: Since this January alone, there have been more than 60,000 cases and 800 deaths. Now, Ebola has again flared, in addition to tuberculosis and cholera, which regularly strike the country.
Vaccines exist for all these diseases, although they are not always available. In late 2018, the country began an immunization initiative in nine provinces. It was a feat of coordination and initiative, and in 2019, the first full year, the percentage of fully immunized children jumped from 42 to 62 percent in Kinshasa, the capital.
This spring, as the program was being readied for its nationwide rollout, the coronavirus struck. Mass vaccination campaigns, which often mean summoning hundreds of children to sit close together in schoolyards and markets, seemed guaranteed to spread coronavirus. Even routine immunization, which typically occurs in clinics, became untenable in many areas.
The country’s health authorities decided to allow vaccinations to continue in areas with measles but no coronavirus cases. But the pandemic froze international flights that would bring medical supplies, and several provinces began running out of vaccines for polio, measles and tuberculosis.
When immunization supplies finally arrived in Kinshasa, they could not be moved around the country. Domestic flights had been suspended. Ground transport was not viable because of shoddy roads. Eventually, a United Nations peacekeeping mission ferried supplies on its planes.
Still, health workers, who had no masks, gloves or sanitizing gel, worried about getting infected; many stopped working. Others were diverted to be trained for Covid.
The cumulative impact has been particularly dire for polio eradication — around 85,000 Congolese children have not received that vaccine.
But the disease that public health officials are most concerned about erupting is measles.
More contagious than Covid
Health workers immunizing against measles in Manila last month. Credit: Aaron Favila/Associated Press.
Measles virus spreads easily by aerosol — tiny particles or droplets suspended in the air — and is far more contagious than the coronavirus, according to experts at the Centers for Disease Control and Prevention.
“If people walk into a room where a person with measles had been two hours ago and no one has been immunized, 100 percent of those people will get infected,” said Dr. Yvonne Maldonado, a pediatric infectious disease expert at Stanford University.
In poorer countries, the measles mortality rate for children under 5 ranges between 3 and 6 percent; conditions like malnutrition or an overcrowded refugee camp can increase the fatality rate. Children may succumb to complications such as pneumonia, encephalitis and severe diarrhea.
In 2018, the most recent year for which data worldwide has been compiled, there were nearly 10 million estimated cases of measles and 142,300 related deaths. And global immunization programs were more robust then.
Before the coronavirus pandemic in Ethiopia, 91 percent of children in the capital, Addis Ababa, received their first measles vaccination during routine visits, while 29 percent in rural regions got them. (To prevent an outbreak of a highly infectious disease like measles, the optimum coverage is 95 percent or higher, with two doses of vaccine.) When the pandemic struck, the country suspended its April measles campaign. But the government continues to report many new cases.
“Outbreak pathogens don’t recognize borders,” said Dr. O’Brien of the W.H.O. “Especially measles: Measles anywhere is measles everywhere.”
Wealthier countries’ immunization rates have also been plunging during the pandemic. Some American states report drops as steep as 70 percent below the same period a year earlier, for measles and other diseases.
Once people start traveling again, the risk of infection will surge. “It keeps me up at night,” said Dr. Stephen L. Cochi, a senior adviser at the global immunization division at the C.D.C. “These vaccine-preventable diseases are just one plane ride away.”
Starting again
Hawa Hamadou, a health worker at the Gamkalé health center in Niamey, Niger, has seen a drop in visits by mothers, who are afraid to bring their children for immunizations. Credit: Juan Haro/UNICEF.
After the W.H.O. and its vaccine partners released the results of a survey last month showing that 80 million babies under a year old were at risk of missing routine immunizations, some countries, including Ethiopia, the Central African Republic and Nepal, began trying to restart their programs.
Uganda is now supplying health workers with motorbikes. In Brazil, some pharmacies are offering drive-by immunization services. In the Indian state of Bihar, a 50-year-old health care worker learned to ride a bicycle in three days so she could take vaccines to far-flung families. UNICEF chartered a flight to deliver vaccines to seven African countries.
Dr. Cochi of the C.D.C., which provides technical and program support to more than 40 countries, said that whether such campaigns can be conducted during the pandemic is an open question. “It will be fraught with limitations. We’re talking low-income countries where social distancing is not a reality, not possible,” he said, citing Brazilian favelas and migrant caravans.
He hopes that polio campaigns will resume swiftly, fearing that the pandemic could set back a global, decades-long effort to eradicate the disease.
Dr. Cochi is particularly worried about Pakistan and Afghanistan, where 61 cases of wild poliovirus Type 1 have been reported this year, and about Chad, Ghana, Ethiopia and Pakistan, where cases of Type 2 poliovirus, mutated from the oral vaccine,have appeared.
Thabani Maphosa, a managing director at Gavi, which partners with 73 countries to purchase vaccines, said that at least a half dozen of those countries say they cannot afford their usual share of vaccine costs because of the economic toll of the pandemic.
If the pandemic cleared within three months, Mr. Maphosa said, he believed the international community could catch up with immunizations over the next year and a half.
“But our scenarios are not telling us that will happen,” he added.
Jan Hoffman reported from New York, and Ruth Maclean from Dakar, Senegal.
What’s the risk of catching coronavirus from a surface? Touching contaminated objects and then infecting ourselves with the germs is not typically how the virus spreads. But it can happen. A number of studies of flu, rhinovirus, coronavirus and other microbes have shown that respiratory illnesses, including the new coronavirus, can spread by touching contaminated surfaces, particularly in places like day care centers, offices and hospitals. But a long chain of events has to happen for the disease to spread that way. The best way to protect yourself from coronavirus — whether it’s surface transmission or close human contact — is still social distancing, washing your hands, not touching your face and wearing masks.
Does asymptomatic transmission of Covid-19 happen? So far, the evidence seems to show it does. A widely cited paper published in April suggests that people are most infectious about two days before the onset of coronavirus symptoms and estimated that 44 percent of new infections were a result of transmission from people who were not yet showing symptoms. Recently, a top expert at the World Health Organization stated that transmission of the coronavirus by people who did not have symptoms was “very rare,” but she later walked back that statement.
How does blood type influence coronavirus? A study by European scientists is the first to document a strong statistical link between genetic variations and Covid-19, the illness caused by the coronavirus. Having Type A blood was linked to a 50 percent increase in the likelihood that a patient would need to get oxygen or to go on a ventilator, according to the new study.
How many people have lost their jobs due to coronavirus in the U.S.? The unemployment rate fell to 13.3 percent in May, the Labor Department said on June 5, an unexpected improvement in the nation’s job market as hiring rebounded faster than economists expected. Economists had forecast the unemployment rate to increase to as much as 20 percent, after it hit 14.7 percent in April, which was the highest since the government began keeping official statistics after World War II. But the unemployment rate dipped instead, with employers adding 2.5 million jobs, after more than 20 million jobs were lost in April.
Will protests set off a second viral wave of coronavirus? Mass protests against police brutality that have brought thousands of people onto the streets in cities across America are raising the specter of new coronavirus outbreaks, prompting political leaders, physicians and public health experts to warn that the crowds could cause a surge in cases. While many political leaders affirmed the right of protesters to express themselves, they urged the demonstrators to wear face masks and maintain social distancing, both to protect themselves and to prevent further community spread of the virus. Some infectious disease experts were reassured by the fact that the protests were held outdoors, saying the open air settings could mitigate the risk of transmission.
How do we start exercising again without hurting ourselves after months of lockdown? Exercise researchers and physicians have some blunt advice for those of us aiming to return to regular exercise now: Start slowly and then rev up your workouts, also slowly. American adults tended to be about 12 percent less active after the stay-at-home mandates began in March than they were in January. But there are steps you can take to ease your way back into regular exercise safely. First, “start at no more than 50 percent of the exercise you were doing before Covid,” says Dr. Monica Rho, the chief of musculoskeletal medicine at the Shirley Ryan AbilityLab in Chicago. Thread in some preparatory squats, too, she advises. “When you haven’t been exercising, you lose muscle mass.” Expect some muscle twinges after these preliminary, post-lockdown sessions, especially a day or two later. But sudden or increasing pain during exercise is a clarion call to stop and return home.
My state is reopening. Is it safe to go out?States are reopening bit by bit. This means that more public spaces are available for use and more and more businesses are being allowed to open again. The federal government is largely leaving the decision up to states, and some state leaders are leaving the decision up to local authorities. Even if you aren’t being told to stay at home, it’s still a good idea to limit trips outside and your interaction with other people.
What are the symptoms of coronavirus? Common symptoms include fever, a dry cough, fatigue and difficulty breathing or shortness of breath. Some of these symptoms overlap with those of the flu, making detection difficult, but runny noses and stuffy sinuses are less common. The C.D.C. has also added chills, muscle pain, sore throat, headache and a new loss of the sense of taste or smell as symptoms to look out for. Most people fall ill five to seven days after exposure, but symptoms may appear in as few as two days or as many as 14 days.
How can I protect myself while flying? If air travel is unavoidable, there are some steps you can take to protect yourself. Most important: Wash your hands often, and stop touching your face. If possible, choose a window seat. A study from Emory University found that during flu season, the safest place to sit on a plane is by a window, as people sitting in window seats had less contact with potentially sick people. Disinfect hard surfaces. When you get to your seat and your hands are clean, use disinfecting wipes to clean the hard surfaces at your seat like the head and arm rest, the seatbelt buckle, the remote, screen, seat back pocket and the tray table. If the seat is hard and nonporous or leather or pleather, you can wipe that down, too. (Using wipes on upholstered seats could lead to a wet seat and spreading of germs rather than killing them.)
How do I take my temperature? Taking one’s temperature to look for signs of fever is not as easy as it sounds, as “normal” temperature numbers can vary, but generally, keep an eye out for a temperature of 100.5 degrees Fahrenheit or higher. If you don’t have a thermometer (they can be pricey these days), there are other ways to figure out if you have a fever, or are at risk of Covid-19 complications.
Should I wear a mask? The C.D.C. has recommended that all Americans wear cloth masks if they go out in public. This is a shift in federal guidance reflecting new concerns that the coronavirus is being spread by infected people who have no symptoms. Until now, the C.D.C., like the W.H.O., has advised that ordinary people don’t need to wear masks unless they are sick and coughing. Part of the reason was to preserve medical-grade masks for health care workers who desperately need them at a time when they are in continuously short supply. Masks don’t replace hand washing and social distancing.
What should I do if I feel sick?If you’ve been exposed to the coronavirus or think you have, and have a fever or symptoms like a cough or difficulty breathing, call a doctor. They should give you advice on whether you should be tested, how to get tested, and how to seek medical treatment without potentially infecting or exposing others.
Summary: Researchers describe a single function that accurately describes all existing available data on active COVID-19 cases and deaths — and predicts forthcoming peaks.
As of late May, COVID-19 has killed more than 325,000 people around the world. Even though the worst seems to be over for countries like China and South Korea, public health experts warn that cases and fatalities will continue to surge in many parts of the world. Understanding how the disease evolves can help these countries prepare for an expected uptick in cases.
This week in the journal Frontiers in Physics, researchers describe a single function that accurately describes all existing available data on active cases and deaths — and predicts forthcoming peaks. The tool uses q-statistics, a set of functions and probability distributions developed by Constantino Tsallis, a physicist and member of the Santa Fe Institute’s external faculty. Tsallis worked on the new model together with Ugur Tirnakli, a physicist at Ege University, in Turkey.
“The formula works in all the countries in which we have tested,” says Tsallis.
Neither physicist ever set out to model a global pandemic. But Tsallis says that when he saw the shape of published graphs representing China’s daily active cases, he recognized shapes he’d seen before — namely, in graphs he’d helped produce almost two decades ago to describe the behavior of the stock market.
“The shape was exactly the same,” he says. For the financial data, the function described probabilities of stock exchanges; for COVID-19, it described daily the number of active cases — and fatalities — as a function of time.
Modeling financial data and tracking a global pandemic may seem unrelated, but Tsallis says they have one important thing in common. “They’re both complex systems,” he says, “and in complex systems, this happens all the time.” Disparate systems from a variety of fields — biology, network theory, computer science, mathematics — often reveal patterns that follow the same basic shapes and evolution.
The financial graph appeared in a 2004 volume co-edited by Tsallis and the late Nobelist Murray Gell-Mann. Tsallis developed q-statitics, also known as “Tsallis statistics,” in the late 1980s as a generalization of Boltzmann-Gibbs statistics to complex systems.
In the new paper, Tsallis and Tirnakli used data from China, where the active case rate is thought to have peaked, to set the main parameters for the formula. Then, they applied it to other countries including France, Brazil, and the United Kingdom, and found that it matched the evolution of the active cases and fatality rates over time.
The model, says Tsallis, could be used to create useful tools like an app that updates in real-time with new available data, and can adjust its predictions accordingly. In addition, he thinks that it could be fine-tuned to fit future outbreaks as well.
“The functional form seems to be universal,” he says, “Not just for this virus, but for the next one that might appear as well.”
Editor’s note: Some of our covid-19 coverage is free for readers of The Economist Today, our daily newsletter. For more stories and our pandemic tracker, see our coronavirus hub
AMERICA HAS passed a grim milestone: 100,000 deaths from a novel coronavirus that began to spread half a year and half a world away. Many Americans think their president has handled the epidemic disastrously, that their country has been hit uniquely hard and that there is a simple causal relationship between the two. The 100,000, which does not include excess deaths mistakenly attributed to other causes, is higher than any other country’s. It has routinely been compared with the 60,000 American casualties in the Vietnam war. A Trump Death Clock in Times Square purports to show how many lives the president’s ineptitude has cost: as we went to press it stood at 60,262. Yet this widespread conviction that America has failed because of Donald Trump is not supported by the numbers. Or, at least, not yet.
The official death rate in America is about the same as in the European Union—which also has excess deaths, but has less erratic leaders and universal health care. Overall, America has fared a bit worse than Switzerland and a bit better than the Netherlands, neither of which is a failed state. New York has been hit about as hard as Lombardy in northern Italy; California acted early and is currently similar to Germany; so far, rural states have, like central Europe, been spared the worst. This reflects two things, both of which will matter now that America is reopening before it has the virus fully under control.
The first is that covid-19, when it first hit, displayed an indifference to presidents and their plans. Around the world it has killed in large, dense and connected cities like New York, London and Paris, and where people are crammed together, including care homes, slaughterhouses and prisons. In some countries, including America, testing was snarled up in red tape.
Having seen what was happening in China, Mr Trump could have acted sooner—as Taiwan, Singapore and Vietnam did. He has failed to do things ordinarily expected of an American president in a crisis, such as giving clear government advice or co-ordinating a federal response. Instead, he has touted quack remedies and spent the days when America passed its sombre milestone spreading suspicion of the voting system and accusing a television host of committing a murder that never happened. All this is reprehensible and it may have been costly. Yet, tempting as it is to conclude that the president’s failures bear most of the blame for covid-19’s spread through America, the reality is more complicated (see Briefing).
That leads to the second feature of the country’s response to covid-19. The virus was always going to be hard on a population with high levels of poverty, obesity and diseases such as diabetes, especially among minorities (see Lexington). But, to a remarkable degree, other layers of government have adapted around the hole where the president should have been. The federal system has limited the damage, thanks to its decentralised decision-making. Lockdowns vary by state, city and county. California responded as soon as it saw cases. In the north-east governors largely ignored the White House and got on with coping with the disease, earning the Republican governors of Maryland and Massachusetts the president’s enmity, but high approval ratings. In Florida, though the governor was reluctant to impose a lockdown, county officials went ahead and did so anyway.
Contrary to demands for nationwide rules, this is a strength not a weakness, and will become more so as the pandemic runs its course. In the best-organised states, which have built up testing capacity, it helps ensure that flare-ups can be spotted quickly and rules adjusted accordingly. Because each region is different, that is more efficient than a nationwide approach.
One way democracies can deal with the virus is to draw on reserves of trust. People must behave in ways that protect fellow citizens whom they have never met, even if they themselves are feeling fine. Americans trust their local officials far more than the president or the federal government. And when it comes to public health those local officials have real power. Without this balancing feature, America might today look like Brazil, where a president with a similar love of hydroxychloroquine and distaste for face masks is wreaking havoc (see article).
If the public-health response in the United States so far matches Europe’s, its economic response to the virus may turn out better. True, the unemployment rate in America is 15%, double that in the EU. Yet in Europe most governments are protecting jobs that may no longer exist once lockdowns end rather than focusing help on the unemployed as America’s has. The EU is probably delaying a painful adjustment. Congress, not known for passing consequential legislation with big bipartisan majorities, agreed on a vastly bigger fiscal stimulus than in the financial crisis a decade ago. With a Democrat in the White House and a Republican-controlled Senate, America might not have mustered a response that was either so rapid or so large.
America still has a hard road ahead. Were daily fatalities to remain at today’s level, which is being celebrated as a sign that the pandemic is waning, another 100,000 people would die by the end of the year. To prevent that, America needs to work with the system it has, trusting local politicians to balance the risks of reopening against the cost of lockdowns.
In the next months the infrastructure built during the lockdown must prove itself. Because the virus has yet to decline in some states, it may flare up in new places, which will then need targeted lockdowns. The capacity to test, vital to spotting clusters of infection, has increased, but is still lacking in some places. Almost all the states lack the contact tracers needed to work out who needs testing and quarantining. When it considers how to withdraw fiscal support, Congress should remember this.
That America and Europe have fared similarly in the pandemic does not absolve Mr Trump. This is the first international crisis since 1945 in which America has not only spurned global leadership but, by cutting funds to the World Health Organisation, actively undermined a co-ordinated international response. That matters, as does Mr Trump’s inability to cleave to a consistent message or to speak to the country in words that do not enrage half of the population. Yet four years after Mr Trump was elected, the time to be surprised by his behaviour has long gone. Luckily, he has mattered less than most Americans think.■
This article appeared in the Leaders section of the print edition under the headline “The American way”
Ali Mokdad dirige parte das projeções feitas pelo IHME, instituto de métrica da Universidade de Washington utilizado pela Casa Branca como um dos principais modelos para monitorar Covid-19.
Desde o meio de maio, Mokdad e sua equipe acompanham o avanço da pandemia no Brasil e suas conclusões são bastantes sombrias. Na segunda-feira (25), o instituto atualizou para cima a expectativa de mortes pela doença no país: de 88 mil para mais de 125 mil óbitos previstos até agosto.
Em entrevista à Folha, Mokdad diz que a tendência de casos e mortes no país é de alta e que a situação pode ser ainda pior se governo e população não levarem a crise a sério e adotarem “lockdown” por duas semanas.
“As infeções e mortes vão crescer e, o mais assustador, haverá a sobrecarga total do sistema de saúde.” Caso cumpra o confinamento total por 14 dias, explica Mokdad, o Brasil conseguirá controlar a propagação do vírus e poderá fazer a reabertura das atividades econômicas de maneira estratégica –e até mais rapidamente.
Especialista em saúde pública, diz sofrer críticas por ter um modelo que varia bastante, mas, no caso da pandemia, prefere que suas projeções se ajustem com o tempo. “Se os brasileiros ficarem em casa por duas semanas, meus números vão baixar. E não porque fiz algo errado, mas porque os brasileiros fizeram algo certo.”
Qual a situação da pandemia no Brasil? Infelizmente o que vemos no Brasil é uma tendência de aumento de casos, que vai resultar no crescimento das mortes no país. Isso se dá por várias razões. Primeiro porque o país não entrou em “lockdown” cedo para impedir a propagação do vírus. O governo e a população brasileira não levaram isso a sério e não fizeram logo as coisas certas para impedir a transmissão do vírus.
Segundo, há muita disparidade no Brasil e a Covid-19 aumenta isso. Nesse caso, é preciso proteger não só os trabalhadores de saúde mas os trabalhadores de serviços essenciais, pessoas pobres que trabalham em funções que as obrigam a sair de casa. Elas não estão protegidas e estão morrendo. A terceira e mais importante preocupação é a sobrecarga do sistema de saúde. Se o país não agir, vai haver mais casos no inverno e não haverá tempo para se preparar. É perigoso e arriscado. Se você colocar tudo isso junto, o Brasil ainda vai enfrentar sérias dificuldades diante da Covid-19.
Em duas semanas, o IHME aumentou as projeções de morte no Brasil de 88 mil para mais de 125 mil até agosto. O que aconteceu? Adicionamos mais estados [de 11 para 19] na nossa projeção, isso é uma coisa. Mas estamos vendo no Brasil mais surtos e casos do que esperávamos. O país está testando mais e encontrando mais casos, mas, mesmo quando ajustamos para os testes, há uma tendência de alta.
No Brasil há também um erro de suposição quando falamos de circulação. Os dados [de mobilidade da população] são baseados no Facebook e no Google, ou seja, em smartphones, ou seja, em pessoas mais ricas. Percebemos que a circulação não parou nas favelas, por exemplo, em lugares onde pessoas mais pobres precisam sair para trabalhar. Se as pessoas se recusarem a levar isso a sério, infelizmente vamos ver mais casos e mortes.
Quais medidas precisam ser tomadas? Fechar escolas e universidades, impedir grandes aglomerações e encontros de pessoas, fechar os estabelecimentos não essenciais, igrejas, templos e locais religiosos. Nos locais essenciais, como mercados e farmácias, é preciso estabelecer regras, limitando o número de pessoas dentro, garantindo que elas se mantenham distantes umas das outras.
A última e mais importante coisa é pedir para quem precisa sair de casa—e sabemos que há quem precise— usar máscara e manter distância de 2 metros de outras pessoas. Para o sistema de saúde, é aumentar a capacidade de tratamento, de detectar cedo a chegada de um surto, fazendo rastreamento e o isolamento de casos, o que é um desafio para o Brasil, onde muitas vezes dez pessoas vivem em uma mesma casa.
Se o Brasil não cumprir essas medidas, qual é o pior cenário para o país? As infeções e mortes vão crescer e, a parte mais assustadora, haverá a sobrecarga total do sistema de saúde. Isso vai causar mais prejuízo à economia do que se fizer o isolamento por duas semanas. Se a população ficar em casa e levar isso a sério por duas semanas, registraremos diminuição da propagação do vírus e poderemos reabrir em fases. É preciso garantir que a retomada econômica seja feita de maneira estratégica, por setores.
É possível evitar o pico de 1.500 mortes diárias em julho e as 125 mil mortes até agosto se o país parar agora? Sim. O Brasil está em uma situação muito difícil e pode ser assim por muito tempo, mas ainda há esperança. Se o governo e a população pararem por duas semanas, podemos parar a circulação do vírus e reabrir o comércio. Se você olhar para estados americanos, como Nova York, depois que há o “lockdown”, as mortes e os casos diminuem. O “lockdown” salvou muitas vidas nos EUA. Fizemos as projeções para o Brasil de 125 mil mortes até 4 de agosto, mas não significa que vai acontecer, podemos parar isso. É preciso que cada brasileiro faça sua parte.
O presidente Jair Bolsonaro é contra medidas de distanciamento social, compara a Covid-19 com uma gripezinha e defende um medicamento com eficácia não comprovada contra a doença. Como essa postura pode impactar a situação do Brasil? Aqui nos EUA temos também uma situação política nesse sentido, infelizmente. Não sou político, vejo os números e dou conselhos a partir do que concluo deles. Pelos dados, o Brasil precisa de uma ação coordenada, caso contrário, vamos ter muitas perdas.
Mas precisamos ter uma coisa clara: Covid-19 não é uma gripe, causa mais mortalidade que gripe, a gripe não causa AVC e nem ataca os pulmões da maneira que a Covid-19 ataca. Contra Covid-19 não há medicamento e ponto final. Não tem vacina. Não é possível comparar Covid-19 e gripe. Fazer isso é passar mensagem errada. Dizer para a população que é possível sair e ver quem pega a doença é inaceitável, é falha de liderança.
Como ganhar a confiança dos governos e da população com projeções que variam tanto e com tanta gente trabalhando com dados sobre o tema? Há muita gente fazendo projeção mas, pela primeira vez na história da ciência, todos concordamos. Os números podem ser diferentes, mas a mensagem mais importante é a mesma: isso é um vírus letal e temos que levá-lo a sério. Meus números mudam porque as pessoas mudam. Se os brasileiros ficarem em casa por duas semanas, meus números vão baixar. E não porque fiz algo errado, mas porque os brasileiros fizeram algo certo. Aprendemos que o modelo muda se novos dados aparecem.
O sr. já foi acusado de ser alarmista ou de produzir notícias falsas quando seus números mudam? Acusado é demais, mas tem gente que fala que meus números são mais altos ou mais baixos do que deveriam ser, e isso eu nem resposto, porque não é um debate científico, é um debate político. No debate científico está todo mundo a bordo com a mesma mensagem.
Como é trabalhar tendo isso em vista, com números tão sensíveis e poderosos? A gente não dorme muito por esses dias, é muito trabalho. É muito difícil dizer que 125 mil pessoas vão morrer no Brasil até agosto. Isso não é um número, são famílias, amigos, é muito duro.






















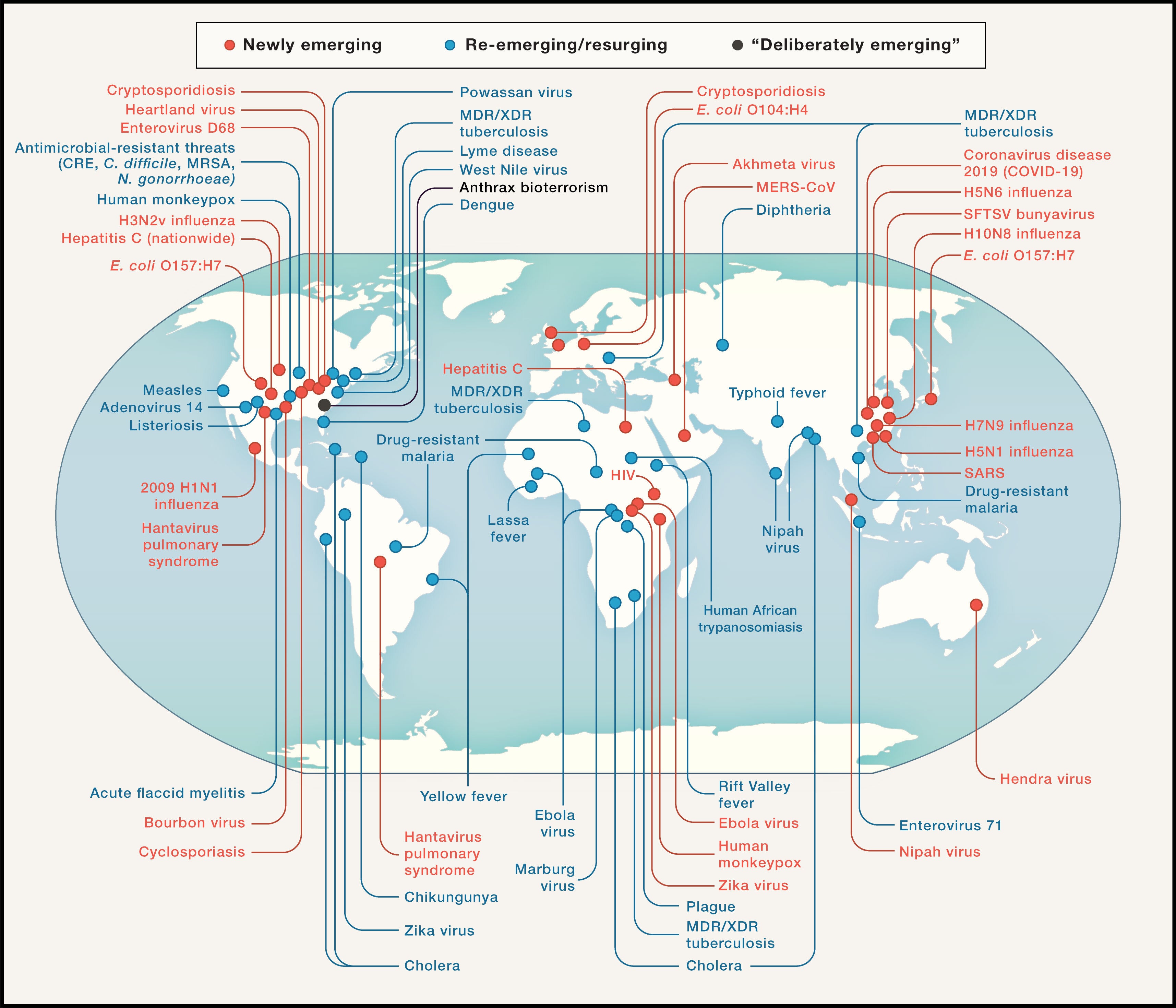

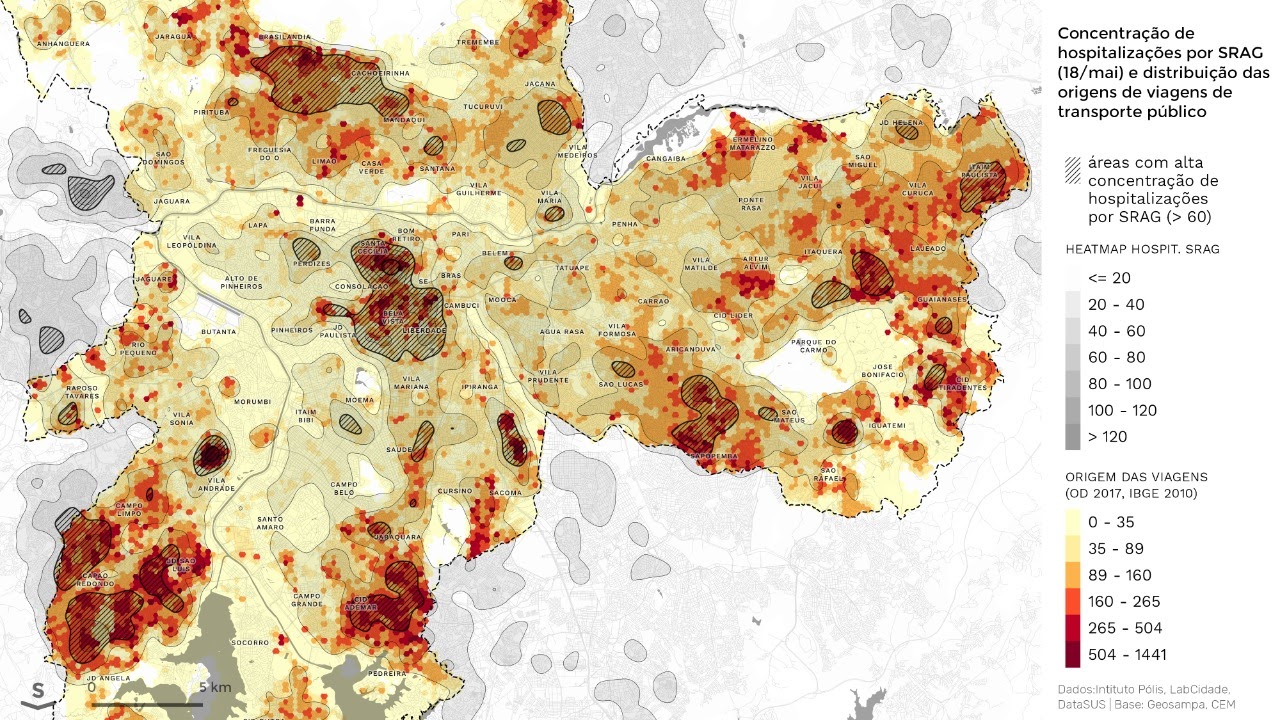


![Students at a university in Germany evaluate data from COVID-19 patients [Reuters]](https://www.aljazeera.com/mritems/imagecache/mbdxxlarge/mritems/Images/2020/6/15/708e7f7043ac44799e463b38335a062d_18.jpg "Data fog: Why some countries' coronavirus numbers do not add up")









{kind=link}
{kind=link}
{kind=link}
Você precisa fazer login para comentar.