The climate crisis resembles a huge planetary lockdown, trapping humanity within an ever-deteriorating environment
‘The shallow layer of earth in which we live … has been transformed into a habitable milieu by the aeons-long labour of evolution.’ Photograph: Jon Helgason/Alamy
Fri 24 Dec 2021 14.00 GMT
There is a moment when a never-ending crisis turns into a way of life. This seems to be the case with the pandemic. If so, it’s wise to explore the permanent condition in which it has left us. One obvious lesson is that societies have to learn once again to live with pathogens, just as they learned to when microbes were first made visible by the discoveries of Louis Pasteur and Robert Koch.
These discoveries were concerned with only one aspect of microbial life. When you also consider the various sciences of the earth system, another aspect of viruses and bacteria comes to the fore. During the long geochemical history of the earth, microbes, together with fungi and plants, have been essential, and are still essential, to the very composition of the environment in which we humans live. The pandemic has shown us that we will never escape the invasive presence of these living beings, entangled as we are with them. They react to our actions; if they mutate, we have to mutate as well.
This is why the many national lockdowns, imposed on citizens to help them survive the virus, are a powerful analogy for the situation in which humanity finds itself detained for good. Lockdown was painful enough, and yet many ways have been found, thanks in part to vaccination, to allow people to resume a semblance of normal life. But there is no possibility of such a resumption if you consider that all living forms are locked down for good inside the limits of the earth. And by “earth” I don’t mean the planet as it can be seen from space, but its very superficial pellicle, the shallow layer of earth in which we live, and which has been transformed into a habitable milieu by the aeons-long labour of evolution.
This thin matrix is what geochemists call the “critical zone”, the only layer of earth where terrestrial life can flourish. It’s in this finite space where everything we care for and everything we have ever encountered exists.There is no way of escaping our earth-bound existence; as young climate activists shout: “There is no planet B.” Here is the connection between the Covid lockdowns we have experienced in the past two years, and the much larger but definitive state of lockdown that we find ourselves in: we are trapped in an environment that we have already altered irreversibly.
If we have been made aware of the agency of viruses in shaping our social relations, we must now reckon with the fact that they will also be moulded for ever by the climate crisis and the quick reactions of ecosystems to our actions. The feeling that we live in a new space appears again at the local as well as the global level. Why would all nations convene in Glasgow to keep global temperature rises below some agreed upon limit, if they did not have the sensation that a huge lid had been put over their territory? When you look up at the blue sky, are you not aware that you are now under some sort of dome inside which you are locked?
Gone is the infinite space; now you are responsible for the safety of this overbearing dome as much as you are for your own health and wealth. It weighs on you, body and soul. To survive under these new conditions we have to undergo a sort of metamorphosis.
This is where politics enters. It is very difficult for most people used to the industrialised way of life, with its dream of infinite space and its insistence on emancipation and relentless growth and development, to suddenly sense that it is instead enveloped, confined, tucked inside a closed space where their concerns have to be shared with new entities: other people of course, but also viruses, soils, coal, oil, water, and, worst of all, this damned, constantly shifting climate.
This disorienting shift is unprecedented, even cosmological, and it is already a source of deep political divisions. Although the sentence “you and I don’t live on the same planet” used to be a joking expression of dissent, it has become true of our present reality. We do live on different planets, with rich people employing private fire fighters and scouting for climate bunkers, while their poorer counterparts are forced to migrate, suffer and die amid the worst consequences of the crisis.
This is why it is important not to misconstrue the political conundrum of our present age. It is of the same magnitude as when, from the 17th century onward, westerners had to shift from the closed cosmos of the past to the infinite space of the modern period. As the cosmos seemed to open, political institutions had to be invented to work through the new and utopian possibilities offered by the Enlightenment. Now, in reverse, the same task falls to present generations: what new political institutions could they invent to cope with people so divided that they belong to different planets?
It would be a mistake to believe that the pandemic is a crisis that will end, instead of the perfect warning for what is coming, what I call the new climatic regime. It appears that all the resources of science, humanities and the arts will have to be mobilised once again to shift attention to our shared terrestrial condition.
Bruno Latour is a philosopher and anthropologist, the author of After Lockdown: A Metamorphosis and the winner of the 2013 Holberg prize
O Harvard Global Health Institute e o Center for Climate, Health, and the Global Environment, da escola de saúde pública de Harvard, reuniram pesquisadores para analisar a literatura científica disponível até o momento e apontar caminhos para prevenção de novas pandemias.
Um dos pontos citados diretamente pelo relatório é o desmatamento. Os cientistas apontam como exemplo o aumento, após processos de desmate na América Central, de roedores como reservatórios de hantavírus —que, em caso de contaminação de humanos, pode levar à síndrome pulmonar por hantavírus.
A expansão de áreas agricultáveis também está ligada ao surgimento de novas doenças. Isso ocorre, afirmam os pesquisadores, pelo potencial de tal ação aproximar humanos a rebanhos de animais silvestres.
“Cerca de 22% da área terrestre em hotspots de biodiversidade, muitas vezes sobrepostos a hotspots de doenças emergentes, é ameaçada por expansão agrícola”, afirma o documento.
O relatório aponta que processos de urbanização descontrolados e sem planejamento podem ter um papel no surgimento de doenças, pelas mudanças no uso de terra e por possíveis grandes concentrações de pessoas e condições de vida ruins.
Há ainda fazendas de animais como outro ponto importante em eventos de spillover, ou transbordamento, em tradução do inglês, de zoonoses —basicamente, quando um vírus salta de uma espécie para uma nova, como para humanos. Os pesquisadores apontam a baixa diversidade genética e o elevado número de animais mantidos em alguns desses locais.
Os cientistas dão como exemplo a transmissão —inicialmente entre suínos e depois para trabalhadores agrícolas— do vírus nipah, na Malásia, em fazendas de porcos com altas concentrações de animais.
Além disso, a caça, o consumo e o comércio de animais selvagens também podem provocar o spillover.
A crise climática é mais um fator que deve impactar nos riscos de aparecimento de novas doenças no mundo, considerando as alterações que ocorrerão em ecossistemas. Segundo os pesquisadores, existe a possibilidade de habitats adequados para espécies diminuírem, o que poderia promover mais encontros entre vida selvagem e humanos, e, com isso, mais eventos de spillover.
“A redução de habitats e disponibilidade de néctar para morcegos, por exemplo, têm pressionado esses animais a buscar fontes alternativas de alimento em áreas urbanas e arredores”, afirmam os cientistas no relatório.
Por fim, os pesquisadores convocados por Harvard apontam estratégias para evitar eventos de spillover. A conservação ambiental é a primeira a ser destacada no relatório.
Outras estratégias listadas são restrições ao consumo de animais selvagens, investigações sobre vírus na vida selvagem e uma rede global de vigilância de patógenos em humanos, animais criados para abate e vida silvestre, entre outras iniciativas.
Segundo o documento, são baixos os investimentos destinados a impedir spillover. “Não mais do que US$ 4 bilhões [R$ 21,5 bilhões] são gastos a cada ano em todo o mundo em atividades de prevenção de transbordamento. A Covid-19 sozinha resultou em uma perda de PIB global estimada em US$ 4 trilhões [R$ 21,5 trilhões], ou cerca de US$ 40 bilhões [R$ 215 bilhões] por ano durante um século”, aponta o relatório.
Ecosystems with a diversity of mammals, including larger-bodies and longer lived creatures like foxes, are better for our health. Credit: Ali Rajabali / Flickr
A growing body of evidence suggests that biodiversity loss increases our exposure to both new and established zoonotic pathogens. Restoring and protecting nature is essential to preventing future pandemics. So reports a new Proceedings of the National Academy of Sciences (PNAS) paper that synthesizes current understanding about how biodiversity affects human health and provides recommendations for future research to guide management.
Lead author Felicia Keesing is a professor at Bard College and a Visiting Scientist at Cary Institute of Ecosystem Studies. She explains, “There’s a persistent myth that wild areas with high levels of biodiversity are hotspots for disease. More animal diversity must equal more dangerous pathogens. But this turns out to be wrong. Biodiversity isn’t a threat to us, it’s actually protecting us from the species most likely to make us sick.”
Zoonotic diseases like COVID-19, SARS, and Ebola are caused by pathogens that are shared between humans and other vertebrate animals. But animal species differ in their ability to pass along pathogens that make us sick.
Rick Ostfeld is a disease ecologist at Cary Institute and a co-author on the paper. He explains, “Research is mounting that species that thrive in developed and degraded landscapes are often much more efficient at harboring pathogens and transmitting them to people. In less-disturbed landscapes with more animal diversity, these risky reservoirs are less abundant and biodiversity has a protective effect.”
Rodents, bats, primates, cloven-hooved mammals like sheep and deer, and carnivores have been flagged as the mammal taxa most likely to transmit pathogens to humans. Keesing and Ostfeld note, “The next emerging pathogen is far more likely to come from a rat than a rhino.”
This is because animals with fast life histories tend to be more efficient at transmitting pathogens. Keesing explains, “Animals that live fast, die young, and have early sexual maturity with lots of offspring tend to invest less in their adaptive immune responses. They are often better at transmitting diseases, compared to longer-lived animals with stronger adaptive immunity.”
When biodiversity is lost from ecological communities, long-lived, larger-bodied species tend to disappear first, while smaller-bodied species with fast life histories tend to proliferate. Research has found that mammal hosts of zoonotic viruses are less likely to be species of conservation concern (i.e. they are more common), and that for both mammals and birds, human development tends to increase the abundance of zoonotic host species, bringing people and risky animals closer together.
“When we erode biodiversity, we favor species that are more likely to be zoonotic hosts, increasing our risk of spillover events,” Ostfeld notes. Adding that, “Managing this risk will require a better understanding of how things like habitat conversion, climate change, and overharvesting affect zoonotic hosts, and how restoring biodiversity to degraded areas might reduce their abundance.”
To predict and prevent spillover, Keesing and Ostfeld highlight the need to focus on host attributes associated with disease transmission rather than continuing to debate the prime importance of one taxon or another. Ostfeld explains, “We should stop assuming that there is a single animal source for each emerging pathogen. The pathogens that jump from animals to people tend to be found in many animal species, not just one. They’re jumpers, after all, and they typically move between species readily.”
Disentangling the characteristics of effective zoonotic hosts – such as their immune strategies, resilience to disturbance, and habitat preferences – is key to protecting public health. Forecasting the locations where these species thrive, and where pathogen transmission and emergence are likely, can guide targeted interventions.
Keesing notes, “Restoration of biodiversity is an important frontier in the management of zoonotic disease risk. Those pathogens that do spill over to infect humans–zoonotic pathogens–often proliferate as a result of human impacts.” Concluding, “As we rebuild our communities after COVID-19, we need to have firmly in mind that one of our best strategies to prevent future pandemics is to protect, preserve, and restore biodiversity.”
Reference: “Impacts of biodiversity and biodiversity loss on zoonotic diseases” by Felicia Keesing and Richard S. Ostfeld, 5 April 2021, Proceedings of National Academy of Sciences. DOI: 10.1073/pnas.2023540118
This research was supported by a National Science Foundation Grant OPUS 1948419 to Keesing.
Cary Institute of Ecosystem Studies is an independent nonprofit center for environmental research. Since 1983, our scientists have been investigating the complex interactions that govern the natural world and the impacts of climate change on these systems. Our findings lead to more effective management and policy actions and increased environmental literacy. Staff are global experts in the ecology of: cities, disease, forests, and freshwater.
Intervenção artística com desenhos de Joseca Yanomami marca a entrega da petição #ForaGarimpoForaCovid a deputados federais e demais autoridades
Por Oswaldo Braga de Souza*
Poesia e política se somaram no encerramento da campanha #ForaGarimpoForaCovid, liderada pelo Fórum de Lideranças Yanomami e Ye’kwana. Para marcar o fim do capítulo mais recente da luta dos indígenas pela expulsão dos mais de 20 mil garimpeiros de suas terras, os coordenadores da Hutukara Associação Yanomami, Dário Kopenawa e Maurício Ye’kwana, entregaram a representantes do Parlamento brasileiro um abaixo-assinado com quase 440 mil assinaturas de apoiadores em todo o mundo.
À noite, em uma intervenção artística inédita, frases em defesa da floresta e desenhos dos xapiri, os espíritos Yanomami, foram projetados na fachada do Congresso por quase duas horas. As ilustrações são do artista Joseca Yanomami e o texto é do líder indigena Davi Kopenawa.
*Consulte a ficha ténica abaixo
Os xapiri são os espíritos que auxiliam os xamãs em seu árduo trabalho de manter o equilíbrio do mundo e o próprio céu em seu lugar. São figuras centrais na cosmologia Yanomami, e se materializam para os xamãs como os espíritos dos animais, das árvores, das águas, de tudo o que existe na Urihi a, a “terra-floresta”, conceito Yanomami que engloba a floresta e todos os seus habitantes físicos e metafísicos.
O objetivo da campanha é exigir a retirada de milhares de garimpeiros da Terra Indígena (TI) Yanomami (AM/RR) para impedir a disseminação da Covid-19, a contaminação do solo e dos rios e o degradação florestal. O garimpo está espalhando a doença na área, segundo relatório produzido pelo Fórum de Lideranças Yanomami e Ye’kwana e a Rede Pró-Yanomami e Ye’kwana, também encaminhado aos parlamentares.
Mais de um terço das 26,7 mil pessoas que moram na TI foi exposto ao novo coronavírus e o número de casos confirmados saltou de 335 para 1,2 mil, entre agosto e outubro, um aumento de mais de 250%, ainda conforme o levantamento. Apesar disso, menos de 5% da população foi testada.
A petição foi apresentada numa reunião virtual das frentes parlamentares de defesa dos direitos indígenas e ambientalista, com a presença de deputados federais e senadores. O evento foi organizado para discutir o aumento do garimpo e seus impactos nos territórios yanomami, kayapó e munduruku e contou com a participação de parlamentares, líderes indígenas, procuradores da República, pesquisadores e organizações da sociedade civil.
“Chega de sofrer. Já perdemos muitos parentes”
“Chega de sofrer. Já perdemos muitos parentes. Temos xawara [Covid-19]. Os Yanomami estão contaminados pelo garimpo, nossos rios estão poluídos, contaminados com mercúrio”, afirmou Dário Kopenawa. “Queremos que as autoridades tomem providências. Não queremos mais perder nossos velhos, nossos filhos, não queremos mais chorar. Queremos que as autoridades retirem os garimpeiros o mais rápido possível”, continuou.
“Ao longo desses meses, alertamos as autoridades sobre os impactos que sofremos com os garimpeiros que invadem nossa terra”, diz carta lida por Maurício Ye’kwana na reunião. “Mas nosso recado não foi escutado. Os garimpeiros continuam entrando em nossas casas”, seguiu a liderança.
“Um absurdo dizer que defender Terras Indígenas, defender indígena, se manifestar contra os garimpos em Terras Indígenas é uma questão ideológica, de esquerda ou de comunista. Isso é lei. Isso é direito. Está na nossa Constituição”, afirmou a deputada federal e coordenadora da Frente Parlamentar em Defesa dos Direitos dos Povos Indígenas, Joênia Wapichana (Rede-RR). “Essa petição é mais uma forma de reivindicar nada além do que está na Constituição, que é o direito à proteção à vida, o direito à terra, o direito de ter sua terra sem invasões”, afirmou.
Joênia lembrou que a TI Yanomami abriga grupos indígenas isolados, os Moxihatëtëa, que correm risco de desaparecer caso sejam contatados por não indígenas e contaminados por doenças para os quais não têm defesas imunológicas, como gripe e sarampo. A Covid-19 representa um risco ainda maior para essas comunidades em virtude da dificuldade para atendimento e transporte de doentes em regiões remotas e de difícil acesso, como é o caso da área.
Estímulo ao garimpo
O governo Bolsonaro não só não fez nada para retirar os invasores do território yanomami como estimula abertamente o garimpo em TIs, o que é ilegal. O Planalto enviou um Projeto de Lei ao Congresso, em fevereiro, para regulamentar a atividade nessas áreas, além da mineração industrial e a construção de hidrelétricas. O resultado é o aumento da presença garimpeira, dos conflitos envolvendo sua atividade e do desmatamento nos territórios indígenas em geral, nos últimos dois anos.
“A responsabilidade pelo aumento das invasões está diretamente relacionada à complacência deste governo com a criminalidade, a desestruturação dos órgãos de fiscalização e controle e com a omissão em cumprir decisões judiciais”, criticou, na reunião, a advogada do ISA Juliana de Paula Batista. Ela lembrou que a Justiça Federal determinou que a União apresente um plano de retirada dos garimpeiros da TI Yanomami e o STF ordenou a implantação de barreiras sanitárias na área. Nenhuma das duas decisões foi cumprida.
“É fundamental que as casas legislativas estejam comprometidas com a defesa e proteção dos povos indígenas e em assegurar seus direitos, previstos na Constituição”, concluiu.
Em agosto, o Supremo Tribunal Federal (STF) confirmou uma liminar do ministro Luís Roberto Barroso que obriga o governo a agir para conter a escalada da crise de saúde entre os povos indígenas. A única medida incluída no pedido original da ação e não atendida foi justamente a retirada imediata de invasores de sete TIs, entre elas a Yanomami. Barroso criou um grupo de trabalho para acompanhar as providências da administração federal. O ministro determinou que fossem refeitos os planos oficiais de enfrentamento geral da Covid-19 e de instalação de barreiras sanitárias nas TIs. O movimento indígena segue aguardando uma medida mais enérgica para forçar o governo a retirar os invasores das sete áreas.
Munduruku
“Querem legalizar o garimpo, como se isso fosse resolver o problema da população indígena. Isso só vai piorar a situação. O garimpo traz prostituição e drogas para o territorio”, criticou, na reunião do dia 03 de dezembro, Alessandra Korap Munduruku, líder indígena ameaçada de morte pelas denúncias contra os invasores da TI Sawré Muybu, no sudoeste do Pará. Em outubro, ela ganhou o prêmio Robert F. Kennedy de Direitos Humanos, dos EUA.
“A maioria dos indígenas tem de beber água suja do rio. Todas as nascentes estão sendo desmatadas para uso dos garimpos. Vemos máquinas, dragas cavando o fundo do rio, enquanto os indígenas têm de comer o peixe. Teremos de comprar peixes na cidade para levar para as aldeias? Teremos de comprar água na cidade para levar para as aldeias. O que será dos indígenas depois de legalizarem o garimpo?”, questionou Alessandra Munduruku.
Ainda na reunião, o WWF-Brasil apresentou parte dos resultados de um estudo realizado pela organização em conjunto com a Fundação Oswaldo Cruz (Fiocruz) sobre contaminação do mercúrio em três aldeias da TI Sawré Muybu.
Os dados revelam uma situação dramática. O mercúrio foi detectado em 100% da população e, em 60% dela, o nível da substância não foi considerado seguro. Em 100% das amostras de peixes, havia resquícios do elemento químico. Em algumas, havia 18 vezes mais mercúrio do que o máximo tolerado pelos critérios da agência ambiental dos EUA.
Em quatro de cada 10 crianças foram identificadas altas concentrações de mercúrio. Em 16% das crianças, foram detectados problemas de neurodesenvolvimento. “As crianças estão perdendo a saúde. Isso é um crime gravíssimo contra as crianças indígenas! Quando Alesssandra Munduruku fala em genocídio, ela não está exagerando”, afirmou Bruno Taitson, representante do WWF-Brasil.
* Com informações de Ester Cezar
Ficha técnica:
O SOPRO DOS XAPIRI XAPIRI PË NË MARI 2020 animação em três canais projetada no Palácio do Congresso Nacional 01:39”
Desenhos: Joseca Yanomami
Frases: Davi Kopenawa Yanomami
Cantos: Ehuana Yaiara Yanomami, Levi Malamahi Alaopeteri Yanomami, Tafarel Yanomami – captados por Marcos Wesley de Oliveira na aldeia Watorikɨ. Outros registros sonoros captados por Gustavo Fioravante, em Watorikɨ.
Realização: Fórum de Lideranças Yanomami e Ye’kwana e Instituto Socioambiental
Apoio: Hutukara Associação Yanomami
Criação, direção e roteiro: Gisela Motta, Isabella Guimarães e Mariana Lacerda [Barreira Y.]
Animação e montagem: JR Muniz e Leandro Mendes – Vigas
Video mapping em Brasília, direção técnica: Alexis Anastasiou
Equipamentos: Visual Farm / Paralax
Captação em Brasília: Bruna Carolli, Cleber Machado, Daniel Basil, Ester Cezar, Guto Martins, Paulo Comar, Victor Ekstrom
Edição e áudio: Cauê Ito
Agradecimentos: aos povos Yanomami e Ye’kwana, Ana Teixeira, André Komatsu, Bruno Rangel, Carlo Zacquini, Claudia Andujar, Gui Conti, Irina Theophilo, Joana Amador, Juliana Calheiros, Kauê Lima, Laura Andreato, Lucas Bambozzi, Peter Pál Pelbart, Pio Figueiroa, Rede Pró-Yanomami e Ye’kwana, Rivane Neuenschwander, Tuíra Kopenawa Yanomami, Vitor Osório
Nurit Bensusan, assessora do ISA e especialista em biodiversidade
É interessante pensar que o fim do mundo talvez seja um longo processo: nada de meteoro ou de explosões atômicas. Uma pandemia aqui, um evento climático extremo ali, menos comida, mais uma pandemia, secas catastróficas, menos comida ainda, mais uma pandemia, sede, fome, guerras, mais secas, mais pandemias, mais inundações… Enfim, a consolidação de um planeta hostil à nossa espécie.
Em relatório recém-lançado, a Plataforma Intergovernamental de Biodiversidade e Serviços Ecossistêmicos (IBPES, na sigla em inglês) chama o período em que estamos entrando, com a pandemia de Covid-19, de a “Era das Pandemias”. Diante dos dados expostos pelo relatório, o nome vem bem a calhar. Alguns deles, para dar o tom:- Estima-se que haja 1,7 milhões de vírus que ainda não foram descritos em mamíferos e aves. Desses, entre 540 mil e 850 mil teriam a capacidade de infectar humanos.
– Os mais importantes reservatórios de patógenos com potencial pandêmico são os mamíferos (em particular morcegos, roedores e primatas) e algumas aves, em especial as aquáticas, assim como os animais criados para a produção de proteína animal, como porcos, galinhas, camelos, etc.
– O risco de pandemias está aumentando rapidamente com a emergência de mais de cinco doenças novas em humanos a cada ano. Qualquer uma dessas tem potencial para se espalhar e se tornar uma nova pandemia.
– O risco é aumentado exponencialmente pelas modificações antropogênicas, tais como a perda de biodiversidade, a simplificação das paisagens e a degradação de ecossistemas.
No quesito “modificações antropogênicas” que aumentam exponencialmente o risco das pandemias, é que estão as ideias, tão bem implementadas por aqui, para apressar o fim do mundo. A aceleração do desmatamento e da degradação do ambiente, o descompromisso com o combate à crise climática e o desrespeito à diversidade social, cultural e de formas de estar no mundo têm sido nosso cotidiano.
Não há dúvida alguma que o atual governo brasileiro parece ter pressa para chegar ao apocalipse. A situação geral do planeta, porém, não é muito diferente. Ao invés de uma janela de oportunidades, a pandemia revelou-se um espelho quebrado cujo reflexo tememos ver. Uma das estranhas consequências da situação é que o inaceitável mundo em que vivíamos, transbordante de desigualdades, racismo, ansiedade, depressão e violência, parece ter se tornado não apenas tolerável mas até mesmo desejável. Não apenas não enxergamos outras possibilidades de futuro, como ansiamos por voltar a nossa vida pregressa.
Pulsão de morte ou confiança na tecnologia?
Curiosamente, o relatório do IBPES não surtiu grandes efeitos. Assim como os números crescentes de mortes por Covid-19, de hectares desmatados na Amazônia ou queimados no Pantanal, de toneladas de carbono lançadas na atmosfera ou de plástico no mar. Trata-se, será, de uma pulsão de morte da nossa espécie ou uma confiança excessiva nas soluções tecnológicas?
Além das ideias para apressar o fim do mundo que já conhecemos, algumas novidades têm chamado atenção. Uma delas é a mortandade de elefantes em Botswana, o lugar com a terceira maior população de elefantes africanos. Nos primeiros meses deste ano, 330 elefantes morreram envenenados por fontes de água contaminadas por cianobactérias, provavelmente uma consequência das mudanças climáticas.
Outra é a situação das praias de Kamtchaka, localizadas na costa leste da Rússia, local que faz a festa dos surfistas. Ali, no começo de setembro, as pessoas começaram a apresentar queimaduras na pele, vômitos e dificuldade para respirar. De lá para cá, milhares de animais marinhos já morreram.
As hipóteses ligadas à poluição não foram comprovadas, apesar dos níveis de elementos derivados do petróleo, de fosfato e de mercúrio estarem muito acima do aceitável. As pesquisas conduziram à conclusão que se trata de uma proliferação exacerbada de algas, que emitem toxinas e exaurem o oxigênio da água, causada pelas mudanças climáticas.
Ambiente hostil e egoísmo
Além de transformarmos o planeta num ambiente hostil para nós mesmos, estamos contribuindo para o rápido desaparecimento da biodiversidade. Se o apelo ético da responsabilidade de carregar tantas mortes nas costas não move a nossa espécie, o egoísmo deveria fazê-lo. É justamente a complexidade da paisagem, composta por várias espécies em múltiplas relações, que garante a contenção das zoonoses, impedindo que essas doenças que vêm dos animais silvestres cheguem aos humanos.
Essas moléstias são muitas e se tornam mais comuns à medida que vamos destruindo os ecossistemas e degradando os serviços que eles nos oferecem. Vale lembrar que a maioria das enfermidades humanas infecciosas que surgiram nas décadas recentes teve origem na vida silvestre e 65% de todos os patógenos humanos descobertos, desde 1980, foram identificados como vírus zoonóticos. Entre elas, estão a Zyka, a Febre do Rift Valley, a gripe aviária, a H1N1 e muitas outras.
A esse cenário, já bastante preocupante, soma-se o descongelamento acelerado do Ártico e do Permafrost, área de milhares de quilômetros quadrados de solos congelados que circunda o Ártico. Esse fenômeno começa a causar uma injeção de mais gases de efeito estufa na atmosfera, o encontro de animais que não conviviam antes e a possibilidade da emergência de novos e velhos patógenos, presentes nos restos mortais de espécies de outros tempos, como o mamute, ou de pessoas de outros séculos, como as vítimas de uma epidemia de varíola do fim do século XIX. Tudo isso aponta para um maior risco de novas doenças e de pandemias.
Mundo sem nós
Alguns livros e filmes já tentaram delinear como seria o mundo sem nós. Aparentemente, a Terra se recuperaria bem do estrago que estamos fazendo e talvez nem demorasse muitos milhares de anos para isso. A única coisa que sobraria, uma lembrança de nossa passagem pelo cosmos, seriam os plastiglomeratos, um material que pode ser descrito como um fragmento rochoso que reúne grãos de areia, detritos plásticos e materiais orgânicos, como conchas, partes de corais e madeiras, amalgamados por algo que já foi um plástico derretido. Sua origem remete a fogos causados por humanos, em geral para queimar lixo. Foram encontrados primeiro na praia Kamilo, no Havaí, em 2014, mas de lá para cá já foram identificadas em Bali, na Califórnia, na ilha de Madeira e em Ontário, no Canadá.
O relatório do IBPES aponta que ainda podemos escapar da Era das Pandemias, pois temos acumulado bastante conhecimento para traçar caminhos que nos permitam prever e evitar novas crises sanitárias. Isso, segundo o relatório, inclui localizar possíveis origens geográficas de novas pandemias, identificar hospedeiros- chave e patógenos com mais probabilidade de emergir e demonstrar como as mudanças ambientais e socioeconômicas estão relacionadas com a emergência de doenças. O relatório também traz um conjunto de mecanismos para tornar isso possível. Alguns estão ligados a um reforço de instrumentos multilaterais, como o estabelecimento de um conselho intergovernamental de prevenção de pandemias que, além de promover a cooperação entre governos, trabalharia com as três convenções da Eco -92 (Mudanças Climáticas, Biodiversidade e Combate à Desertificação), para desenvolver uma abordagem chamada de One Heath (uma saúde, em inglês). Trata-se de pensar uma abordagem que conecte saúde humana, saúde animal e questões ambientais.
Há várias outras recomendações tanto ligadas ao financiamento de atividades que degradam o meio ambiente como relacionadas com o consumo humano. O inusitado é que nada disso é novo. Sabemos de tudo isso e sabemos há muito tempo. Sabemos que essa relação predatória que cultivamos com a natureza tem um preço e que, fatalmente, ele seria cobrado.
A conclusão do relatório é que as transformações necessárias a evitar pandemias podem parecer de difícil implementação, caras e de impacto incerto. A isso, os autores contrapõem os custos de enfrentar uma pandemia e afirmam que esse caminho trará benefícios para a saúde, a biodiversidade e as nossas economias. Apesar de não ser algo novo, o caminho para evitar o fim do mundo é apontado, descrito e sinalizado. Resta saber se vamos, como sempre, fazer mais do mesmo, ou se vamos agarrar o touro pelos chifres, sobreviver, viver e deixar viver, aqui e agora, neste planeta.
Os Huni Kuin do Acre e do Leste da floresta amazônica peruana compartilham com muitos outros povos indígenas da região uma filosofia de vida que poderíamos chamar de ecosófica[ii] e que atribui a maior parte das doenças ao fato de comermos animais. As pessoas adoecem porque a caça e os peixes, mas também algumas plantas que consumimos e outros seres que agredimos ou com os quais interagimos, se vingam e mandam seu nisun, dor de cabeça e tonteira que pode resultar em doença e morte.
O xamanismo e o uso de plantas psicotrópicas, como tabaco e cipó, servem para descobrir a ação destes agentes invisíveis e de contra-efetuar, através do canto, do sopro, de perfumes e plantas medicinais, o movimento de captura do espírito da vítima por parte dos duplos dos animais mortos. O universo da floresta é, assim, habitado por uma multiplicidade de espécies que são sujeitos e negociam seu direito ao espaço e à própria vida. Neste universo a cosmopolítica dos humanos consiste em matar somente o necessário e em negociar com os donos das espécies ou com os próprios duplos dos animais. Tem-se a aguda (con)ciência de que para viver é preciso matar e de que toda ação, toda predação, desencadeia uma contra-predação.
Quando a quarentena foi anunciada no Brasil, meu amigo, o líder de canto do cipó, Ibã Sales Huni Kuin, se despediu por telefone: “Vamos nos retirar na floresta, vamos ficar quietos e não vamos deixar mais ninguém entrar, porque tudo isso é nisun”. Nada sabia, ainda, sobre as hipóteses de causa do novo vírus, que apontam de fato para o nisun de outras florestas. E apesar do nome dado aos Huni Kuin pelos seus inimigos ser Kaxinawa, povo morcego, não consomem estes animais porque os consideram seres que possuem yuxin, o poder de transformar a forma. O que pode um vírus, no entanto, Ibãe seus parentes indígenas sabem muito bem. Pois vírus importados, como a influenza e a varíola, causaram, no passado, mais mortes na sua população do que as guerras travadas contra eles na época de invasão de suas terras.
A narrativa científica mais aceita do momento, pelo que conseguimos deduzir da literatura disponível e de livre acesso durante a pandemia, atribui o novo corona à passagem do vírus de uma espécie de morcego (horseshoe bat) que vive nas florestas Chinesas para o ser humano[iii]. A hipótese se baseia no sequenciamento do genoma do vírus do COVID-19 e suas grandes semelhanças com um coronavírus presente nestes morcegos. Outro animal que hospeda um vírus geneticamente muito similar é o pangolim, um tipo de tatu asiático muito apreciado por grande parte da população chinesa como iguaria e remédio. Uma das hipóteses é que este poderia ter sido o hospedeiro intermediário do vírus entre o morcego e o humano[iv]; as últimas pesquisas, no entanto, afirmam que o vírus do morcego é mais próximo do COVID-19 do que aquele encontrado nos pangolins. Ambos os animais são consumidos na China e em outros países asiáticos. Os primeiros casos do novo corona vírus foram detectados em um grande mercado de Wuhan na China, onde se vende animais selváticos vivos, entre os quais morcegos e muitos pangolins, apesar de sua captura e comercialização serem proibidas.
O ‘zoonotic spillover’ de viroses que convivem com espécies selváticas, sem causar-lhes mal, para seres humanos, onde causam assustadoras pandemias, não começou nem terminará com o novo coronavírus. Outras epidemias recentes como a malária, a aids e a febre amarela foram resultado do spillover entre floresta e cidade.. O problema é especialmente interessante para a antropologia em geral e a etnologia em particular, porque nossa disciplina se interessou desde o começo pelas complexas relações entre humanos e animais, Natureza e Cultura, cidade e floresta. Agentes patogênicos, que convivem de forma simbiótica com seus hospedeiros animais, podem representar diferentes graus de perigo para os humanos, dependendo da cultura ou sociedade específica em questão. As regras de dieta e de negociação em torno da caça apontam para um saber acumulado, por parte dos povos da floresta, do potencial patogênico dos animais. Estes possuem seus próprios hábitos e habitats que precisam ser respeitados se quiserem que a caça não se vire contra o caçador.
A novidade destas novas epidemias, argumentam epidemiólogos e biólogos, consiste na rapidez com que o vírus viaja e se multiplica no meio humano, por causa da grande aglomeração e circulação de seres da mesma espécie nas cidades e nas regiões transitórias entre as cidades e as florestas. A realidade relacional contemporânea de intensa circulação de pessoas, mercadorias e animais é o cronótopo perfeito para a disseminação desta nova ameaça mundial. Este cronótopo vai acompanhado de uma redução cada vez maior das áreas de floresta onde os hospedeiros dos agentes patogênicos conviviam com os vírus de modo que estes não lhes causavam doenças, nem o transmitiam para os seres humanos.
Em entrevista dada à CNN (20/03/2020), intitulada “the bats are not to blame”, “não são os morcegos os culpados”, Andrew Cunningham, Professor da Zoological Society de Londres, afirma que: “a causa do “zoonotic spillover”, ou o transfer de morcegos ou outras espécies selvagens, é quase sempre o comportamento humano”. O biólogo aponta algumas características interessantes dos morcegos que nos ajudam a entender sua importância e seus perigos para os humanos. Os morcegos são os únicos mamíferos que voam, o que faz com que eles possam cruzar grandes distâncias e disseminar muitos agentes patogênicos. Mas eles também são os polinizadores mais importantes da floresta tropical, e muitas espécies dependem exclusivamente dos morcegos para sobreviver. No mito de origem das plantas cultivadas dos Huni Kuin, foi um quatipuru transformado em homem que ensinou o cultivo das plantas aos humanos. O mesmo quatipuru, no entanto, sabia se transformar também em morcego. Os morcegos, como os humanos, gostam de viver em grandes grupos, o que facilita a disseminação de sementes, pólen e vírus. O voo do morcego requer muita energia, afirma Cunningham, o que produz altas temperaturas no animal, temperaturas que no ser humano significariam febre. É por esta razão que quando passa para o humano, o vírus é tão virulento. Outro elemento interessante é que, como os humanos, os morcegos sentem stress. Quando percebem seu habitat danificado pelo desflorestamento ou quando amontoados vivos em grandes feiras, juntos com outros animais, para serem sacrificados, o aumento do stress pressiona seu sistema imunológico e pode fazer com que um vírus latente se torne manifesto e mais contagioso.
Não é o fato dos humanos comerem caça a causa das epidemias. As epidemias são o resultado do desmatamento e da extinção dos animais que antes eram seus hospedeiros simbióticos. As epidemias são também o resultado de uma relação extrativista das grandes cidades com as florestas. Elas surgem nas franjas das florestas ameaçadas, nos interstícios da fricção interespécie e de lá são rapidamente transportadas para o mundo inteiro através de caminhões, barcos e aviões. E não é somente a caça cujo stress causa pandemias, outros animais também sofrem e causam doenças. Estes são prisioneiros de outra área intersticial entre a floresta e a cidade, a área rural do grande agronegócio alimentício, notória para o surgimento de novas gripes virulentas que podem virar pandemias. É nas grandes criações industrializadas de galinhas e porcos confinados que surgiram há alguns anos a chamada ‘gripe suína’ e outras que foram um prenúncio do vírus que observamos hoje.
A grande rede que conecta humanos e não humanos é a causa e a solução para o problema. Vivemos, em escala planetária, um problema em comum; sua solução também terá de ser comum. Virá da troca interdisciplinar e internacional de informações, mas virá sobretudo do que podemos aprender de outras tradições de pensamento que não se construíram sobre a separação dualista entre natureza e cultura. A substituição de ontologias relacionais pela oposição entre “sujeito” e “objeto”, resultando numa ontologia dualista, possibilitou a empresa modernista e capitalista e sua invenção de uma máquina de conquista do mundo, capturando em suas engrenagens até as mais resistentes minorias humanas e não humanas, que tentam sobreviver em suas margens.
As ontologias dessas minorias, no entanto, falam uma linguagem que contém conhecimentos vitais para o planeta hoje e que precisamos traduzir, com urgência, para a linguagem da ciência. Assim, na sua videoconferência para o Colóquio “Os mil nomes de Gaia” (2014), Donna Haraway apelou para uma consciência renovada de como todos os seres, incluindo os humanos, são compostos de outros seres e emaranhados numa malha densa de devir-com. Em vez de inter-relacionalidade, estamos lidando com intra-relacionalidade; somos entidades compostas de relações, entrecruzadas por outras agências e habitadas por subjetividades diferentes. Somos múltiplos e divíduos em vez de indivíduos; somos fractais. Somos habitados por bactérias e vírus saudáveis e nocivos que travam batalhas intermináveis. Essas novas descobertas cientificas se aproximam cada vez mais do que as filosofias ameríndias há tempos tentam nos ensinar. “A noção de uma entidade somada ao meio ambiente não pode mais ser pensada […]. Temos o que os biólogos chamam de holobiontes, a coleção de entidades tomadas em conjunto na sua relacionalidade que constroem uma entidade boa o suficiente para sobreviver o dia”[v].
A reação em rede planetária à nova pandemia, que se espalha pelo ar em gotículas invisíveis, transforma nossos corpos em campos de batalha invisíveis onde é, às vezes, a própria autodefesa, a reação excessiva do nosso sistema imunológico aos invasores, que mata as células vitais e acaba destruindo nossos órgãos. Ou seja, quando o sistema está muito estressado ele se auto-consome. Não é o fato de comermos porcos, morcegos, galinhas ou pandolins que causa epidemias mundiais, mas o modo como a civilização mundial, que se alimenta do crescimento sem fim das cidades sobre as florestas, as árvores e seus habitantes, parou de escutar a revolta, não das coisas, mais dos animais, das plantas e de Gaia. Ou como diria Ailton Krenak, as pessoas foram alienadas e arrancadas da terra que é viva e com a qual é preciso dialogar, conviver[vi].
__________
[i] Professora Titular de Antropologia na Universidade Federal do Rio de Janeiro, docente e pesquisadora no Programa de Pós Graduação em Sociologia e Antropologia (PPGSA/UFRJ).
[ii] Termo usado por Kay Arhem em “Ecosofia Makuna”, 1993, In La Selva Humanizada: Ecologia Alternativa em el Trópico Húmedo Colombiano. Bogotá: Instituto Colombiano de Antropología, pp. 109-126.
[iii] Wallace, Rob; Liebman, Alex; Chaves, Luis Fernando; Wallace, Rodrick, April 1, 2020, “COVID-19 and Circuits of capital”, in Monthly Review, New York.
[iv] Tommy Tsan-Yuk Lam, Marcus Ho-Hin Shum, Hua-Chen Zhu, Yi-Gang Tong, Xue-Bing Ni, Yun-Shi Liao, Wei Wei, William Yiu-Man Cheung, Wen-Juan Li, Lian-Feng Li, Gabriel M. Leung, Edward C. Holmes, Yan-Ling Hu & Yi Guan. 28.03.2020,“Identifying SARS-CoV-2 related corona viruses in Malayan pangolins”, In Nature, www.nature.com.
“O hospital em que eu trabalho, em Paris, está cheio de pacientes infectados pelo coronavírus. Vai se tornar uma referência para a doença. Só hoje eu internei 10 (cinco deles com menos de 50 anos).
Esta semana e na próxima estaremos no pico da infecção. O governo francês está pagando hotéis próximos aos hospitais para que os médicos e demais trabalhadores da saúde não contaminem suas famílias. Eu estou num hotel confortável, a três minutos de carro do hospital.
Os restaurantes da região têm enviado refeições de graça, no almoço e no jantar, para toda a equipe de plantão. Comemos por turnos, juntos: médicos, enfermeiros e soignants – técnicos, maqueiros, secretárias e seguranças.
Aqui na França, muita gente vai morrer. Já estamos enviando pacientes para a Suíça, Alemanha e Luxemburgo, pois faltam leitos de UTI. No nosso hospital há muitos jovens infectados.
Todo mundo aqui está trabalhando a todo vapor. Foram canceladas todas as férias.
Até o fim da semana teremos 400 pacientes POR DIA intubados na Île-de-France (a província onde fica Paris). É muita gente! Nosso hospital tem 120 pacientes com Covid-19. A previsão é que, daqui a 15 dias, os 692 leitos sejam ocupados por pacientes infectados pelo novo coronavírus.
Todos os outros casos (infartos, AVCs, fraturas etc) são encaminhados a clínicas privadas. Cidade vazia. Polícia e exército nas ruas, multando quem não tem permissão de trafegar. Peguei a minha autorização hoje no hospital.
Dia 2
Mais um dia de confinamento em Île-de-France. Talvez o dia mais difícil de todos na minha vida como médico.
No texto anterior eu expliquei que a previsão era que se esgotassem todos os respiradores da província até o fim dessa semana, com uma previsão de 400 pacientes por dia.
Previsão errada.
Hoje praticamente todos os respiradores foram tomados. Em nosso hospital, por volta das 15h30, já não tínhamos como ventilar pacientes que precisavam ser intubados. Conclusão: desabou um desespero em nossas cabeças porque sabíamos que teríamos que escolher a quem salvar e a quem deixar. E foi isso o que automaticamente fizemos. Fui julgado por um grande amigo, de fora da área da saúde, quando lhe contei isso. Mas era isso ou deixar a peteca cair e não salvar ninguém! Ou tomar a decisão errada de salvar quem não teria chance.
Como na Itália (e acredito que na Espanha também), somos obrigados a decidir. O regulador do plantão telefonou para o que chamamos de Proteção Civil e o exército se encarregará de distribuir tendas com respiradores em volta dos hospitais estratégicos localizados ao redor de Paris. Medida de medicina de guerra (e foi este mesmo o termo utilizado aqui). Isso já acontece na Alsácia (leste da França, fronteira com a Alemanha).
Vi colegas com lágrimas nos olhos. Minha chefe ligava de hora em hora para saber o fluxo de pacientes no Pronto-Socorro. Sim, aqui, geralmente, a chefia é mais que um posto. E a chefe se mostrou uma verdadeira líder, compadecendo-se conosco pela situação.
Os mais graves eram encaminhados a unidades de internação Covid-19 para morrer com dignidade. E a cada 15 minutos, em média, recebíamos ligações da enfermagem dessas unidades confirmando que tal ou tal paciente não deveria ser reanimado. Todos eles com máscara facial de oxigênio a 15L/min e dessaturando.
A conduta era sedar e oferecer conforto e dignidade. Fomos tomados por uma sensação de impotência frente a uma doença nova. Esta é a minha primeira pandemia (e de quase todos aqui). Os rostos dos que atendemos à tarde passam por nossos pensamentos. Vimos, um por um, eles descansarem.
Sinto um misto de alegria por participar de um salvamento coordenado e, ao mesmo tempo, uma tristeza imensa por saber que, em muitos casos, estávamos e ainda estamos perdendo a batalha para esse vírus.
Às 20h se ouve o barulho de aplausos nas janelas. Mas só quem estava no front sabia o que estava acontecendo. As mortes se seguiam. O telefone não parava de tocar. A desesperança e as lágrimas eram visíveis nos olhos de todos. Só quem não participava eram os colegas já contaminados pelo vírus, pois estavam fora de combate. Sim, tenho colegas em casa esperando se recuperar pra voltar. Ou não.
No meio do massacre, a solidariedade era sentida como um mexer numa ferida aberta. A realidade sangrava aos nossos olhos. Os pediatras suspenderam o atendimento, uma vez que as crianças têm sido, quase na sua totalidade, poupadas da infecção. E esses pediatras se dispuseram a gerenciar as UTIs recém-criadas em várias unidades no hospital.
Parei no meio do dia, por alguns segundos, para mandar mensagens a familiares e pessoas mais próximas. Tanto pra desabafar como para prevenir de que o pior está por vir.
Os restaurantes continuam a mandar comida de graça para que não percamos tempo em escolher e telefonar. Não falta comida, nem máscaras N-95 (aqui chamadas de Fpp2), nem oxigênio. Nem falta vontade de exercer nossa sagrada vocação de salvar vidas. Mas o avanço da doença está mais rápido que a nossa capacidade de responder à altura.
Nunca me senti tão médico quanto hoje. E também mais ser humano. A experiência nos deixa saber, numa situação dessas, quem vai partir e quem vai lutar por três semanas (esse tem sido o tempo médio) intubado, pronado, sob diálise, para ressuscitar e enfrentar um longo caminho de fisioterapia e reabilitação até uma vida normal.
Agora as pessoas pararam de chegar (são exatamente 04h23). Meu colega, chefe de plantão como eu, foi descansar por volta das 2h30. Daqui a pouco é minha vez. Mas eu disse aos residentes que não consigo descansar. Eles também não. A realidade da medicina já é dura pra quem cai no ritmo de trabalho logo depois da faculdade. Nesse clima de guerra então… Vejo seus olhos assustados e desejo que não tivesse sido assim… Estamos no pico da infecção nesta semana e na próxima. Terei plantões dia sim, dia não – assim como muitos colegas por aqui. É a vida.
Às 10 da manhã a vida recomeça. Inicia com o que chamamos de Reunião Covid-19. Minha chefe reúne todo o pessoal do PS e nos posiciona sobre as últimas notícias, na França e no mundo, quanto à pandemia. Tomamos decisões, discutimos protocolos… e a guerra continua.
Uma enfermeira liga perguntando se pode quebrar o protocolo e deixar uma família entrar no quarto para se despedir do familiar (um pai, marido, avô). Não autorizo. Pela proteção de todos. Desligo o telefone. Lágrimas caem pelo meu rosto. Vou deitar e agradeço a Deus por estar vivo.
Recado aos brasileiros
Vocês, brasileiros, especialmente idosos, terão de ficar em casa por pelo menos dois meses, se quiserem viver. É que o pico aí no Brasil será daqui a um mês e o vírus é mais ativo em temperaturas baixas. Na minha opinião, isso vai se arrastar por aí se não forem respeitadas as medidas de confinamento.
Summary of the article: Strong coronavirus measures today should only last a few weeks, there shouldn’t be a big peak of infections afterwards, and it can all be done for a reasonable cost to society, saving millions of lives along the way. If we don’t take these measures, tens of millions will be infected, many will die, along with anybody else that requires intensive care, because the healthcare system will have collapsed.
Within a week, countries around the world have gone from: “This coronavirus thing is not a big deal” to declaring the state of emergency. Yet many countries are still not doing much. Why?
Every country is asking the same question: How should we respond? The answer is not obvious to them.
Some countries, like France, Spain or Philippines, have since ordered heavy lockdowns. Others, like the US, UK, or Switzerland, have dragged their feet, hesitantly venturing into social distancing measures.
Here’s what we’re going to cover today, again with lots of charts, data and models with plenty of sources:
What’s the current situation?
What options do we have?
What’s the one thing that matters now: Time
What does a good coronavirus strategy look like?
How should we think about the economic and social impacts?
When you’re done reading the article, this is what you’ll take away:
Our healthcare system is already collapsing. Countries have two options: either they fight it hard now, or they will suffer a massive epidemic. If they choose the epidemic, hundreds of thousands will die. In some countries, millions. And that might not even eliminate further waves of infections. If we fight hard now, we will curb the deaths. We will relieve our healthcare system. We will prepare better. We will learn. The world has never learned as fast about anything, ever. And we need it, because we know so little about this virus. All of this will achieve something critical: Buy Us Time.
If we choose to fight hard, the fight will be sudden, then gradual. We will be locked in for weeks, not months. Then, we will get more and more freedoms back. It might not be back to normal immediately. But it will be close, and eventually back to normal. And we can do all that while considering the rest of the economy too.
Ok, let’s do this.
1. What’s the situation?
Last week, I showed this curve:
It showed coronavirus cases across the world outside of China. We could only discern Italy, Iran and South Korea. So I had to zoom in on the bottom right corner to see the emerging countries. My entire point is that they would soon be joining these 3 cases.
Let’s see what has happened since.
As predicted, the number of cases has exploded in dozens of countries. Here, I was forced to show only countries with over 1,000 cases. A few things to note:
Spain, Germany, France and the US all have more cases than Italy when it ordered the lockdown
An additional 16 countries have more cases today than Hubei when it went under lockdown: Japan, Malaysia, Canada, Portugal, Australia, Czechia, Brazil and Qatar have more than Hubei but below 1,000 cases. Switzerland, Sweden, Norway, Austria, Belgium, Netherlands and Denmark all have above 1,000 cases.
Do you notice something weird about this list of countries? Outside of China and Iran, which have suffered massive, undeniable outbreaks, and Brazil and Malaysia, every single country in this list is among the wealthiest in the world.
Do you think this virus targets rich countries? Or is it more likely that rich countries are better able to identify the virus?
It’s unlikely that poorer countries aren’t touched. Warm and humid weather probablyhelps, but doesn’t prevent an outbreak by itself — otherwise Singapore, Malaysia or Brazil wouldn’t be suffering outbreaks.
The most likely interpretations are that the coronavirus either took longer to reach these countries because they’re less connected, or it’s already there but these countries haven’t been able to invest enough on testing to know.
Either way, if this is true, it means that most countries won’t escape the coronavirus. It’s a matter of time before they see outbreaks and need to take measures.
What measures can different countries take?
2. What Are Our Options?
Since the article last week, the conversation has changed and many countries have taken measures. Here are some of the most illustrative examples:
Measures in Spain and France
In one extreme, we have Spain and France. This is the timeline of measures for Spain:
On Thursday, 3/12, the President dismissed suggestions that the Spanish authorities had been underestimating the health threat. On Friday, they declared the State of Emergency. On Saturday, measures were taken:
People can’t leave home except for key reasons: groceries, work, pharmacy, hospital, bank or insurance company (extreme justification)
Specific ban on taking kids out for a walk or seeing friends or family (except to take care of people who need help, but with hygiene and physical distance measures)
All bars and restaurants closed. Only take-home acceptable.
All entertainment closed: sports, movies, museums, municipal celebrations…
Weddings can’t have guests. Funerals can’t have more than a handful of people.
Mass transit remains open
On Monday, land borders were shut.
Some people see this as a great list of measures. Others put their hands up in the air and cry of despair. This difference is what this article will try to reconcile.
France’s timeline of measures is similar, except they took more time to apply them, and they are more aggressive now. For example, rent, taxes and utilities are suspended for small businesses.
Measures in the US and UK
The US and UK, like countries such as Switzerland, have dragged their feet in implementing measures. Here’s the timeline for the US:
Wednesday 3/11: travel ban.
Friday: National Emergency declared. No social distancing measures
Monday: the government urges the public to avoid restaurants or bars and attend events with more than 10 people. No social distancing measure is actually enforceable. It’s just a suggestion.
Lots of states and cities are taking the initiative and mandating much stricter measures.
The UK has seen a similar set of measures: lots of recommendations, but very few mandates.
These two groups of countries illustrate the two extreme approaches to fight the coronavirus: mitigation and suppression. Let’s understand what they mean.
Option 1: Do Nothing
Before we do that, let’s see what doing nothing would entail for a country like the US:
This fantastic epidemic calculator can help you understand what will happen under different scenarios. I’ve pasted below the graph the key factors that determine the behavior of the virus. Note that infected, in pink, peak in the tens of millions at a certain date. Most variables have been kept from the default. The only material changes are R from 2.2 to 2.4 (corresponds better to currently available information. See at the bottom of the epidemic calculator), fatality rate (4% due to healthcare system collapse. See details below or in the previous article), length of hospital stay (down from 20 to 10 days) and hospitalization rate (down from 20% to 14% based on severe and critical cases. Note the WHO calls out a 20% rate) based on our most recently available gathering of research. Note that these numbers don’t change results much. The only change that matters is the fatality rate.
If we do nothing: Everybody gets infected, the healthcare system gets overwhelmed, the mortality explodes, and ~10 million people die (blue bars). For the back-of-the-envelope numbers: if ~75% of Americans get infected and 4% die, that’s 10 million deaths, or around 25 times the number of US deaths in World War II.
You might wonder: “That sounds like a lot. I’ve heard much less than that!”
So what’s the catch? With all these numbers, it’s easy to get confused. But there’s only two numbers that matter: What share of people will catch the virus and fall sick, and what share of them will die. If only 25% are sick (because the others have the virus but don’t have symptoms so aren’t counted as cases), and the fatality rate is 0.6% instead of 4%, you end up with 500k deaths in the US.
If we don’t do anything, the number of deaths from the coronavirus will probably land between these two numbers. The chasm between these extremes is mostly driven by the fatality rate, so understanding it better is crucial. What really causes the coronavirus deaths?
How Should We Think about the Fatality Rate?
This is the same graph as before, but now looking at hospitalized people instead of infected and dead:
The light blue area is the number of people who would need to go to the hospital, and the darker blue represents those who need to go to the intensive care unit (ICU). You can see that number would peak at above 3 million.
Now compare that to the number of ICU beds we have in the US (50k today, we could double that repurposing other space). That’s the red dotted line.
No, that’s not an error.
That red dotted line is the capacity we have of ICU beds. Everyone above that line would be in critical condition but wouldn’t be able to access the care they need, and would likely die.
This is why people died in droves in Hubei and are now dying in droves in Italy and Iran. The Hubei fatality rate ended up better than it could have been because they built 2 hospitals nearly overnight. Italy and Iran can’t do the same; few, if any, other countries can. We’ll see what ends up happening there.
So why is the fatality rate close to 4%?
If 5% of your cases require intensive care and you can’t provide it, most of those people die. As simple as that.
These numbers only show people dying from coronavirus. But what happens if all your healthcare system is collapsed by coronavirus patients? Others also die from other ailments.
What happens if you have a heart attack but the ambulance takes 50 minutes to come instead of 8 (too many coronavirus cases) and once you arrive, there’s no ICU and no doctor available? You die.
There are 4 million admissions to the ICU in the US every year, and 500k (~13%) of them die. Without ICU beds, that share would likely go much closer to 80%. Even if only 50% died, in a year-long epidemic you go from 500k deaths a year to 2M, so you’re adding 1.5M deaths, just with collateral damage.
If the coronavirus is left to spread, the US healthcare system will collapse, and the deaths will be in the millions, maybe more than 10 million.
The same thinking is true for most countries. The number of ICU beds and ventilators and healthcare workers are usually similar to the US or lower in most countries. Unbridled coronavirus means healthcare system collapse, and that means mass death.
Unbridled coronavirus means healthcare systems collapse, and that means mass death.
By now, I hope it’s pretty clear we should act. The two options that we have are mitigation and suppression. Both of them propose to “flatten the curve”, but they go about it very differently.
Option 2: Mitigation Strategy
Mitigation goes like this: “It’s impossible to prevent the coronavirus now, so let’s just have it run its course, while trying to reduce the peak of infections. Let’s just flatten the curve a little bit to make it more manageable for the healthcare system.”
This chart appears in a very important paper published over the weekend from the Imperial College London. Apparently, it pushed the UK and US governments to change course.
It’s a very similar graph as the previous one. Not the same, but conceptually equivalent. Here, the “Do Nothing” situation is the black curve. Each one of the other curves are what would happen if we implemented tougher and tougher social distancing measures. The blue one shows the toughest social distancing measures: isolating infected people, quarantining people who might be infected, and secluding old people. This blue line is broadly the current UK coronavirus strategy, although for now they’re just suggesting it, not mandating it.
Here, again, the red line is the capacity for ICUs, this time in the UK. Again, that line is very close to the bottom. All that area of the curve on top of that red line represents coronavirus patients who would mostly die because of the lack of ICU resources.
Not only that, but by flattening the curve, the ICUs will collapse for months, increasing collateral damage.
You should be shocked. When you hear: “We’re going to do some mitigation” what they’re really saying is: “We will knowingly overwhelm the healthcare system, driving the fatality rate up by a factor of 10x at least.”
You would imagine this is bad enough. But we’re not done yet. Because one of the key assumptions of this strategy is what’s called “Herd Immunity”.
Herd Immunity and Virus Mutation
The idea is that all the people who are infected and then recover are now immune to the virus. This is at the core of this strategy: “Look, I know it’s going to be hard for some time, but once we’re done and a few million people die, the rest of us will be immune to it, so this virus will stop spreading and we’ll say goodbye to the coronavirus. Better do it at once and be done with it, because our alternative is to do social distancing for up to a year and risk having this peak happen later anyways.”
Except this assumes one thing: the virus doesn’t change too much. If it doesn’t change much, then lots of people do get immunity, and at some point the epidemic dies down
How likely is this virus to mutate? It seems it already has.
This graph represents the different mutations of the virus. You can see that the initial strains started in purple in China and then spread. Each time you see a branching on the left graph, that is a mutation leading to a slightly different variant of the virus.
This should not be surprising: RNA-based viruses like the coronavirus or the flu tend to mutate around 100 times faster than DNA-based ones—although the coronavirus mutates more slowly than influenza viruses.
Not only that, but the best way for this virus to mutate is to have millions of opportunities to do so, which is exactly what a mitigation strategy would provide: hundreds of millions of people infected.
That’s why you have to get a flu shot every year. Because there are so many flu strains, with new ones always evolving, the flu shot can never protect against all strains.
Put in another way: the mitigation strategy not only assumes millions of deaths for a country like the US or the UK. It also gambles on the fact that the virus won’t mutate too much — which we know it does. And it will give it the opportunity to mutate. So once we’re done with a few million deaths, we could be ready for a few million more — every year. This corona virus could become a recurring fact of life, like the flu, but many times deadlier.
The best way for this virus to mutate is to have millions of opportunities to do so, which is exactly what a mitigation strategy would provide.
So if neither doing nothing and mitigation will work, what’s the alternative? It’s called suppression.
Option 3: Suppression Strategy
The Mitigation Strategy doesn’t try to contain the epidemic, just flatten the curve a bit. Meanwhile, the Suppression Strategy tries to apply heavy measures to quickly get the epidemic under control. Specifically:
Go hard right now. Order heavy social distancing. Get this thing under control.
Then, release the measures, so that people can gradually get back their freedoms and something approaching normal social and economic life can resume.
What does that look like?
All the model parameters are the same, except that there is an intervention around now to reduce the transmission rate to R=0.62, and because the healthcare system isn’t collapsed, the fatality rate goes down to 0.6%. I defined “around now” as having ~32,000 cases when implementing the measures (3x the official number as of today, 3/19). Note that this is not too sensitive to the R chosen. An R of 0.98 for example shows 15,000 deaths. Five times more than with an R of 0.62, but still tens of thousands of deaths and not millions. It’s also not too sensitive to the fatality rate: if it’s 0.7% instead of 0.6%, the death toll goes from 15,000 to 17,000. It’s the combination of a higher R, a higher fatality rate, and a delay in taking measures that explodes the number of fatalities. That’s why we need to take measures to reduce R today. For clarification, the famous R0 is R at the beginning (R at time 0). It’s the transmission rate when nobody is immune yet and there are no measures against it taken. R is the overall transmission rate.
Under a suppression strategy, after the first wave is done, the death toll is in the thousands, and not in the millions.
Why? Because not only do we cut the exponential growth of cases. We also cut the fatality rate since the healthcare system is not completely overwhelmed. Here, I used a fatality rate of 0.9%, around what we’re seeing in South Korea today, which has been most effective at following Suppression Strategy.
Said like this, it sounds like a no-brainer. Everybody should follow the Suppression Strategy.
So why do some governments hesitate?
They fear three things:
This first lockdown will last for months, which seems unacceptable for many people.
A months-long lockdown would destroy the economy.
It wouldn’t even solve the problem, because we would be just postponing the epidemic: later on, once we release the social distancing measures, people will still get infected in the millions and die.
Here is how the Imperial College team modeled suppressions. The green and yellow lines are different scenarios of Suppression. You can see that doesn’t look good: We still get huge peaks, so why bother?
We’ll get to these questions in a moment, but there’s something more important before.
This is completely missing the point.
Presented like these, the two options of Mitigation and Suppression, side by side, don’t look very appealing. Either a lot of people die soon and we don’t hurt the economy today, or we hurt the economy today, just to postpone the deaths.
This ignores the value of time.
3. The Value of Time
In our previous post, we explained the value of time in saving lives. Every day, every hour we waited to take measures, this exponential threat continued spreading. We saw how a single day could reduce the total cases by 40% and the death toll by even more.
But time is even more valuable than that.
We’re about to face the biggest wave of pressure on the healthcare system ever seen in history. We are completely unprepared, facing an enemy we don’t know. That is not a good position for war.
What if you were about to face your worst enemy, of which you knew very little, and you had two options: Either you run towards it, or you escape to buy yourself a bit of time to prepare. Which one would you choose?
This is what we need to do today. The world has awakened. Every single day we delay the coronavirus, we can get better prepared. The next sections detail what that time would buy us:
Lower the Number of Cases
With effective suppression, the number of true cases would plummet overnight, as we saw in Hubei last week.
As of today, there are 0 daily new cases of coronavirus in the entire 60 million-big region of Hubei.
The diagnostics would keep going up for a couple of weeks, but then they would start going down. With fewer cases, the fatality rate starts dropping too. And the collateral damage is also reduced: fewer people would die from non-coronavirus-related causes because the healthcare system is simply overwhelmed.
Suppression would get us:
Fewer total cases of Coronavirus
Immediate relief for the healthcare system and the humans who run it
Reduction in fatality rate
Reduction in collateral damage
Ability for infected, isolated and quarantined healthcare workers to get better and back to work. In Italy, healthcare workers represent 8% of all contagions.
Understand the True Problem: Testing and Tracing
Right now, the UK and the US have no idea about their true cases. We don’t know how many there are. We just know the official number is not right, and the true one is in the tens of thousands of cases. This has happened because we’re not testing, and we’re not tracing.
With a few more weeks, we could get our testing situation in order, and start testing everybody. With that information, we would finally know the true extent of the problem, where we need to be more aggressive, and what communities are safe to be released from a lockdown.
We could also set up a tracing operation like the ones they have in China or other East Asia countries, where they can identify all the people that every sick person met, and can put them in quarantine. This would give us a ton of intelligence to release later on our social distancing measures: if we know where the virus is, we can target these places only. This is not rocket science: it’s the basics of how East Asia Countries have been able to control this outbreak without the kind of draconian social distancing that is increasingly essential in other countries.
The measures from this section (testing and tracing) single-handedly curbed the growth of the coronavirus in South Korea and got the epidemic under control, without a strong imposition of social distancing measures.
Build Up Capacity
The US (and presumably the UK) are about to go to war without armor.
We have masks for just two weeks, few personal protective equipments (“PPE”), not enough ventilators, not enough ICU beds, not enough ECMOs (blood oxygenation machines)… This is why the fatality rate would be so high in a mitigation strategy.
But if we buy ourselves some time, we can turn this around:
We have more time to buy equipment we will need for a future wave
We can quickly build up our production of masks, PPEs, ventilators, ECMOs, and any other critical device to reduce fatality rate.
Put in another way: we don’t need years to get our armor, we need weeks. Let’s do everything we can to get our production humming now. Countries are mobilized. People are being inventive, such as using 3D printing for ventilator parts. We can do it. We just need more time. Would you wait a few weeks to get yourself some armor before facing a mortal enemy?
This is not the only capacity we need. We will need health workers as soon as possible. Where will we get them? We need to train people to assist nurses, and we need to get medical workers out of retirement. Many countries have already started, but this takes time. We can do this in a few weeks, but not if everything collapses.
Lower Public Contagiousness
The public is scared. The coronavirus is new. There’s so much we don’t know how to do yet! People haven’t learned to stop hand-shaking. They still hug. They don’t open doors with their elbow. They don’t wash their hands after touching a door knob. They don’t disinfect tables before sitting.
Once we have enough masks, we can use them outside of the healthcare system too. Right now, it’s better to keep them for healthcare workers. But if they weren’t scarce, people should wear them in their daily lives, making it less likely that they infect other people when sick, and with proper training also reducing the likelihood that the wearers get infected. (In the meantime, wearing something is better than nothing.)
All of these are pretty cheap ways to reduce the transmission rate. The less this virus propagates, the fewer measures we’ll need in the future to contain it. But we need time to educate people on all these measures and equip them.
Understand the Virus
We know very very little about the virus. But every week, hundreds of new papers are coming.
The world is finally united against a common enemy. Researchers around the globe are mobilizing to understand this virus better.
How does the virus spread? How can contagion be slowed down? What is the share of asymptomatic carriers? Are they contagious? How much? What are good treatments? How long does it survive? On what surfaces? How do different social distancing measures impact the transmission rate? What’s their cost? What are tracing best practices? How reliable are our tests?
Clear answers to these questions will help make our response as targeted as possible while minimizing collateral economic and social damage. And they will come in weeks, not years.
Find Treatments
Not only that, but what if we found a treatment in the next few weeks? Any day we buy gets us closer to that. Right now, there are already several candidates, such as Favipiravir, Chloroquine, or Chloroquine combined with Azithromycin. What if it turned out that in two months we discovered a treatment for the coronavirus? How stupid would we look if we already had millions of deaths following a mitigation strategy?
Understand the Cost-Benefits
All of the factors above can help us save millions of lives. That should be enough. Unfortunately, politicians can’t only think about the lives of the infected. They must think about all the population, and heavy social distancing measures have an impact on others.
Right now we have no idea how different social distancing measures reduce transmission. We also have no clue what their economic and social costs are.
Isn’t it a bit difficult to decide what measures we need for the long term if we don’t know their cost or benefit?
A few weeks would give us enough time to start studying them, understand them, prioritize them, and decide which ones to follow.
Fewer cases, more understanding of the problem, building up assets, understanding the virus, understanding the cost-benefit of different measures, educating the public… These are some core tools to fight the virus, and we just need a few weeks to develop many of them. Wouldn’t it be dumb to commit to a strategy that throws us instead, unprepared, into the jaws of our enemy?
4. The Hammer and the Dance
Now we know that the Mitigation Strategy is probably a terrible choice, and that the Suppression Strategy has a massive short-term advantage.
But people have rightful concerns about this strategy:
How long will it actually last?
How expensive will it be?
Will there be a second peak as big as if we didn’t do anything?
Here, we’re going to look at what a true Suppression Strategy would look like. We can call it the Hammer and the Dance.
The Hammer
First, you act quickly and aggressively. For all the reasons we mentioned above, given the value of time, we want to quench this thing as soon as possible.
One of the most important questions is: How long will this last?
The fear that everybody has is that we will be locked inside our homes for months at a time, with the ensuing economic disaster and mental breakdowns. This idea was unfortunately entertained in the famous Imperial College paper:
Do you remember this chart? The light blue area that goes from end of March to end of August is the period that the paper recommends as the Hammer, the initial suppression that includes heavy social distancing.
If you’re a politician and you see that one option is to let hundreds of thousands or millions of people die with a mitigation strategy and the other is to stop the economy for five months before going through the same peak of cases and deaths, these don’t sound like compelling options.
But this doesn’t need to be so. This paper, driving policy today, has been brutally criticized for core flaws: They ignore contact tracing (at the core of policies in South Korea, China or Singapore among others) or travel restrictions (critical in China), ignore the impact of big crowds…
The time needed for the Hammer is weeks, not months.
This graph shows the new cases in the entire Hubei region (60 million people) every day since 1/23. Within 2 weeks, the country was starting to get back to work. Within ~5 weeks it was completely under control. And within 7 weeks the new diagnostics was just a trickle. Let’s remember this was the worst region in China.
Remember again that these are the orange bars. The grey bars, the true cases, had plummeted much earlier (see Chart 9).
The measures they took were pretty similar to the ones taken in Italy, Spain or France: isolations, quarantines, people had to stay at home unless there was an emergency or had to buy food, contact tracing, testing, more hospital beds, travel bans…
Details matter, however.
China’s measures were stronger. For example, people were limited to one person per household allowed to leave home every three days to buy food. Also, their enforcement was severe. It is likely that this severity stopped the epidemic faster.
In Italy, France and Spain, measures were not as drastic, and their implementation is not as tough. People still walk on the streets, many without masks. This is likely to result in a slower Hammer: more time to fully control the epidemic.
Some people interpret this as “Democracies will never be able to replicate this reduction in cases”. That’s wrong.
For several weeks, South Korea had the worst epidemic outside of China. Now, it’s largely under control. And they did it without asking people to stay home. They achieved it mostly with very aggressive testing, contact tracing, and enforced quarantines and isolations.
The following table gives a good sense of what measures different countries have followed, and how that has impacted them (this is a work-in-progress. Feedback welcome.)
This shows how countries who were prepared, with stronger epidemiological authority, education on hygiene and social distancing, and early detection and isolation, didn’t have to pay with heavier measures afterwards.
Conversely, countries like Italy, Spain or France weren’t doing these well, and had to then apply the Hammer with the hard measures at the bottom to catch up.
The lack of measures in the US and UK is in stark contrast, especially in the US. These countries are still not doing what allowed Singapore, South Korea or Taiwan to control the virus, despite their outbreaks growing exponentially. But it’s a matter of time. Either they have a massive epidemic, or they realize late their mistake, and have to overcompensate with a heavier Hammer. There is no escape from this.
But it’s doable. If an outbreak like South Korea’s can be controlled in weeks and without mandated social distancing, Western countries, which are already applying a heavy Hammer with strict social distancing measures, can definitely control the outbreak within weeks. It’s a matter of discipline, execution, and how much the population abides by the rules.
Once the Hammer is in place and the outbreak is controlled, the second phase begins: the Dance.
The Dance
If you hammer the coronavirus, within a few weeks you’ve controlled it and you’re in much better shape to address it. Now comes the longer-term effort to keep this virus contained until there’s a vaccine.
This is probably the single biggest, most important mistake people make when thinking about this stage: they think it will keep them home for months. This is not the case at all. In fact, it is likely that our lives will go back to close to normal.
In this video, the South Korea Foreign Minister explains how her country did it. It was pretty simple: efficient testing, efficient tracing, travel bans, efficient isolating and efficient quarantining.
Want to guess their measures? The same ones as in South Korea. In their case, they complemented with economic help to those in quarantine and travel bans and delays.
Is it too late for these countries and others? No. By applying the Hammer, they’re getting a new chance, a new shot at doing this right. The more they wait, the heavier and longer the hammer, but it can control the epidemics.
But what if all these measures aren’t enough?
The Dance of R
I call the months-long period between the Hammer and a vaccine or effective treatment the Dance because it won’t be a period during which measures are always the same harsh ones. Some regions will see outbreaks again, others won’t for long periods of time. Depending on how cases evolve, we will need to tighten up social distancing measures or we will be able to release them. That is the dance of R: a dance of measures between getting our lives back on track and spreading the disease, one of economy vs. healthcare.
How does this dance work?
It all turns around the R. If you remember, it’s the transmission rate. Early on in a standard, unprepared country, it’s somewhere between 2 and 3: During the few weeks that somebody is infected, they infect between 2 and 3 other people on average.
If R is above 1, infections grow exponentially into an epidemic. If it’s below 1, they die down.
During the Hammer, the goal is to get R as close to zero, as fast as possible, to quench the epidemic. In Wuhan, it is calculated that R was initially 3.9, and after the lockdown and centralized quarantine, it went down to 0.32.
But once you move into the Dance, you don’t need to do that anymore. You just need your R to stay below 1: a lot of the social distancing measures have true, hard costs on people. They might lose their job, their business, their healthy habits…
You can remain below R=1 with a few simple measures.
This is an approximation of how different types of patients respond to the virus, as well as their contagiousness. Nobody knows the true shape of this curve, but we’ve gathered data from different papers to approximate how it looks like.
Every day after they contract the virus, people have some contagion potential. Together, all these days of contagion add up to 2.5 contagions on average.
It is believed that there are some contagions already happening during the “no symptoms” phase. After that, as symptoms grow, usually people go to the doctor, get diagnosed, and their contagiousness diminishes.
For example, early on you have the virus but no symptoms, so you behave as normal. When you speak with people, you spread the virus. When you touch your nose and then open door knob, the next people to open the door and touch their nose get infected.
The more the virus is growing inside you, the more infectious you are. Then, once you start having symptoms, you might slowly stop going to work, stay in bed, wear a mask, or start going to the doctor. The bigger the symptoms, the more you distance yourself socially, reducing the spread of the virus.
Once you’re hospitalized, even if you are very contagious you don’t tend to spread the virus as much since you’re isolated.
This is where you can see the massive impact of policies like those of Singapore or South Korea:
If people are massively tested, they can be identified even before they have symptoms. Quarantined, they can’t spread anything.
If people are trained to identify their symptoms earlier, they reduce the number of days in blue, and hence their overall contagiousness
If people are isolated as soon as they have symptoms, the contagions from the orange phase disappear.
If people are educated about personal distance, mask-wearing, washing hands or disinfecting spaces, they spread less virus throughout the entire period.
Only when all these fail do we need heavier social distancing measures.
The ROI of Social Distancing
If with all these measures we’re still way above R=1, we need to reduce the average number of people that each person meets.
There are some very cheap ways to do that, like banning events with more than a certain number of people (eg, 50, 500), or asking people to work from home when they can.
Other are much, much more expensive economically, socially and ethically, such as closing schools and universities, asking everybody to stay home, or closing businesses.
This chart is made up because it doesn’t exist today. Nobody has done enough research about this or put together all these measures in a way that can compare them.
It’s unfortunate, because it’s the single most important chart that politicians would need to make decisions. It illustrates what is really going through their minds.
During the Hammer period, politicians want to lower R as much as possible, through measures that remain tolerable for the population. In Hubei, they went all the way to 0.32. We might not need that: maybe just to 0.5 or 0.6.
But during the Dance of the R period, they want to hover as close to 1 as possible, while staying below it over the long term term. That prevents a new outbreak, while eliminating the most drastic measures.
What this means is that, whether leaders realize it or not, what they’re doing is:
List all the measures they can take to reduce R
Get a sense of the benefit of applying them: the reduction in R
Get a sense of their cost: the economic, social, and ethical cost.
Stack-rank the initiatives based on their cost-benefit
Pick the ones that give the biggest R reduction up till 1, for the lowest cost.
This is for illustrative purposes only. All data is made up. However, as far as we were able to tell, this data doesn’t exist today. It needs to. For example, the list from the CDC is a great start, but it misses things like education measures, triggers, quantifications of costs and benefits, measure details, economic / social countermeasures…
Initially, their confidence on these numbers will be low. But that‘s still how they are thinking—and should be thinking about it.
What they need to do is formalize the process: Understand that this is a numbers game in which we need to learn as fast as possible where we are on R, the impact of every measure on reducing R, and their social and economic costs.
Only then will they be able to make a rational decision on what measures they should take.
Conclusion: Buy Us Time
The coronavirus is still spreading nearly everywhere. 152 countries have cases. We are against the clock. But we don’t need to be: there’s a clear way we can be thinking about this.
Some countries, especially those that haven’t been hit heavily yet by the coronavirus, might be wondering: Is this going to happen to me? The answer is: It probably already has. You just haven’t noticed. When it really hits, your healthcare system will be in even worse shape than in wealthy countries where the healthcare systems are strong. Better safe than sorry, you should consider taking action now.
For the countries where the coronavirus is already here, the options are clear.
On one side, countries can go the mitigation route: create a massive epidemic, overwhelm the healthcare system, drive the death of millions of people, and release new mutations of this virus in the wild.
On the other, countries can fight. They can lock down for a few weeks to buy us time, create an educated action plan, and control this virus until we have a vaccine.
Governments around the world today, including some such as the US, the UK or Switzerland have so far chosen the mitigation path.
That means they’re giving up without a fight. They see other countries having successfully fought this, but they say: “We can’t do that!”
What if Churchill had said the same thing? “Nazis are already everywhere in Europe. We can’t fight them. Let’s just give up.” This is what many governments around the world are doing today. They’re not giving you a chance to fight this. You have to demand it.
Share the Word
Unfortunately, millions of lives are still at stake. Share this article—or any similar one—if you think it can change people’s opinion. Leaders need to understand this to avert a catastrophe. The moment to act is now.
If you are an expert in the field and want to criticize or endorse the article or some of its parts, feel free to leave a private note here or contextually and I will respond or address.
If you want to translate this article, do it on a Medium post and leave me a private note here with your link. Here are the translations currently available:
This article has been the result of a herculean effort by a group of normal citizens working around the clock to find all the relevant research available to structure it into one piece, in case it can help others process all the information that is out there about the coronavirus.
Special thanks to Dr. Carl Juneau (epidemiologist and translator of the French version), Dr. Brandon Fainstad, Pierre Djian, Jorge Peñalva, John Hsu, Genevieve Gee, Elena Baillie, Chris Martinez, Yasemin Denari, Christine Gibson, Matt Bell, Dan Walsh, Jessica Thompson, Karim Ravji, Annie Hazlehurst, and Aishwarya Khanduja. This has been a team effort.
Thank you also to Berin Szoka, Shishir Mehrotra, QVentus, Illumina, Josephine Gavignet, Mike Kidd, and Nils Barth for your advice. Thank you to my company, Course Hero, for giving me the time and freedom to focus on this.
2 MSc in Engineering. Stanford MBA. Ex-Consultant. Creator of viral applications with >20M users. Currently leading a billion-dollar business @ Course Hero
Thomas Friedman, um dos colunistas mais influentes do mundo, ouviu três médicos e escreveu o artigo mais contundente até agora sobre o risco do lockdown global se estender por muito tempo.
No texto, publicado hoje à tarde no The New York Times, Friedman nota que os políticos estão tendo que tomar “decisões enormes de vida ou morte, enquanto atravessam uma neblina com informação imperfeita e todo mundo no banco de trás gritando com eles. Eles estão fazendo o melhor que podem.”
Mas com o desemprego se alastrando pelo mundo tão rápido quanto o vírus, “alguns especialistas estão começando a questionar: ‘Espera um minuto! O que estamos fazendo com nós mesmos? Com nossa economia? Com a próxima geração? Será que essa cura — mesmo que por um período curto — será pior que a doença?’”
Friedman diz que as lideranças políticas estão ouvindo o conselho de epidemiologistas sérios e especialistas em saúde pública. Ainda assim, ele diz que o mundo tem que ter cuidado com o “pensamento de grupo” e que até “pequenas escolhas erradas podem ter grandes consequências.”
Para ele, a questão é como podemos ser mais cirúrgicos na resposta ao vírus de forma a manter a letalidade baixa e ao mesmo tempo permitir que as pessoas voltem ao trabalho o mais cedo possível e com segurança.
Friedman diz que “se a minha caixa de email for alguma indicação, uma reação mais inteligente está começando a brotar.”
Ele cita um artigo publicado semana passada pelo Dr. John P. A. Ioannidis, um epidemiologista e co-diretor do Centro de Inovação em Meta-Pesquisa de Stanford. No artigo, Ioannidis diz que a comunidade científica ainda não sabe exatamente qual é a taxa de mortalidade do coronavírus. Segundo ele, “as evidências disponíveis hoje indicam que a letalidade pode ser de 1% ou ainda menor.”
“Se essa for a taxa verdadeira, paralisar o mundo todo com implicações financeiras e sociais potencialmente tremendas pode ser totalmente irracional. É como um elefante sendo atacado por um gato doméstico. Frustrado e tentando fugir do gato, o elefante acidentalmente pula do penhasco e morre.”
Friedman também cita o Dr. Steven Woolf, diretor emérito do Centro Sobre a Sociedade e Saúde da Universidade da Virgínia, para quem o lockdown “pode ser necessário para conter a transmissão comunitária, mas pode prejudicar a saúde de outras formas, custando vidas.”
“Imagine um paciente com dor no peito ou sofrendo um derrame — casos em que a rapidez de resposta é essencial para salvar vidas — hesitando em chamar o serviço de emergência por medo de pegar coronavírus. Ou um paciente de câncer tendo que adiar sua quimioterapia porque a clínica está fechada.”
Friedman complementa: “Imagine o estresse e a doença mental que virá — já está vindo — de termos fechado a economia, gerando desemprego em massa.”
Woolf, o médico da Virgínia, afirma no artigo que a renda é uma das variáveis mais fortes a afetar a saúde e a longevidade. “Os pobres, que já sofrem há gerações com taxas de mortalidade mais altas, serão os mais prejudicados e provavelmente os que receberão menos ajuda. São as camareiras dos hotéis fechados e as famílias sem opções quando o transporte público fecha.”
Há outro caminho?, pergunta Friedman.
Para ele, a melhor ideia até agora veio do Dr. David Katz, diretor do Centro de Prevenção e Pesquisa da Universidade de Yale e um especialista em saúde pública e medicina preventiva.
Num artigo publicado sexta-feira no The New York Times, o Dr. Katz diz que há três objetivos neste momento: salvar tantas vidas quanto possível, garantindo que o sistema de saúde não entre em colapso, “mas também garantir que no processo de atingir os dois primeiros objetivos não destruamos nossa economia e, como resultado disso, ainda mais vidas.”
Como fazer isso?
Katz diz que o mundo tem que pivotar da estratégia de “interdição horizontal” que estamos empregando agora — restringindo o movimento e o comércio de toda a população, sem considerar a variância no risco de infecção severa — para uma estratégia mais “cirúrgica”, ou de “interdição vertical”.
“A abordagem cirúrgica e vertical focaria em proteger e isolar os que correm maior risco de morrer ou sofrer danos de longo prazo — isto é, os idosos, pessoas com doenças crônicas e com baixa imunidade — e tratar o resto da sociedade basicamente da mesma forma que sempre lidamos com ameaças mais familiares como a gripe.”
Katz sugere que o isolamento atual dure duas semanas, em vez de um período indefinido. Para os infectados, os sintomas aparecerão nesse período. “Aqueles que tiverem uma infecção sintomática devem se auto-isolar em seguida, com ou sem testes, que é exatamente o que fazemos com a gripe. Quem não estiver sintomático e fizer parte da população de baixo risco deveria voltar ao trabalho ou a escola depois daquelas duas semanas.”
“O efeito rejuvenescedor na alma humana e na economia — de saber que existe luz no fim do túnel — é difícil de superestimar. O risco não será zero, mas o risco de acontecer algo ruim com qualquer um de nós em qualquer dia da nossa vida nunca é zero.”
A medical official outside an emergency tent installed for patients infected by COVID-19 in Poland- Credit Sky News
Covid-19 is a flu-like illness (symptoms include fever, cough, and breathing problems) caused by a corona virus (SARS CoV-2). Like Ebola, the virus causing Covid-19 circulates within populations of bats and crossed over to humans via the bush meat trade. The first human cases were identified in China in December 2019, and the infection has now (March 2020) reached more than 100 countries.
The disease is now recognised by the World Health Organization as a pandemic. Up to 80 percent of the population of some countries might eventually become infected. Most cases will be mild, and recovery spontaneous. About 5 percent of cases will be life-threatening. Death rates appear to be around 1-2 percent. The elderly are most at risk.[1]
Currently, attention is focused on reducing the rate at which Covid-19 spreads. One aim is to delay the peak of infection beyond the winter flu period in the northern hemisphere, when medical help is stretched. Slowing the epidemic also allows more time for preparation of health systems to cope with large numbers, and for work on vaccine development.
Predictably, some politicians have demanded border closures against immigrants and refugees, even though spread is associated with tourism and normal business travel. Africans internationally stigmatised by Ebola might feel aggrieved that cases of Covid-19 have been introduced from Europe and Asia. But in a globally connected and inter-dependent world blaming and stigmatising helps no one. It is better to share ideas about what can be done to protect.
This is where Africa’s experience of Ebola has something to offer. Communities experiencing Ebola in West Africa in 2014-15 rapidly learnt from scratch how to cope with a deadly new infection, and this provides the rest of the world with important information on strategies to address novel disease threats more generally.
Like Ebola, Covid-19 is a family disease, in the sense that many infections occur in the home. Restrictions on travel can slow the spread of the disease, but it also helps if individuals and families understand infection pathways and implement domestic precautions. This is something in which West Africans confronted by Ebola have had much experience.
The name for Ebola in Mende, one of the main languages of Sierra Leone, the worst affected country in 2014-15, was bonda wote, literally ‘family turn round’. In other words, it was clearly recognised that this was a disease requiring families to change behaviour in major ways, especially in how they cared for the sick.
Covid-19 will require similar changes at the family level, especially in terms of how the elderly are protected. The buzz words for epidemic responders include self-isolation and social distancing, but the details of how to implement these vague concepts have been left to local social imagination.
Answers are required for both the uninfected elderly, and for others who are sick.
Should grandpa be packed off to a shed in the garden away from the family for his own protection? What happens when grandma gets lonely and wants to see the grandchildren? Who does the shopping? How does the daily-paid worker ‘self-isolate’ when there is no sick pay? Who collects the children from school when a single mum is sick?
Much depends on actual family arrangements and housing stock. So African solutions for Ebola will not work directly in other parts of the world. But it is important to know that under the challenge of Ebola local people showed much inventiveness in devising solutions to such problems.
Evidence shows that ways can be found to reduce family risks of infection, even with a disease 30 times more deadly than Covid-19.[2]For Ebola, these ranged from the elbow knock that replaced shaking of hands as a public greeting, to the appointment of a single carer in the household to look after the sick while waiting for help, to the carefully choreographed ‘safe and respectful’ funerals that allowed some element of local ritual back into the burial process, a major source of infection.
Every encouragement should be given to this local adaptive creativity, and the authorities should listen carefully to information from below about what would help to make a difference.
However, Covid-19 is not Ebola, and differences have to be taken into account. Some of the major questions about how the disease spreads are as yet unknown, and citizens and households need to be listening for this information as it becomes available and helped to adapt to its implications in real time.
This implies having very good means of two-way communication. In Sierra Leone a telephone helpline, ‘117’, played an important part in arranging emergency Ebola response, but it was much poorer at harvesting feedback from communities about what could be done better.
It seems that the lesson has not been learnt with Covid-19. In Britain, the National Health Service helpline, ‘111’ has now been ‘stood down’ for Covid-19 enquiries relating to domestic testing, since the epidemic is deemed to have passed into a new phase. How then are the authorities to have a conversation with families about the resources most needed for adaptation at household level?
Case-handling is a second area of difference. Ebola does not spread easily. The virologist Peter Piot put it well when he stated that he would have no problem sitting next to someone with Ebola provided they were not vomiting over him. Infection spreads only through contact with body fluids. Covid-19, however, spreads through the air, as well as via bodily contact, and case numbers will be much higher.
With Ebola in West Africa the number of cases turning up at specialist Ebola care facilities at the height of the epidemic numbered in tens or hundreds per week. With Covid-19 the numbers of cases requiring intensive care at the peak of the epidemic may amount to hundreds of thousands.
Even if stretched out over several months infection on this scale implies a large extra demand for medical care.
Ebola taught that epidemics cause deaths from other diseases through their impact on health systems. In all there were about 12,000 Ebola deaths in Upper West Africa (Guinea, Liberia, Sierra Leone) in 2014-15 but many additional fatalities resulted from, for example, closure of facilities such as maternity clinics.
So contingency planning is required. A key challenge for Covid-19 is how health system care should best be organized, without severely disrupting other forms of health provision.
For Ebola, the first response was to build large field hospitals (Ebola Treatment Centres).[3]These were seen as the safest option. But they were shunned by families, because so few patients came out alive. They were also often in the wrong place (built behind, not ahead, of the epidemic).
Information started to filter through that some communities were taking their own steps to reduce infection and bury the dead. This raised the question whether there was more scope for community care.
Family do-it-yourself responses proved controversial. International responders were adamant that there would be nothing resembling home care; it was too dangerous. Local communities were equally adamant that there would have to be some form of home care; they could not stand by and watch family members die, when an ambulance to take a patient to an ETC might take days to arrive over bad or non-existent roads.
Families saw it as their duty to be involved in care of the sick. So, they repeatedly asked what to do while waiting for help to arrive. Could they not prepare food for the sick? Could they not be trained to safely bury the dead?
No, they were told. Ebola required specialist management.
Communities answered back. They pointed to areas at the outset of the epidemic, where the epidemic was rolled back with only local resources. In Kailahun District, for example, an intense initial outbreak was reduced to a trickle of cases by local responders organizing quarantine and burial with improvised resources. That cases then declined without outside help implied either that the disease burnt out more readily than anticipated, or that local improvisation worked better than expected. There is evidence to support both interpretations.[4]
Experts knew that Ebola control required prompt diagnosis, before the ‘wet’ symptoms of the disease became apparent. Something had to be done to speed up the presentation of cases. The answer was to build much smaller community care centres (CCC) close to where active transmission was taking place.[5]This also changed the relationship between families and Ebola responders from fear to active cooperation.
Staff of CCC were for the most part local volunteers – trained nurses who had not been absorbed on to the payroll of the Ministry of Health, or villagers willing to take on high-risk chores for a decent wage. The fact that staffing was local meant patients saw familiar faces, and this built trust. CCC also normalized Ebola by bringing treatment within a framework of general medical assistance.
As a result, patients were presented more promptly than was the case with the distant ETC. Ebola (indistinguishable from malaria or typhoid in its early phase) was more rapidly identified and isolated. One study estimates that CCC contributed up to one third of the infection control ending the epidemic in Sierra Leone.[6]
This example of responders modifying their approach to infection control better to accommodate family requirements may hold lessons for Covid-19.
Specifically, cases may have to be kept out of main hospitals as much as possible, Thus, there may be a need for field treatment facilities not dissimilar to CCC, as a half-way house between home isolation and intensive care. In effect these facilities would isolate and triage the most vulnerable cases, as was the case with Ebola CCC.
There is also a possibility that any such facilities might be run up by military personnel[7]and staffed by medically trained ‘volunteers’ (retired doctors and nurses), as in Sierra Leone.
Interesting to note, the chief medical advisor for England was previously one of the proponents of the introduction of CCC in Sierra Leone, and we may be about to see some lessons directly transferred.[8]
Quarantine for Ebola in Sierra Leone is also an issue from which Covid-19 responders might wish to draw lessons. Much of it was organised and imposed by the state, and was at times heavy-handed. But communities also organised their own quarantine. They understood that self-isolation was in their own interest, and this sometimes worked surprisingly effectively.
Use was made of an approach used during the civil war of 1991-2002 of mobilising community youth to identify infiltrators. Visitors who might have been carrying the virus were turned away. But in other cases the approach was more focused on sequestering those who were well. Rural families sometimes decamped from villages with outbreaks to settle down for a few weeks in their farms, where sleeping quarters were sometimes built for the purpose.
In this respect, Sierra Leonean rural communities showed a clear appreciation of the fact that there were two distinct kinds of quarantine – self-isolation and protective sequestration. Both kinds are being used as part of the response to Covid-19, but at times without adequate discussion of how the two types differ and have different social motivations – self-protection and altruism towards neighbours. It is not wise to talk about self-isolation for the sick and the elderly in the same breath. The different motivations need to be more clearly explained.
In conclusion, it is also important to say something about what Africa can learn from its own experience of Ebola. The point made above should be reiterated – about the differences as well as similarities between Covid-19 and Ebola.
Prompt case finding, contact tracing and quarantine are being applied to Covid-19 as they were for Ebola.[9]Good hygiene practices, such as hand washing, also remain applicable. African countries with experience of Ebola know how to do these things, and this will be helpful in dealing with early cases.
However, African countries also have to be prepared to learn to adapt to the specific features of this new disease as more data emerge. This will pose more of a challenge, since this will require rapid knowledge-based domestic adaptation to new information on how Covid-19 spreads (perhaps most notably, why it affects the old more than the young, and how older people might be best protected from its effects).
The main lesson for both Africa and other parts of the world from Ebola for Covid-19, however, is that shared learning between communities and medical professionals is a key aspect of human adaptive response to emergent diseases. In any disease in which community mobilization is an important aspect families need to think like epidemiologists, but equally epidemiologists need to think like families.
Paul Richards’ Ebola book front cover, part of the African Arguments book series
References:
[1]Xu, J., Zhao, S., Teng T., Abdalla, A.E., Zhu, W., Xie, L., Wang, Y., Guo, X. (2020) ‘Systematic comparison of two animal-to-human transmitted human coronaviruses: SARS-CoV-2 and SARS-CoV’, Viruses 12, 244.
[2]Richards, P. (2016) Ebola: How a People’s Science Helped End an Epidemic, London: Zed Books.
[3]Richards, P., Mokuwa, E., Welmers, P., Maat, H., Beisel, U. (2019) ‘Trust, and distrust, of Ebola Treatment Centers: a case-study from Sierra Leone’, PLoS ONE14(12): e0224511. https://doi.org/10.1371/journal.pone.0224511.
[4]Glynn, Judith R. et al. (2017) ‘Asymptomatic infection and unrecognised Ebola virus disease in Ebola-affected households in Sierra Leone: a cross-sectional study using a new non-invasive assay for antibodies to Ebola virus’,Lancet Infectious Diseases17(6), 645-653. On local case finding, quarantine and burial procedures see Richards (2016) op. cit.
[5]Mokuwa, E.Y., Maat, H. (2020) ‘Rural populations exposed to Ebola Virus Disease respond positively to localised case handling: evidence from Sierra Leone’, PLoS Negl Trop Dis 14(1): e0007666. https://doi.org/10.1371/journal.pntd.0007666.
[6]Pronyk, P., Rogers, B., Lee, S., Bhatnagar, A., Wolman, Y., Monasch, R., Hipgrave, D., Salama, P., Kucharski, A., Chopra, M., and on behalf of the UNICEF Sierra Leone Ebola Response Team, (2016) ‘The effect of community-based prevention and care on Ebola transmission in Sierra Leone’,American Journal of Public Health 106, 727–32, https://doi.org/10.2105/AJPH.2015.303020.
[7]Aaaron Walawalkar and Jamie Grierson, The Guardian,8 March 2020, 14.12 GMT.
[8]Whitty, C.J.M., Farrar, J., Ferguson, N., Edmunds, W.J., Piot, P., Leach, M., Davies, S.C. (2014) ‘Tough choices to reduce Ebola transmission’, Nature515, 13 November, 192–4; see also Ian Sample and Lisa O’Carroll ‘Prof Chris Whitty – the expert we need in the coronavirus crisis’, Guardian,4 March 2020.
Most of us face multiple hardships in life—financial stress, job loss, divorce, the premature death of a spouse or parent. Painful and unsettling life events divert our lives into unimaginable paths filled with stress and pain. Like most people, I have experienced a number of painful events: religious discrimination, the suicide of a loved one, divorce, and the death of parents. I have also been diagnosed with and treated for Non-Hodgkin Lymphoma (NHL), a series of blood cancers most of which are classified as incurable. These life-altering experiences have shaped the course of my personal and professional life—in unexpected ways.
My life as an anthropologist has afforded me a particular perspective on existentially troubling life events. During early fieldwork in the Republic of Niger, one of the poorest nations in the world, I had to confront the psychological and existential ramifications of yearly meningitis outbreaks. These always occurred during the hot dry season—from March until the first rains of June. In hot and dry conditions that were perfect for transmission, a few of my students, some of my friends and many children got sick.
Many of the children died.
One year during a particularly bad outbreak I witnessed daily processions of men and women carrying the newly dead to their final resting place. Men walked silently their gazes downcast. Women wailed as they accompanied their loved ones to the cemetery. During that outbreak, a pall settled over the rural village where I lived. Conversations lapsed into stressful silences. We all wondered if we would be next. Was the tightness in my neck muscular, or was it the onset of meningitis? Invisible and silent, the scourge of meningitis put my life at risk, a visceral threat that forced me to consider what was important in my life.
In Niger, hot and dry conditions create a perfect storm for meningitis outbreaks. Source: Paul Stoller
During another year of fieldwork in Niger, I lived through a cholera epidemic. While the transmission of meningitis bacteria and/or virus comes from close contact with infected others—cholera makes its way to human beings through contaminated water or food.
That year, many people in the region of Tillaberi became cholera victims. In response to a flood of new cholera patients, the local government, which had no funds to meet the challenges of the outbreak, set up a makeshift lean-to village—a horrible place to put the sick and dying. The lean-to village had been built close to the dunetop compound where I was living. From our compound we observed the arrival of hundreds of emaciated victims, wrapped in soiled rags, being transported on donkey-pulled carts to the cholera village. The stench of that lean-to village saturated my senses and haunts me to this day. During that time of contagion, conversations focused on the onset of cholera, treatment regimens, and death rates, which soared in an exceedingly poor region of rural Niger. The long shadow of cholera cast its shade on us all. Despite my relative privilege among the poor and destitute, I nonetheless wondered about the safety of my water and food. Would I succumb to cholera? Again, the threat of an epidemic compelled me to think about what mattered in my life: love, family and my contributions, however small they might be, to my community and my profession.
We are now living through the COVID-19 coronavirus pandemic. The deadly virus is spreading exponentially, and there is no apparent end is in sight. An unsettling eeriness extends itself over our lives and our communities. Are we unwitting carriers of the virus who have exposed our loved ones and our friends to the COVID-19 coronavirus? It is a hard reality to bear. Even so, we don’t know if we’ll be infected or not. And if we are infected, we don’t know if our illness will be serious—or even deadly. We are, in fact, living in a moment of a devastating uncertainty in which we have been told to practice social distancing—a good way to slow the rate of contagion. Concerts have been cancelled. Sporting events have been postponed. Theaters have gone dark. In grocery stores, it is difficult to find bread, water, eggs, milk and TP.
Coronavirus shopping on March 14, 2020 Source: Paul Stoller
Travel has been curtailed. Gyms and restaurants are closed. Universities have emptied their dormitories and have transitioned to remote education. K-12 public and private schools have shut their doors. The entire populations of Italy, Spain, France have been placed on lockdown. Where I live, people have been told to stay at home—all to contain the silent and invisible virus. If this surreal scenario is not the end of the world, it may well be the end of social life as we have known it.
The great French surrealist thinker Antonin Artaud thought that most of us make our way through life in a half-conscious state. “You look but you don’t see,” as a wise elder among the Songhay people of Niger and Mali once told me. “You listen but you don’t hear. You touch but you don’t feel.” Indeed, the routine of everyday life can numb our sensibilities. Each day, most of us wake up, go to school, or to work. At midday we eat lunch. At day’s end we return home, enjoy some sort of dinner, enjoy a night watching television, or steaming a film. Sometimes we break the routine. We hang out with our friends. We go out for dinner, have a drink at our favorite bar, or attend a sporting event or a concert.
This routine is, for all intents and purposes, social life as we expect it to unfold. When those expectations are subverted—by an outbreak of meningitis, a cholera epidemic or the COVID-19 coronavirus pandemic—we are forced to change our routines and reconfigure our personal and social expectations. Facing potential illness or possible death, many of us are provoked to think about what is important, about what we might do for our family, our neighbors, our communities.
We are about to experience the full turbulence of a pandemic. There will be isolation, confusion, pain, suffering and loss, but such a state can also provoke penetratingly honest self-reflection, deep listening, existential change, and social transformation. Pandemic hardship can bring on pandemic change. Trapped in this unsettled moment between our past and future, perhaps we can take time to reconnect and, to paraphrase T.S. Elliot, know ourselves for the first time.
Passengers wearing protective face masks stand at Schiphol Airport in Amsterdam, on March 13, 2020, amid an outbreak of COVID-19, the new coronavirus. Photo by OLAF KRAAK/ANP/AFP via Getty Images.
Climate protection and public health have striking similarities. The benefits of both can be enjoyed by everyone, even by individuals who do not contribute to the collective efforts to address these problems. If climate change slows down, both drivers of gas-guzzlers and electric cars will benefit – although the former did not help in climate efforts. Similarly, if the spread of Coronavirus is halted (the so-called flattening the curve), individuals who refused to wash their hands, as well as the ones who washed them assiduously, will enjoy the restored normal life.
Most countries have gotten their acts together, although belatedly, on Coronavirus. Citizens also seem to be following the advice of public health officials. Could then the Coronavirus policy model be applied to climate change? We urge caution because these crises are different, which means that policies that worked well for Coronavirus might not be effective for climate change.
Different Penalties for Policy and Behavioral Procrastination
Climate change is the defining crisis of our times. Floods, hurricanes, forest fires, and extreme weather events have become more frequent and severe over the years. Although climate change generates passionate discussions in big cities and university campuses, there is inadequate public clamor for immediate action. Some types of decarbonization policies are certainly in place. However, carbon-intensive lifestyles continue (with “flying shame” in Scandinavia being an exception). Today In: Green Tech
This policy lethargy and behavioral inertia are due to many reasons, including concerted opposition by the fossil fuel industry to deep decarbonization. But there are other reasons as well. Climate change is cumulative and does not have a quick onset. Its effects are not always immediate and visible. Many individuals probably do not see a clear link between their actions and the eventual outcome. This reduces the willingness to alter lifestyles and tolerate personal sacrifices for the collective good.
In contrast, Coronavirus is forcing an immediate policy response and behavioral changes. Its causality is clear and its onset quick. Lives are at stake, especially in western countries. The stock markets are tanking, and the economy is heading towards a recession. Politicians recognize that waffling can lead to massive consequences, even in the short-term. Corona-skeptic President Trump has reversed course and declared a national emergency.
In the US, there is federal inaction on climate change. But Coronavirus seems different. 2020 is a Presidential election year, and perhaps this motivates the federal government to (finally) act decisively so that Coronavirus does not become Hurricane Katrina type of political liability.
Spatial Optimism
Climate policies are hobbled by “spatial optimism,” whereby individuals believe that their risk of getting affected by climate change is less than for others. This reduces the willingness to tolerate personal sacrifices for deep decarbonization.
Coronavirus episode began with some level of spatial optimism in the Western world. After all, it was happening in China. But this confidence has quickly disappeared. Globalization means a lot of international travel and trade. China is the main global supplier of many products. Prominent companies such as Apple (AAPL) and Tesla (TSLA) depend on China for manufacturing and sales of their products. Spatial optimism has been overwhelmed by international travel as well as globalized supply chains and financial markets.
Belief in the Efficacy of Adaptation
Some might believe that climate change can be “managed.” Innovators will probably develop commercial-scale negative carbon technologies and societies will adapt to sea-level rise by building seawalls, or maybe relocating some communities to safer areas.
Coronavirus offers no such comfort. Unlike the seasonal flu, there is no vaccine (yet). It is difficult to adapt to the Coronavirus threat when you don’t know what to touch, where to go, and if your family members and neighbors are infected. Not to mention, how many rolls of tissue paper you need to stock before the supplies run out at the local grocery store.
Different Incentives to Attack Scientific Knowledge
On Coronavirus, citizens seem to be willing to follow the advice of public health professionals (at least when it comes to social distancing as reflected in empty roads and shopping centers). Every word of Dr. Anthony Fauci counts.
Why has this advice not drawn scorn from politicians who are suspicious of the “deep state”? After all, the same politicians attack scientific consensus on climate change.
Climate skeptics probably see substantial political and economic payoffs by delaying climate action. Stock markets have not penalized climate skepticism in the US: markets hit record high levels in the first three years of the Trump presidency. And, climate opposition is not leading to electoral losses. On the contrary, the climate agendas in liberal states, such as Oregon and Washington, have stalled.
Nobody seems to gain by attacking scientific consensus to delay policy action on Coronavirus. Airlines, hospitality, and tourism industries, who have taken a direct hit from social-distancing policies, probably want the problem to be quickly addressed so that people can get back to their “normal” lives.
US politicians who talk about the “deep state,” may want Coronavirus issue resolved before the November 2020 election. Attacking science does not further their political objectives. After all, the looming recession and the stock market decline could influence the election outcomes.
Depth, Scale, and Duration of Changes
Climate policy will cause economic and social dislocation. Decarbonization means that some industries will shut down. Jobs will be lost, and communities will suffer unless “just transition” policies are in place.
Coronavirus policies will probably not cause long-term structural changes in the economy. People will resume flying, tourists will flock to Venice, Rome, and Paris, and the basketball arenas will again overflow with spectators.
However, some short-term measures could lead to long-term changes. For example, individuals may realize that telecommuting is easy and efficient. As a result, they may permanently reduce their work-related travel. Coronavirus may provide the sort of a “nudge” that shifts long-term behavioral preferences.
In sum, the contrast between the rapid response to Coronavirus and policy waffling on climate change reveals how citizens think of risk and how this shapes their willingness to incur costs for the collective good. Further, it suggests that politicians respect science when its recommendations serve their political ends.
Nives Dolsak is Stan and Alta Barer Professor in Sustainability Science and Director of the School of Marine & Environmental Affairs. Aseem Prakash is the Walker Family Professor and the Director of the Center for Environmental Politics. Both are at the University of Washington, Seattle.
Nações Unidas, 17/4/2014 – Poucos no mundo podem alardear que o câncer não os tocou. Neste momento, milhões enfrentam uma batalha pessoal contra a doença e muitos mais estão sentados juntos a seres queridos que lutam por sua vida, visitando amigos que se recuperam de uma quimioterapia ou averiguando sobre os últimos tratamentos para seus familiares. O prognóstico da organização líder em pesquisa sobre câncer não indica melhorias. O Informe Mundial do Câncer 2014 diz que nos próximos 20 anos se espera que os novos casos aumentem 70%, chegando a 25 milhões em 2025.
Produzido a cada cinco anos pela Agência Internacional para a Pesquisa sobre o Câncer (Iarc), da Organização Mundial da Saúde, o informe de 632 páginas aponta que os novos casos passaram de 12,7 milhões em 2008 para 14,1 milhões em 2012. Neste último ano, o mundo experimentou o recorde de 8,2 milhões de mortes por câncer. Os países em desenvolvimento estão entre a cruz e a espada. Por um lado, seguem sofrendo uma grande presença de tipos de câncer associados a infecções, como o de colo uterino, estômago e fígado, que são relacionados à pobreza e à falta de água potável, vacinas, centros de detecção precoce e opções adequadas de tratamento.
Por outro lado, os tumores relacionados com estilos de vida opulentos, como o de pulmão, mama e intestino grosso – pelo elevado consumo de tabaco, álcool e alimentos pesados – também estão dizimando as fileiras crescentes das classes médias desses países.
A África, por exemplo, experimenta uma “alta alarmante” do tabagismo, e a previsão é que a quantidade de adultos fumantes passe de “77 milhões para 572 milhões até 2100, se não forem aplicadas novas políticas”, afirma a Sociedade Norte-Americana do Câncer. O sul-africano Evan Blecher, diretor do programa internacional de pesquisa sobre controle do tabaco dessa entidade, atribui esse aumento a múltiplos fatores. Um dos principais é o crescimento econômico.
“As economias africanas estão crescendo mais rapidamente e de forma mais sustentada do que nos últimos 50 anos”, afirmou Blecher à IPS, da Cidade do Cabo, sua cidade natal. “O crescimento econômico impulsiona o consumo de tabaco porque há mais dinheiro. Alguns dos países onde vemos maior aumento do tabagismo são Angola, República Democrática do Congo, Etiópia, Madagascar, Moçambique, Senegal e Nigéria, que são os de maior crescimento econômico da África e do mundo”, acrescentou.
Esta dupla carga, de tumores da pobreza e da opulência, paira sobre sistemas de saúde que já estão sob pressão. A Agência Internacional de Energia Atômica (AIEA) informa que os países de renda média e baixa, onde residem 85% da população mundial, possuem apenas 4.400 máquinas de megavoltagem, o que representa menos de 35% das instalações mundiais de radioterapia. A AIEA também afirma que 23 países com mais de um milhão de habitantes cada um, a maioria na África, não têm um só aparelho de radioterapia.
R. Sankaranarayanan, consultor especial da Iarc, pontuou à IPS que a brecha oncológica não separa apenas as nações em diferentes graus de desenvolvimento, mas as populações dentro delas. “A enorme disparidade de sobrevivência de câncer de mama entre as zonas rurais e urbanas de China, Índia e Tailândia, ou entre as populações negras e brancas dos Estados Unidos, é um bom exemplo”, ressaltou. Pesquisadores e médicos dos Estados Unidos dizem que há uma diferença de 8,8% nas taxas de mortalidade por câncer de mama das mulheres negras para as brancas.
Como a obesidade é um grave problema para as comunidades afro-norte-americanas (afeta 50% dos adultos negros e 35% dos brancos), não surpreende que elas tenham maior incidência de câncer colo-retal, associado ao consumo excessivo de alimentos processados e pouco saudáveis.
Na Índia, onde foram registrados mais de um milhão de novos casos em 2012 e quase um milhão de mortes por alguma forma de câncer, a grande diversidade de estilos de vida se mostra como o fator decisivo da brecha oncológica. Por exemplo, a maior incidência de câncer se registrou no Estado de Mizorán, uma das regiões de maior crescimento econômico, enquanto a menor ocorreu em Barshi, distrito rural do Estado de Maharashtra, onde boa parte da população se dedica à atividade agrícola.
Silvana Luciani, assessora em prevenção e controle do câncer da Organização Pan-Americana da Saúde, observou que as disparidades dos serviços de saúde dentro da região também resultam em taxas de mortalidade desequilibradas. “Na América Central a mortalidade por câncer de colo uterino é de 15 ou 18 mortes por cem mil pessoas, enquanto na América do Norte é de duas por cem mil”, detalhou à IPS. “Isso se deve a programas de detecção como o exame papanicolau que são realizados há muito tempo na América do Norte e têm uma qualidade muito maior do que na América Central, onde os serviços de saúde estão fragmentados”, acrescentou.
Sankaranarayanan destacou que países como Coreia do Sul, Turquia, Malásia, Índia, Gana, Marrocos, Brasil, Chile, Colômbia, Costa Rica e México “estão adotando sistemas de saúde de atenção universal ou seguros nacionais de saúde dirigidos às populações mais pobres”. Mas “as populações cada vez mais envelhecidas e o surgimento de tecnologias oncológicas muito caras aumentam as pressões sobre esses serviços”, enfatizou.
Uma barreira ao desenvolvimento
O câncer de pulmão encabeça a lista de diagnósticos, com 1,8 milhão, ou quase 13% do total mundial. Em seguida vem o câncer de mama, com 1,7 milhão, enquanto o que afeta o intestino grosso representa 9,7%.
O mais mortal continua sendo o de pulmão, que mata 1,6 milhão de pessoas por ano, enquanto outras 800 mil falecem por câncer de fígado e 700 mil por câncer de estômago. Esta mortandade é acompanhada de custos astronômicos dos serviços de saúde, que em 2010 chegaram a US$ 1,6 trilhão.
A incidência cresce em países de renda média e baixa que não têm nem a experiência nem os recursos financeiros para enfrentar a situação. De todos os casos diagnosticados, 60% correspondem a Ásia, África e América do Sul, mesmas regiões onde ocorrem 70% das mortes. Envolverde/IPS









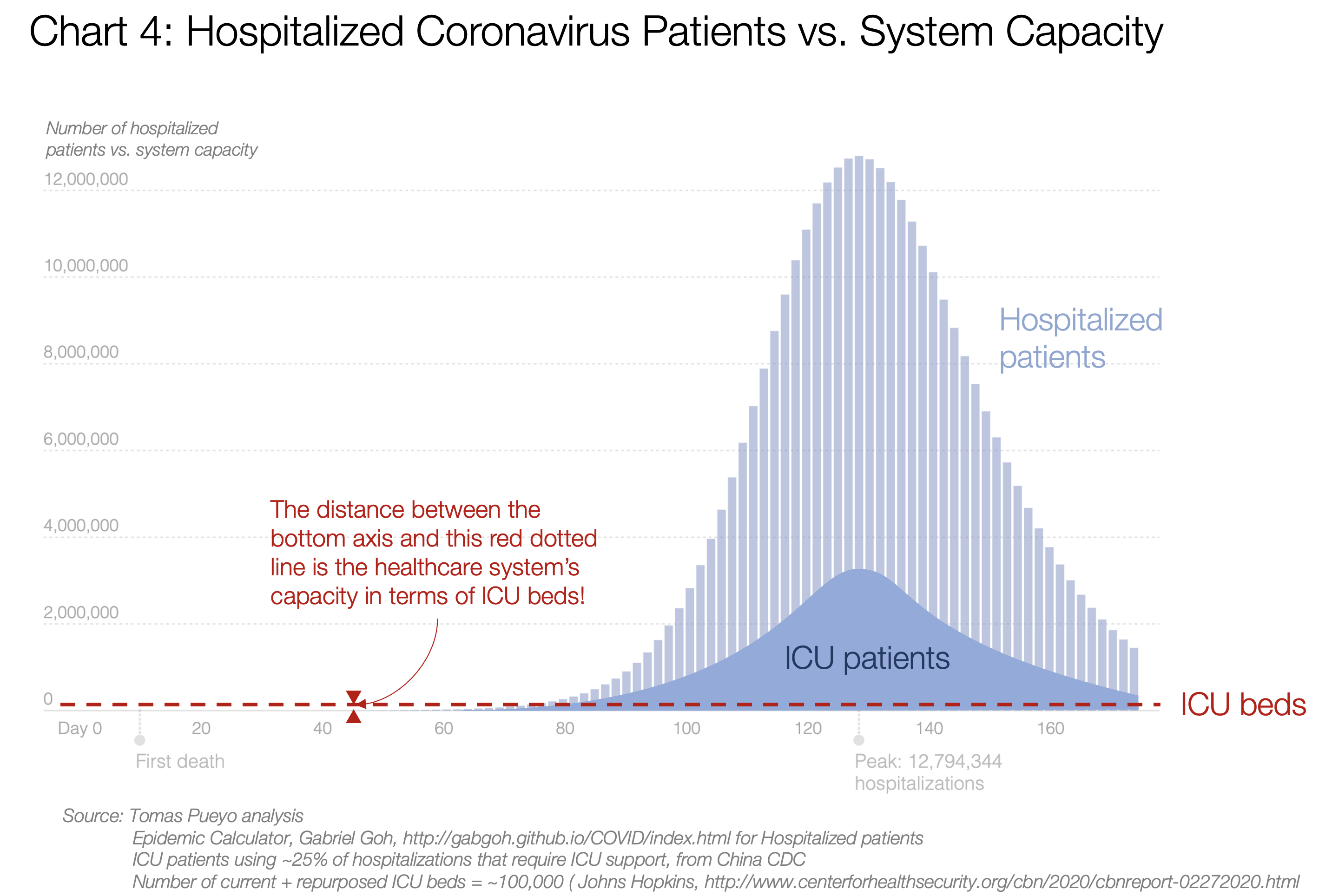

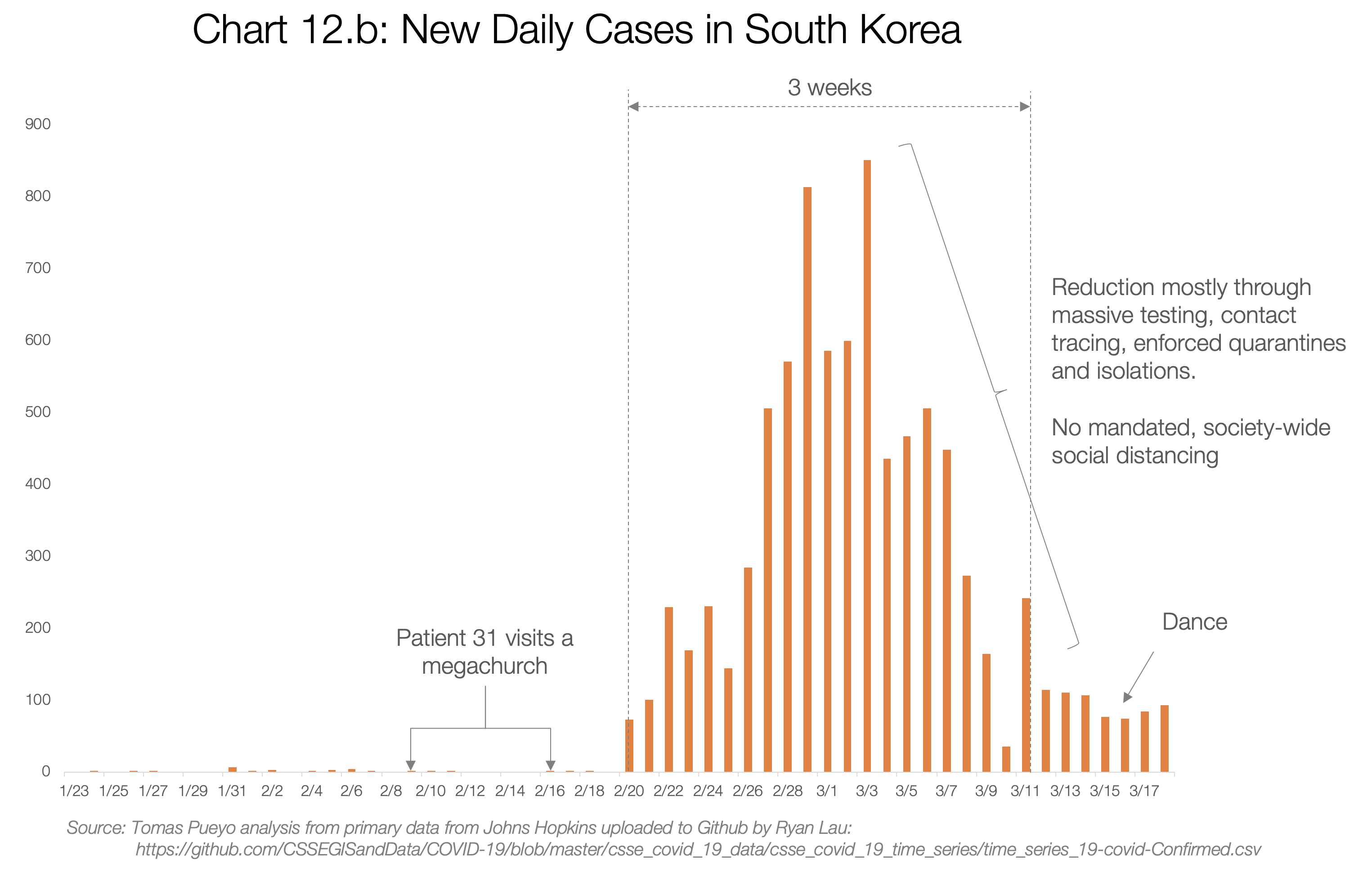
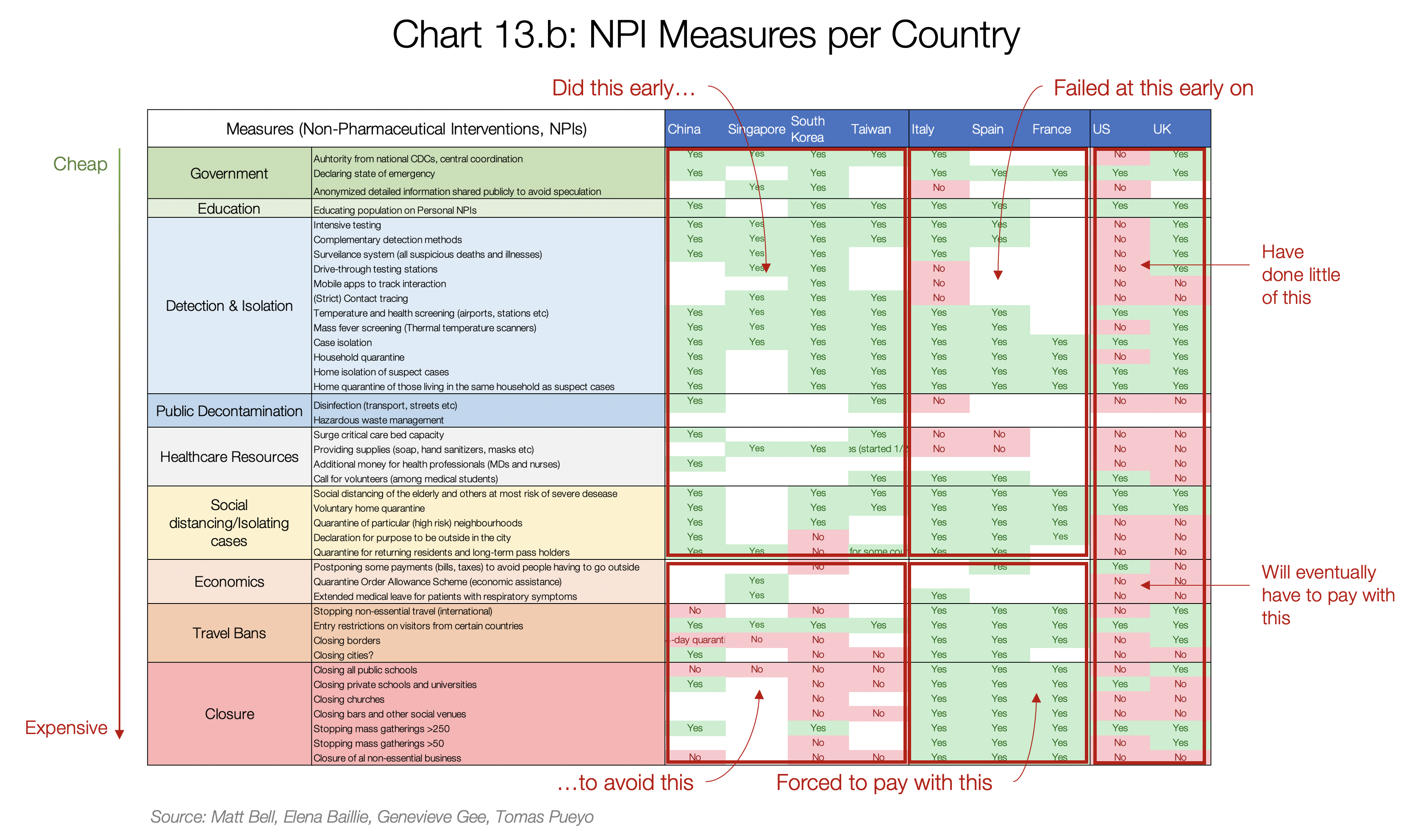

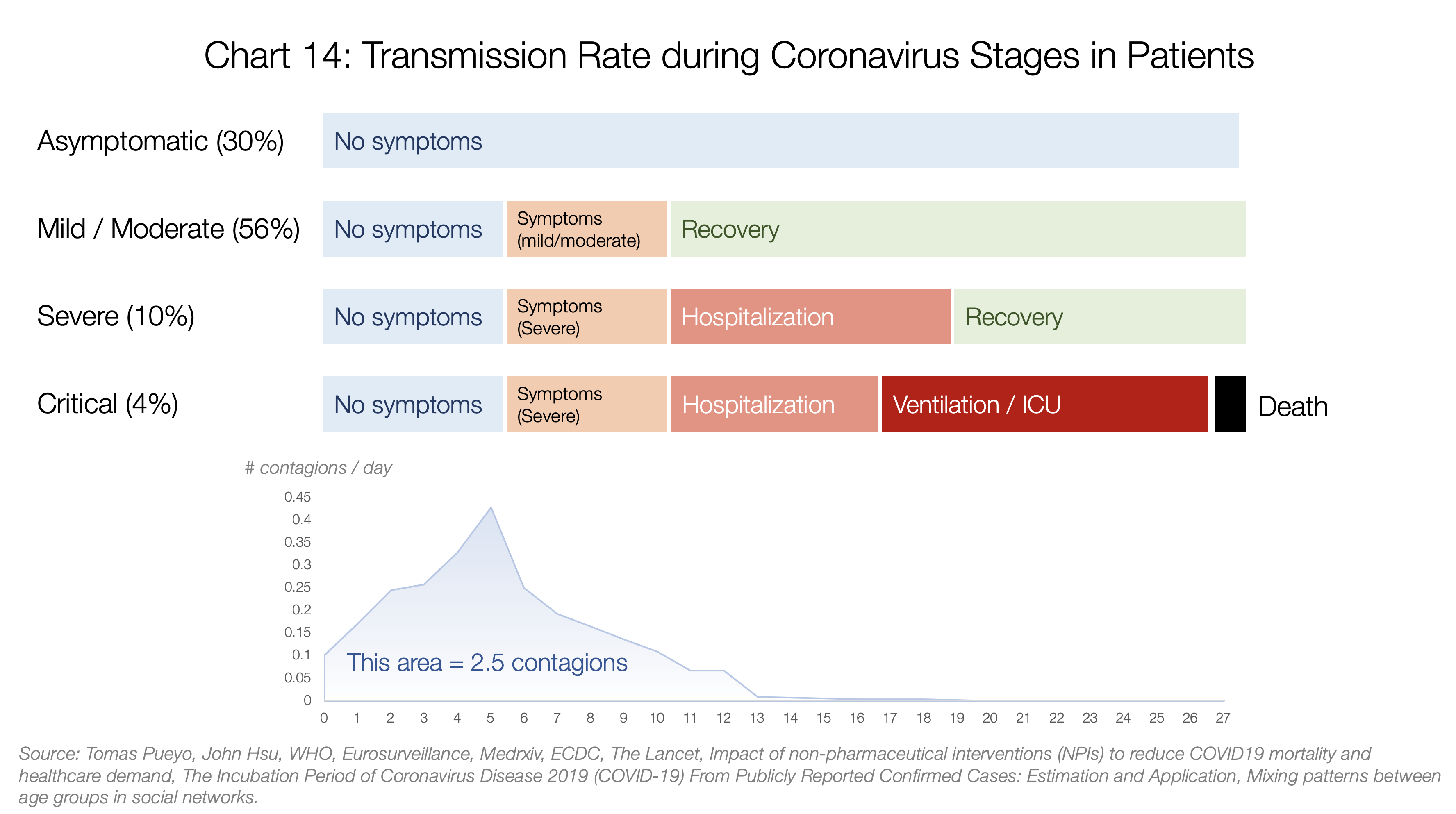
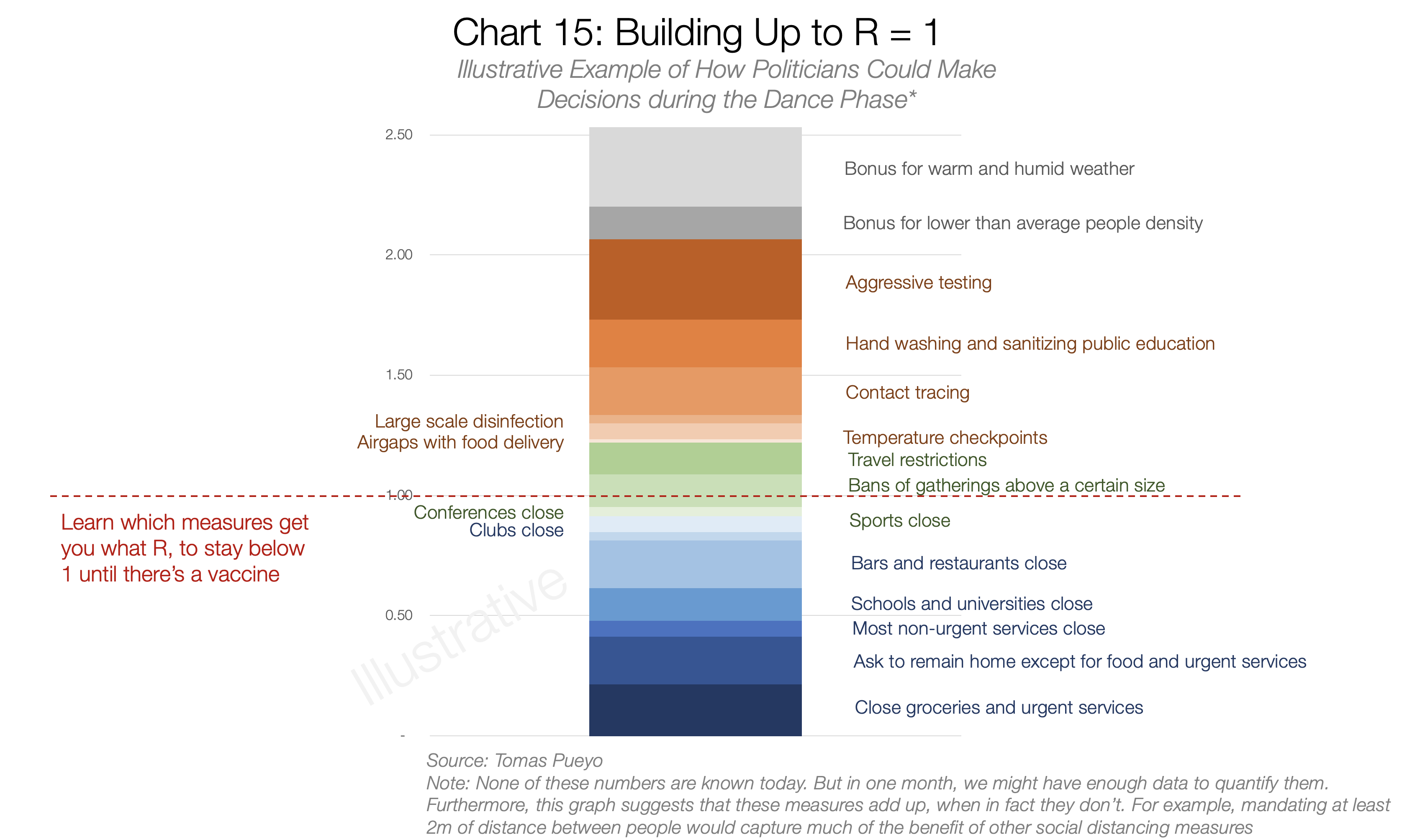








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Você precisa fazer login para comentar.