It was late fall of 2022 when David Stallknecht heard that bodies were raining from the sky.
Stallknecht, a wildlife biologist at the University of Georgia, was already fearing the worst. For months, wood ducks had been washing up on shorelines; black vultures had been teetering out of tree tops. But now thousands of ghostly white snow-goose carcasses were strewn across agricultural fields in Louisiana, Missouri, and Arkansas. The birds had tried to take flight, only to plunge back to the ground. “People were saying they were literally dropping down dead,” Stallknecht told me. Even before he and his team began testing specimens in the lab, they suspected they knew what they would find: yet another crop of casualties from the deadly strain of avian influenza that had been tearing across North America for roughly a year.
Months later, the bird-flu outbreak continues to rage. An estimated 58.4 million domestic birds have died in the United States alone. Farms with known outbreaks have had to cull their chickens en masse, sending the cost of eggs soaring; zoos have herded their birds indoors to shield them from encounters with infected waterfowl. The virus has been steadily trickling into mammalian populations—foxes, bears, mink, whales, seals—on both land and sea, fueling fears that humans could be next. Scientists maintain that the risk of sustained spread among people is very low, but each additional detection of the virus in something warm-blooded and furry hints that the virus is improving its ability to infiltrate new hosts. “Every time that happens, it’s another chance for that virus to make the changes that it needs,” says Richard Webby, a virologist at St. Jude Children’s Research Hospital. “Right now, this virus is a kid in a candy store.”
A human epidemic, though, remains a gloomy forecast that may not come to pass. In the meantime, the outbreak has already been larger, faster-moving, and more devastating to North America’s wildlife than any other in recorded history, and has not yet shown signs of stopping. “I would use just one word to describe it: unprecedented,” says Shayan Sharif, an avian immunologist at Ontario Veterinary College. “We have never seen anything like this before.” This strain of bird flu is unlikely to be our next pandemic. But a flu pandemic has already begun for countless other creatures—and it could alter North America’s biodiversity for good.
Deadly strains of avian flu have been ferried onto North American shores multiple times before, and rapidly petered out. That was the case in 2014, when a highly virulent version of the virus crossed the Pacific from Asia and invaded U.S. poultry farms, forcing workers to exterminate millions of chickens and turkeys. The brutal interventions worked: “They did all the right things, and nipped it in the bud,” says Nicole Nemeth, a veterinary pathologist at the University of Georgia. Hardly any wild birds were affected; egg prices bumped up briefly, then settled back roughly to baseline. “It just kind of died down,” Nemeth told me. “And everyone breathed a sigh of relief.”
Some birds are likely to make it through the outbreak just fine. For as long as humans have been aware of this particular strain of avian influenza, scientifically classed as H5N1, the virus has been relatively gentle on certain types of waterfowl, especially mallards, pintails, and other so-called dabbling ducks. “Some populations have a prevalence as high as 40 percent, and they’re as normal as normal could be,” Stallknecht said. Those same species have also been some of avian flu’s best chauffeurs in the past, silently spreading the feces-borne infection across countries and continents during their seasonal migrations.
Others haven’t been so lucky. Some of the same respiratory issues that strike humans who have the flu—sneezing, coughing, pneumonia when the disease gets severe—can hit birds, too. But across a variety of susceptible species, necropsies show more extensive damage, with evidence of virus in various organs, including the liver, gut, and brain. The neurologic problems can be among the worst: Swans might swim in listless circles; geese might waddle shakily onto shores, their necks twisted and turned; eagles might flap defeatedly from their perches, unable to launch themselves into the air. Michelle Hawkins, a veterinarian at UC Davis, told me that several of the red-tailed hawks she’s treated in her clinic have arrived with their eyes shaking so vigorously from side to side that the spasms turn the animals’ head; others appear to gaze off into nothingness, unresponsive even when humans approach.
Death can come swiftly—sometimes within a day or two of the infection’s start. Birds simply keel over as if they’ve been shot, their bodies dropping like rocks. On poultry farms, outbreaks can wipe out entire flocks in just two or three days. In wilder settings, locals have spotted bald eagles plummeting out of their nests, leaving shrieking chicks behind. By the time infected birds reach Hawkins in her clinic, “they’re usually almost dead,” she told me. “And we can’t figure out how to help them except to put them out of their misery.” Hawkins estimated that in the past few months alone, her team’s euthanasia rate has gone up by about 50 percent.
Mammals so far haven’t fared much better. Last spring, the corpse of a dolphin infected with the virus was found wedged into a canal in Florida—around the same time that Wisconsin locals happened upon litters of ailing fox kits, drooling, twitching, and struggling to stand in the hours before they seized and died. In the fall, three young, flu-stricken grizzlies in Montana were euthanized after researchers noticed that the disoriented animals had begun to go blind. Wendy Puryear, a molecular virologist at Tufts University, told me that seals sick with the virus will sometimes convulse so badly that they can barely hold their bodies straight. Every seal she’s seen that tested positive has ended up dead within days. This month, researchers in Peru reported that they were picking up the virus in some of the sea lions that have died by the hundreds along the country’s coast; a similar situation may now be playing out among a number of Scotland’s seals.
It’s hard to say why this outbreak is so much worse than the ones that came before. Microbial evolution may be one culprit: Flu viruses are particularly inclined to tweak their RNA code; when two genetically distinct versions of the pathogens wind up in the same cell, they can also swap bits of their genomes. This iteration of H5N1 may be particularly adept at sparking lethal disease—something Justin Brown, a veterinary pathologist at Penn State, thinks is quite likely, given how many animals have died. It may also be more easily exiting birds’ bodies in feces, or more efficiently entering cells in the airway or gut. “This particular virus seems to be better adapted to wild birds. I think that’s the key thing,” Stallknecht told me. As climate change alters migration schedules, and pushes certain avian species into more frequent contact with one another’s contaminated scat, the risks of intermingling are only growing. The greater the number of infections, the more animals will die. “It becomes a numbers game,” Stallknecht said.
Flu viruses have never had much trouble spreading: They can be breathed out or defecated; they can persist on surfaces for hours, and in cool waters for days. But Webby suspects that the ballooning of this epidemic can be at least partly blamed on the severity of disease. “The easiest birds to catch are the ones that are sick,” he told me. Hawks, eagles, owls, and other predatory birds may be stumbling across dying ducks and eating them, unwittingly infecting themselves. Nemeth thinks that certain species, including black vultures, are now cutting out the middlebird and feasting on the carcasses of their own kin as they continue to die in droves. “They see dead tissue, they’re going to eat it,” she told me. It’s a morbid tragedy of abundance, as the virus climbs the food chain to reach species it hasn’t easily accessed before. “The biggest impact is on these atypical hosts,” Webby told me, which lack the prior exposures to the virus that might have helped protect them.
Predation or scavenging of sick or dead birds is probably how certain mammals—grizzlies, foxes, opossums, and the like—are catching the virus too. The seals and dolphins present a bit more of a puzzle, Puryear told me, though it’s possible to guess at what’s at play. At least some types of seals have been documented consuming birds; other marine mammals might simply be gulping feces-infested water. A recent avian-flu outbreak at a mink farm in Spain suggests a more troubling mode of transmission: mammals repeatedly conveying the virus to one another—a possible first for H5N1. “That is really disconcerting,” Sharif told me. “It tells me the virus is adapting to mammals.”
Animals vulnerable to the virus don’t have many good options for protection. Some avian-flu vaccines have been used on certain poultry farms, mostly abroad. But some of the same issues that plague human-flu vaccines are obstacles in the bird world too, Brown told me: The ingredients of the shots aren’t always good matches for the circulating virus, and the immunizations, which may be pretty good at staving off severe disease, don’t do much to block infection or transmission, making outbreaks tough to contain. Wild birds, which can’t be corralled and immunized en masse, are essentially out of luck. Nemeth told me that some of her colleagues in Florida have been trying to clear the ground of carcasses so that they won’t become sources of infection for yet another unlucky mammal or bird. “But they just can’t keep up with the number of deaths,” she said. Essentially all avian species are thought to be susceptible to infection—and there’s simply no way to reach every bird, says Becky Poulson, an avian-flu researcher at the University of Georgia. After hopscotching across the globe for decades, H5N1 now seems very likely to be in North America for good, “part of the new normal here,” Poulson told me.
Experts told me they’re hopeful that the outbreak will abate before long. But even if that happens, some species may not live to see it. North America’s birds already face a medley of threats—chemical pollution, window collisions, habitat destruction, roving colonies of feral cats—and some of them cannot sustain another blow. “This could be the last nail in the coffin for some species,” says Min Huang, who leads the migratory-bird program at Connecticut’s Department of Energy and Environmental Protection.
The current epidemic “may not be directly affecting us, in that almost none of us are getting sick,” says Kishana Taylor, a virologist at Rutgers University. But the extent of its reach into wildlife means that humans will still notice its many impacts. In a world with fewer birds, other animals—such as coyotes, snakes, and even humans—might go hungrier, while the fish, insects, and rats that birds eat could experience population booms. The treetops and shorelines, once alive with song, could go silent; far fewer seeds might be dispersed. The U.S.’s national bird—one of the country’s few conservation success stories—could once again find itself pushed to the brink. Some locals in the Southeast have already told Nemeth that they’re feeling the absence of vultures, as roadside deer carcasses begin to fester in the sun. The bird pandemic will have its survivors. But they are likely to be living in a world that is quieter, lonelier, and harsher than it was before.
New antibody and antiviral treatments, and better vaccines, are on the way
The Economist – Nov 8th 2021
IN THE WELL-VACCINATED wealthier countries of the world, year three of the pandemic will be better than year two, and covid-19 will have much less impact on health and everyday activities. Vaccines have weakened the link between cases and deaths in countries such as Britain and Israel (see chart). But in countries that are poorer, less well vaccinated or both, the deleterious effects of the virus will linger. A disparity of outcomes between rich and poor countries will emerge. The Gates Foundation, one of the world’s largest charities, predicts that average incomes will return to their pre-pandemic levels in 90% of advanced economies, compared with only a third of low- and middle-income economies.
Although the supply of vaccines surged in the last quarter of 2021, many countries will remain under-vaccinated for much of 2022, as a result of distribution difficulties and vaccine hesitancy. This will lead to higher rates of death and illness and weaker economic recoveries. The “last mile” problem of vaccine delivery will become painfully apparent as health workers carry vaccines into the planet’s poorest and most remote places. But complaints about unequal distribution will start to abate during 2022 as access to patients’ arms becomes a larger limiting factor than access to jabs. Indeed, if manufacturers do not scale back vaccine production there will be a glut by the second half of the year, predicts Airfinity, a provider of life-sciences data.
Booster jabs will be more widely used in 2022 as countries develop an understanding of when they are needed. New variants will also drive uptake, says Stanley Plotkin of the University of Pennsylvania, inventor of the rubella vaccine. Dr Plotkin says current vaccines and tweaked versions will be used as boosters, enhancing protection against variants.
The vaccination of children will also expand, in some countries to those as young as six months. Where vaccine hesitancy makes it hard for governments to reach their targets they will be inclined to make life difficult for the unvaccinated—by requiring vaccine passports to attend certain venues, and making vaccination compulsory for groups such as health-care workers.
Immunity and treatments may be widespread enough by mid-2022 to drive down case numbers and reduce the risk of new variants. At this point, the virus will become endemic in many countries. But although existing vaccines may be able to suppress the virus, new ones are needed to cut transmission.
Stephane Bancel, the boss of Moderna, a maker of vaccines based on mRNA technology, says his firm is working on a “multivalent” vaccine that will protect against more than one variant of covid-19. Beyond that he is looking at a “pan-respiratory” vaccine combining protection against multiple coronaviruses, respiratory viruses and strains of influenza.
Other innovations in covid-19 vaccines will include freeze-dried formulations of mRNA jabs, and vaccines that are given via skin patches or inhalation. Freeze-dried mRNA vaccines are easy to transport. As the supply of vaccines grows in 2022, those based on mRNA will be increasingly preferred, because they offer higher levels of protection. That will crimp the global market for less effective vaccines, such as the Chinese ones.
In rich countries there will also be greater focus on antibody treatments for people infected with covid-19. America, Britain and other countries will rely more on cocktails such as those from Regeneron or AstraZeneca.
Most promising of all are new antiviral drugs. Pfizer is already manufacturing “significant quantities” of its protease inhibitor. In America, the government has agreed to buy 1.2bn courses of an antiviral drug being developed by Merck, known as molnupiravir. This has shown its efficacy in trials, and the company has licensed it for widespread, affordable production.
There are many other antivirals in the pipeline. Antiviral drugs that can be taken in pill form, after diagnosis, are likely to become blockbusters in 2022, helping make covid-19 an ever more treatable disease. That will lead, in turn, to new concerns about unequal access and of misuse fostering resistant strains.
The greatest risk to this more optimistic outlook is the emergence of a new variant capable of evading the protection provided by existing vaccines. The coronavirus remains a formidable foe.
Natasha Loder: Health-policy editor, The Economist■
This article appeared in the Science and Technology section of the print edition of The World Ahead 2022 under the headline “From pandemic to endemic”
But the taming of the coronavirus conceals failures in public health
The Economist – Nov 8th 2021
PANDEMICS DO NOT die—they fade away. And that is what covid-19 is likely to do in 2022. True, there will be local and seasonal flare-ups, especially in chronically undervaccinated countries. Epidemiologists will also need to watch out for new variants that might be capable of outflanking the immunity provided by vaccines. Even so, over the coming years, as covid settles into its fate as an endemic disease, like flu or the common cold, life in most of the world is likely to return to normal—at least, the post-pandemic normal.
Behind this prospect lie both a stunning success and a depressing failure. The success is that very large numbers of people have been vaccinated and that, at each stage of infection from mild symptoms to intensive care, new medicines can now greatly reduce the risk of death. It is easy to take for granted, but the rapid creation and licensing of so many vaccines and treatments for a new disease is a scientific triumph.
The polio vaccine took 20 years to go from early trials to its first American licence. By the end of 2021, just two years after SARS-CoV-2 was first identified, the world was turning out roughly 1.5bn doses of covid vaccine each month. Airfinity, a life-sciences data firm, predicts that by the end of June 2022 a total of 25bn doses could have been produced. At a summit in September President Joe Biden called for 70% of the world to be fully vaccinated within a year. Supply need not be a constraint.
Immunity has been acquired at a terrible cost
Vaccines do not offer complete protection, however, especially among the elderly. Yet here, too, medical science has risen to the challenge. For example, early symptoms can be treated with molnupiravir, a twice-daily antiviral pill that in trials cut deaths and admissions to hospital by half. The gravely ill can receive dexamethasone, a cheap corticosteroid, which reduces the risk of death by 20-30%. In between are drugs like remdesivir and an antibody cocktail made by Regeneron.
Think of the combination of vaccination and treatment as a series of walls, each of which blocks a proportion of viral attacks from becoming fatal. The erection of each new wall further reduces the lethality of covid.
However, alongside this success is that failure. One further reason why covid will do less harm in the future is that it has already done so much in the past. Very large numbers of people are protected from current variants of covid only because they have already been infected. And many more, particularly in the developing world, will remain unprotected by vaccines or medicines long into 2022.
This immunity has been acquired at terrible cost. The Economist has tracked excess deaths during the pandemic—the mortality over and above what you would have expected in a normal year. Our central estimate on October 22nd was of a global total of 16.5m deaths (with a range from 10.2m to 19.2m), which was 3.3 times larger than the official count. Working backwards using assumptions about the share of fatal infections, a very rough estimate suggests that these deaths are the result of 1.5bn-3.6bn infections—six to 15 times the recorded number.
The combination of infection and vaccination explains why in, say, Britain in the autumn, you could detect antibodies to covid in 93% of adults. People are liable to re-infection, as Britain shows, but with each exposure to the virus the immune system becomes better trained to repel it. Along with new treatments and the fact that more young people are being infected, that explains why the fatality rate in Britain is now only a tenth of what it was at the start of 2021. Other countries will also follow that trajectory on the road to endemicity.
All this could yet be upended by a dangerous new variant. The virus is constantly mutating and the more of it there is in circulation, the greater the chance that an infectious new strain will emerge. However, even if Omicron and Rho variants strike, they may be no more deadly than Delta is. In addition, existing treatments are likely to remain effective, and vaccines can rapidly be tweaked to take account of the virus’s mutations.
Just another endemic disease
Increasingly, therefore, people will die from covid because they are elderly or infirm, or they are unvaccinated or cannot afford medicines. Sometimes people will remain vulnerable because they refuse to have a jab when offered one—a failure of health education. But vaccine doses are also being hoarded by rich countries, and getting needles into arms in poor and remote places is hard. Livelihoods will be ruined and lives lost all for lack of a safe injection that costs just a few dollars.
Covid is not done yet. But by 2023, it will no longer be a life-threatening disease for most people in the developed world. It will still pose a deadly danger to billions in the poor world. But the same is, sadly, true of many other conditions. Covid will be well on the way to becoming just another disease.
Edward Carr: Deputy editor, The Economist■
This article appeared in the Leaders section of the print edition of The World Ahead 2022 under the headline “Burning out”
O Harvard Global Health Institute e o Center for Climate, Health, and the Global Environment, da escola de saúde pública de Harvard, reuniram pesquisadores para analisar a literatura científica disponível até o momento e apontar caminhos para prevenção de novas pandemias.
Um dos pontos citados diretamente pelo relatório é o desmatamento. Os cientistas apontam como exemplo o aumento, após processos de desmate na América Central, de roedores como reservatórios de hantavírus —que, em caso de contaminação de humanos, pode levar à síndrome pulmonar por hantavírus.
A expansão de áreas agricultáveis também está ligada ao surgimento de novas doenças. Isso ocorre, afirmam os pesquisadores, pelo potencial de tal ação aproximar humanos a rebanhos de animais silvestres.
“Cerca de 22% da área terrestre em hotspots de biodiversidade, muitas vezes sobrepostos a hotspots de doenças emergentes, é ameaçada por expansão agrícola”, afirma o documento.
O relatório aponta que processos de urbanização descontrolados e sem planejamento podem ter um papel no surgimento de doenças, pelas mudanças no uso de terra e por possíveis grandes concentrações de pessoas e condições de vida ruins.
Há ainda fazendas de animais como outro ponto importante em eventos de spillover, ou transbordamento, em tradução do inglês, de zoonoses —basicamente, quando um vírus salta de uma espécie para uma nova, como para humanos. Os pesquisadores apontam a baixa diversidade genética e o elevado número de animais mantidos em alguns desses locais.
Os cientistas dão como exemplo a transmissão —inicialmente entre suínos e depois para trabalhadores agrícolas— do vírus nipah, na Malásia, em fazendas de porcos com altas concentrações de animais.
Além disso, a caça, o consumo e o comércio de animais selvagens também podem provocar o spillover.
A crise climática é mais um fator que deve impactar nos riscos de aparecimento de novas doenças no mundo, considerando as alterações que ocorrerão em ecossistemas. Segundo os pesquisadores, existe a possibilidade de habitats adequados para espécies diminuírem, o que poderia promover mais encontros entre vida selvagem e humanos, e, com isso, mais eventos de spillover.
“A redução de habitats e disponibilidade de néctar para morcegos, por exemplo, têm pressionado esses animais a buscar fontes alternativas de alimento em áreas urbanas e arredores”, afirmam os cientistas no relatório.
Por fim, os pesquisadores convocados por Harvard apontam estratégias para evitar eventos de spillover. A conservação ambiental é a primeira a ser destacada no relatório.
Outras estratégias listadas são restrições ao consumo de animais selvagens, investigações sobre vírus na vida selvagem e uma rede global de vigilância de patógenos em humanos, animais criados para abate e vida silvestre, entre outras iniciativas.
Segundo o documento, são baixos os investimentos destinados a impedir spillover. “Não mais do que US$ 4 bilhões [R$ 21,5 bilhões] são gastos a cada ano em todo o mundo em atividades de prevenção de transbordamento. A Covid-19 sozinha resultou em uma perda de PIB global estimada em US$ 4 trilhões [R$ 21,5 trilhões], ou cerca de US$ 40 bilhões [R$ 215 bilhões] por ano durante um século”, aponta o relatório.
RIO DE JANEIRO — Rail-thin teenagers hold placards at traffic stops with the word for hunger — fome — in large print. Children, many of whom have been out of school for over a year, beg for food outside supermarkets and restaurants. Entire families huddle in flimsy encampments on sidewalks, asking for baby formula, crackers, anything.
A year into the pandemic, millions of Brazilians are going hungry.
The scenes, which have proliferated in the last months on Brazil’s streets, are stark evidence that President Jair Bolsonaro’s bet that he could protect the country’s economy by resisting public health policies intended to curb the virus has failed.
From the start of the outbreak, Brazil’s president has been skeptical of the disease’s impact, and scorned the guidance of health experts, arguing that the economic damage wrought by the lockdowns, business closures and mobility restrictions they recommended would be a bigger threat than the pandemic to the country’s weak economy.
The virus is ripping through the social fabric, setting wrenching records, while the worsening health crisis pushes businesses into bankruptcy, killing jobs and further hampering an economy that has grown little or not at all for more than six years.
Daniela dos Santos cooking a meal in downtown São Paulo. The pandemic aggravated Brazil’s economic crisis, increasing the rolls of the unemployed and the homeless.Volunteers distributing sandwiches and soup.
Last year, emergency government cash payments helped put food on the table for millions of Brazilians — but when the money was scaled back sharply this year, with a debt crisis looming, many pantries were left bare.
And about 117 million people, or roughly 55 percent of the country’s population, faced food insecurity, with uncertain access to enough nutrition, in 2020 — a leap from the 85 million who did so two years previous, the study showed.
“The way the government has handled the virus has deepened poverty and inequality,” said Douglas Belchior, the founder of UNEafro Brasil, one of a handful of organizations that have banded together to raise money to get food baskets to vulnerable communities. “Hunger is a serious and intractable problem in Brazil.”
Luana de Souza, 32, was one of several mothers who lined up outside an improvised food pantry on a recent afternoon hoping to score a sack with beans, rice and cooking oil. Her husband had worked for a company that organized events, but lost his job last year — one of eight million people who joined Brazil’s unemployment rolls during the pandemic, driving the rate above 14 percent, according to Brazil’s Institute of Geography and Statistics.
At first the family managed by spending their government assistance carefully, she said, but this year, once the payments were cut, they struggled.
“There is no work,” she said. “And the bills keep coming.”
Ismael dos Santos asks drivers for change at a traffic light.Members of an evangelical church serving breakfast.
Brazil’s economy had gone into recession in 2014, and had not recovered when the pandemic hit. Mr. Bolsonaro often invoked the reality of families like Ms. de Souza’s, who cannot afford to stay home without working, to argue that the type of lockdowns governments in Europe and other wealthy nations ordered to curb the spread of the virus were untenable in Brazil.
Last year, as governors and mayors around Brazil signed decrees shutting down nonessential businesses and restricting mobility, Mr. Bolsonaro called those measures “extreme” and warned that they would result in malnutrition.
As a second wave of cases this year led to the collapse of the health care system in several cities, local officials again imposed a raft of strict measures — and found themselves at war with Mr. Bolsonaro.
“People have to have freedom, the right to work,” he said last month, calling the new quarantine measures imposed by local governments tantamount to living in a “dictatorship.”
Early this month, as the daily death toll from the virus sometimes surpassed 4,000, Mr. Bolsonaro acknowledged the severity of the humanitarian crisis facing his country. But he took no responsibility and instead faulted local officials.
“Brazil is at the limit,” he said, arguing that the blame lay with “whoever closed everything.”
But economists said that the argument that restrictions intended to control the virus would worsen Brazil’s economic downturn was “a false dilemma.”
In an open letter addressed to Brazilian authorities in late March, more than 1,500 economists and businesspeople asked the government to impose stricter measures, including lockdown.
“It is not reasonable to expect economic activity to recover from an uncontrolled epidemic,” the experts wrote.
Laura Carvalho, an economist, published a study showing that restrictions can have a negative short-term impact on a country’s financial health, but that, in the long run, it would have been a better strategy.
“If Bolsonaro had carried out lockdown measures, we would have moved earlier from the economic crisis,” said Ms. Carvalho, a professor at the University of São Paulo.
Mr. Bolsonaro’s approach had a broadly destabilizing effect, said Thomas Conti, lecturer at Insper, a business school.
“The Brazilian real was the most devalued currency among all developing countries,” Mr. Conti said. “We are at an alarming level of unemployment, there is no predictability to the future of the country, budget rules are being violated, and inflation grows nonstop.”
Evangelical church members performing baptisms while distributing food.Volunteers with a Catholic charity preparing meals for the hungry in São Paulo.
The country’s worsening Covid-19 crisis has left Mr. Bolsonaro politically vulnerable. The Senate this month began an inquiry into the government’s handling of the pandemic. The study is expected to document missteps, including the government’s endorsement of drugs that are ineffective to treat Covid-19 and shortages of basic medical supplies, including oxygen. Some of those missteps are likely to be blamed for preventable deaths.
Creomar de Souza, a political analyst and the founder of the consultancy Dharma Politics in Brasília, said the president underestimated the threat the pandemic posed to the country and failed to put together a comprehensive plan to address it.
“They thought it wouldn’t be something serious and figured that the health system would be able to handle it,” he said.
Mr. de Souza said Mr. Bolsonaro has always campaigned and governed combatively, appealing to voters by presenting himself as an alternative to dangerous rivals. His response to the pandemic has been consistent with that playbook, he said.
“The great loss, in addition to the increasing number of victims in this tragedy, is an erosion of governance,” he said. “We’re facing a scenario of high volatility, with a lot of political risks, because the government didn’t deliver on public policies.”
Advocacy and human rights organizations earlier this year started a campaign called Tem Gente Com Fome, or People are Going Hungry, with the aim of raising money from companies and individuals to get food baskets to needy people across the country.
Mr. Belchior, one of the founders, said the campaign was named after a poem by the writer and artist Solano Trindade. It describes scenes of misery viewed as a train in Rio de Janeiro makes its way across poor neighborhoods where the state has been all but absent for decades.
“Families are increasingly pleading for earlier food deliveries,” said Mr. Belchior. “And they’re depending more on community actions than the government.”
Waiting in line for food to be handed out.Joaquim Ribeiro searching for recyclable materials to sell.
Carine Lopes, 32, the president of a community ballet school in Manguinhos, a low-income, working-class district of Rio de Janeiro, has responded to the crisis by turning her organization into an impromptu relief center.
Since the beginning of the pandemic, the price of basic products rose dramatically at nearby stores, she said. The cost of cooking oil more than tripled. A kilogram of rice goes for twice as much. As meat became increasingly prohibitive, Sunday outdoor cookouts became a rarity in the neighborhood.
Long used to fielding calls from parents who desperately wanted a slot for their children at the ballet school, Ms. Lopes has gotten used to a very different appeal. Old acquaintances and strangers text her daily asking about the food baskets the ballet school has been distributing weekly.
“These moms and dads are only thinking about basic things now,” she said. “They call and say: ‘I’m unemployed. I don’t have anything else to eat this week. Is there anything you can give us?’”
When the virus finally recedes, the poorest families will have the hardest time bouncing back, she said.
Ms. Lopes despairs thinking of students who have been unable to tune in to online classes in households that have no internet connection, or where the only device with a screen belongs to a working parent.
“No one will be able to compete for a scholarship with a middle-class student who managed to keep up with classes using their good internet and their tablets,” she said. “Inequality is being exacerbated.”
Handing out food baskets.
Ernesto Londoño is the Brazil bureau chief, based in Rio de Janeiro. He was previously an editorial writer and, before joining The Times in 2014, reported for The Washington Post.
Despite warnings, American and European officials gave up leverage that could have guaranteed access for billions of people. That risks prolonging the pandemic.
Credit: Joao Silva/The New York Times
In the coming days, a patent will finally be issued on a five-year-old invention, a feat of molecular engineering that is at the heart of at least five major Covid-19 vaccines. And the United States government will control that patent.
The new patent presents an opportunity — and some argue the last best chance — to exact leverage over the drug companies producing the vaccines and pressure them to expand access to less affluent countries.
The question is whether the government will do anything at all.
The rapid development of Covid-19 vaccines, achieved at record speed and financed by massive public funding in the United States, the European Union and Britain, represents a great triumph of the pandemic. Governments partnered with drugmakers, pouring in billions of dollars to procure raw materials, finance clinical trials and retrofit factories. Billions more were committed to buy the finished product.
But this Western success has created stark inequity. Residents of wealthy and middle-income countries have received about 90 percent of the nearly 400 million vaccines delivered so far. Under current projections, many of the rest will have to wait years.
Growing numbers of health officials and advocacy groups worldwide are calling for Western governments to use aggressive powers — most of them rarely or never used before — to force companies to publish vaccine recipes, share their know-how and ramp up manufacturing. Public health advocates have pleaded for help, including asking the Biden administration to use its patent to push for broader vaccine access.
Governments have resisted. By partnering with drug companies, Western leaders bought their way to the front of the line. But they also ignored years of warnings — and explicit calls from the World Health Organization — to include contract language that would have guaranteed doses for poor countries or encouraged companies to share their knowledge and the patents they control.
“It was like a run on toilet paper. Everybody was like, ‘Get out of my way. I’m gonna get that last package of Charmin,’” said Gregg Gonsalves, a Yale epidemiologist. “We just ran for the doses.”
Credit: Lena Mucha for The New York Times
The prospect of billions of people waiting years to be vaccinated poses a health threat to even the richest countries. One example: In Britain, where the vaccine rollout has been strong, health officials are tracking a virus variant that emerged in South Africa, where vaccine coverage is weak. That variant may be able to blunt the effect of vaccines, meaning even vaccinated people might get sick.
Western health officials said they never intended to exclude others. But with their own countries facing massive death tolls, the focus was at home. Patent sharing, they said, simply never came up.
“It was U.S.-centric. It wasn’t anti-global.” said Moncef Slaoui, who was the chief scientific adviser for Operation Warp Speed, a Trump administration program that funded the search for vaccines in the United States. “Everybody was in agreement that vaccine doses, once the U.S. is served, will go elsewhere.”
President Biden and Ursula von der Leyen, the president of the European Union’s executive branch, are reluctant to change course. Mr. Biden has promised to help an Indian company produce about 1 billion doses by the end of 2022 and his administration has donated doses to Mexico and Canada. But he has made it clear that his focus is at home.
“We’re going to start off making sure Americans are taken care of first,” Mr. Biden said recently. “But we’re then going to try and help the rest of the world.”
Pressuring companies to share patents could be seen as undermining innovation, sabotaging drugmakers or picking drawn-out and expensive fights with the very companies digging a way out of the pandemic.
As rich countries fight to keep things as they are, others like South Africa and India have taken the battle to the World Trade Organization, seeking a waiver on patent restrictions for Covid-19 vaccines.
Russia and China, meanwhile, have promised to fill the void as part of their vaccine diplomacy. The Gamaleya Institute in Moscow, for example, has entered into partnerships with producers from Kazakhstan to South Korea, according to data from Airfinity, a science analytics company, and UNICEF. Chinese vaccine makers have reached similar deals in the United Arab Emirates, Brazil and Indonesia.
Credit: Adam Dean for The New York Times
Addressing patents would not, by itself, solve the vaccine imbalance. Retrofitting or constructing factories would take time. More raw materials would need to be manufactured. Regulators would have to approve new assembly lines.
And as with cooking a complicated dish, giving someone a list of ingredients is no substitute to showing them how to make it.
To address these problems, the World Health Organization created a technology pool last year to encourage companies to share know-how with manufacturers in lower-income nations.
Not a single vaccine company has signed up.
“The problem is that the companies don’t want to do it. And the government is just not very tough with the companies,” said James Love, who leads Knowledge Ecology International, a nonprofit.
Drug company executives told European lawmakers recently that they were licensing their vaccines as quickly as possible, but that finding partners with the right technology was challenging.
“They don’t have the equipment,” Moderna’s chief executive, Stéphane Bancel, said. “There is no capacity.”
But manufacturers from Canada to Bangladesh say they can make vaccines — they just lack patent licensing deals. When the price is right, companies have shared secrets with new manufacturers in just months, ramping up production and retrofitting factories.
Credit: Andrew Testa for The New York Times
It helps when the government sweetens the deal. Earlier this month, Mr. Biden announced that the pharmaceutical giant Merck would help make vaccines for its competitor Johnson & Johnson. The government pressured Johnson & Johnson to accept the help and is using wartime procurement powers to secure supplies for the company. It will also pay to retrofit Merck’s production line, with an eye toward making vaccines available to every adult in the United States by May.
Despite the hefty government funding, drug companies control nearly all of the intellectual property and stand to make fortunes off the vaccines. A critical exception is the patent expected to be approved soon — a government-led discovery for manipulating a key coronavirus protein.
This breakthrough, at the center of the 2020 race for a vaccine, actually came years earlier in a National Institutes of Health lab, where an American scientist named Dr. Barney Graham was in pursuit of a medical moonshot.
‘We’d already done everything’
For years, Dr. Graham specialized in the kind of long, expensive research that only governments bankroll. He searched for a key to unlock universal vaccines — genetic blueprints to be used against any of the roughly two dozen viral families that infect humans. When a new virus emerged, scientists could simply tweak the code and quickly make a vaccine.
In 2016, while working on Middle East Respiratory Syndrome, another coronavirus known as MERS, he and his colleagues developed a way to swap a pair of amino acids in the coronavirus spike protein. That bit of molecular engineering, they realized, could be used to develop effective vaccines against any coronavirus. The government, along with its partners at Dartmouth College and the Scripps Research Institute, filed for a patent, which will be issued this month.
When Chinese scientists published the genetic code of the new coronavirus in January 2020, Dr. Graham’s team had their cookbook ready.
“We kind of knew exactly what we had to do,” said Jason McLellan, one of the inventors, who now works at the University of Texas at Austin. “We’d already done everything.”
Dr. Graham was already working with Moderna on a vaccine for another virus when the outbreak in China inspired his team to change focus. “We just flipped it to coronavirus and said, ‘How fast can we go?’” Dr. Graham recalled.
Credit: Pete Marovich for The New York Times
Within a few days, they emailed the vaccine’s genetic blueprint to Moderna to begin manufacturing. By late February, Moderna had produced enough vaccines for government-run clinical trials.
“We did the front end. They did the middle. And we did the back end,” Dr. Graham said.
Exactly who holds patents for which vaccines won’t be sorted out for months or years. But it is clear now that several of today’s vaccines — including those from Moderna, Johnson & Johnson, Novavax, CureVac and Pfizer-BioNTech — rely on the 2016 invention. Of those, only BioNTech has paid the U.S. government to license the technology. The patent is scheduled to be issued March 30.
Patent lawyers and public health advocates say it’s likely that other companies will either have to negotiate a licensing agreement with the government, or face the prospect of a lawsuit worth billions. The government filed such a lawsuit in 2019 against the drugmaker Gilead over H.I.V. medication.
This gives the Biden administration leverage to force companies to share technology and expand worldwide production, said Christopher J. Morten, a New York University law professor specializing in medical patents.
“We can do this the hard way, where we sue you for patent infringement,” he said the government could assert. “Or just play nice with us and license your tech.”
The National Institutes of Health declined to comment on its discussions with the drugmakers but said it did not anticipate a dispute over patent infringement. None of the drug companies responded to repeated questions about the 2016 patent.
Experts said the government has stronger leverage on the Moderna vaccine, which was almost entirely funded by taxpayers. New mRNA vaccines, such as those from Moderna, are relatively easier to manufacture than vaccines that rely on live viruses. Scientists compare it to an old-fashioned cassette player: Try one tape. If it’s not right, just pop in another.
Moderna expects $18.4 billion in vaccine sales this year, but it is the delivery system — the cassette player — that is its most prized secret. Disclosing it could mean giving away the key to the company’s future.
Credit: Mike Kai Chen for The New York Times
“There should be no division in order to win this battle,” President Emmanuel Macron of France said.
Yet European governments had backed their own champions. The European Investment Bank lent nearly $120 million to BioNTech, a German company, and Germany bought a $360 million stake in the biotech firm CureVac after reports that it was being lured to the United States.
“We funded the research, on both sides of the Atlantic,” said Udo Bullmann, a German member of the European Parliament. “You could have agreed on a paragraph that says ‘You are obliged to give it to poor countries in a way that they can afford it.’ Of course you could have.”
A People’s Vaccine
In May, the leaders of Pakistan, Ghana, South Africa and others called for governments to support a “people’s vaccine” that could be quickly manufactured and given for free.
They urged the governing body of the World Health Organization to treat vaccines as “global public goods.”
Though such a declaration would have had no teeth, the Trump administration moved swiftly to block it. Intent on protecting intellectual property, the government said calls for equitable access to vaccines and treatments sent “the wrong message to innovators.”
World leaders ultimately approved a watered-down declaration that recognized extensive immunization — not the vaccines themselves — as a global public good.
That same month, the World Health Organization launched the technology-access pool and called on governments to include clauses in their drug contracts guaranteeing equitable distribution. But the world’s richest nations roundly ignored the call.
In the United States, Operation Warp Speed went on a summertime spending spree, disbursing over $10 billion to handpicked companies and absorbing the financial risks of bringing a vaccine to market.
“Our role was to enable the private sector to be successful,” said Paul Mango, a top adviser to the then health secretary, Alex M. Azar II.
The deals came with few strings attached.
Credit: Philip Cheung for The New York Times
Large chunks of the contracts are redacted and some remain secret. But public records show that the government used unusual contracts that omitted its right to take over intellectual property or influence the price and availability of vaccines. They did not let the government compel companies to share their technology.
British and other European leaders made similar concessions as they ordered enough doses to vaccinate their populations multiple times over.
“You have to write the rules of the game, and the place to do that would have been these funding contracts,” said Ellen ’t Hoen, the director of Medicines Law and Policy, an international research group.
By comparison, one of the world’s largest health financiers, the Bill & Melinda Gates Foundation, includes grant language requiring equitable access to vaccines. As leverage, the organization retains some right to the intellectual property.
Dr. Slaoui, who came to Warp Speed after leading research and development at GlaxoSmithKline, is sympathetic to this idea. But it would have been impractical to demand patent concessions and still deliver on the program’s primary goals of speed and volume, he said.
“I can guarantee you that the agreements with the companies would have been much more complex and taken a much longer time,” he said. The European Union, for example, haggled over price and liability provisions, which delayed the rollout.
In some ways, this was a trip down a trodden path. When the H1N1 “swine flu” pandemic broke out in 2009, the wealthiest countries cornered the global vaccine market and all but locked out the rest of the world.
Experts said at the time that this was a chance to rethink the approach. But the swine flu pandemic fizzled and governments ended up destroying the vaccines they had hoarded. They then forgot to prepare for the future.
The International View
For months, the United States and European Union have blocked a proposal at the World Trade Organization that would waive intellectual property rights for Covid-19 vaccines and treatments. The application, put forward by South Africa and India with support from most developing nations, has been bogged down in procedural hearings.
“Every minute we are deadlocked in the negotiating room, people are dying,” said Mustaqeem De Gama, a South African diplomat who is involved in the talks.
But in Brussels and Washington, leaders are still worried about undermining innovation.
During the presidential campaign, Mr. Biden’s team gathered top intellectual property lawyers to discuss ways to increase vaccine production.
“They were planning on taking the international view on things,” said Ana Santos Rutschman, a Saint Louis University law professor who participated in the sessions.
Most of the options were politically thorny. Among them was the use of a federal law allowing the government to seize a company’s patent and give it to another in order to increase supply. Former campaign advisers say the Biden camp was lukewarm to this proposal and others that called for a broader exercise of its powers.
The administration has instead promised to give $4 billion to Covax, the global vaccine alliance. The European Union has given nearly $1 billion so far. But Covax aims to vaccinate only 20 percent of people in the world’s poorest countries this year, and faces a $2 billion shortfall even to accomplish that.
Credit: Joao Silva/The New York Times
Dr. Graham, the N.I.H. scientist whose team cracked the coronavirus vaccine code for Moderna, said that pandemic preparedness and vaccine development should be international collaborations, not competitions.
“A lot of this would not have happened unless there was a big infusion of government money,” he said.
But governments cannot afford to sabotage companies that need profit to survive.
Dr. Graham has largely moved on from studying the coronavirus. He is searching for a universal flu vaccine, a silver bullet that could prevent all strains of the disease without an annual tweak.
Though he was vaccinated through work, he spent the early part of the year trying to get his wife and grown children onto waiting lists — an ordeal that even one of the key inventors had to endure. “You can imagine how aggravating that is,” he said.
Matina Stevis-Gridneff and Monika Pronczuk contributed reporting.
Lincoln Park in Chicago. Scientists are hopeful, as vaccinations continue and despite the emergence of variants, that we’re past the worst of the pandemic. Credit: Lyndon French for The New York Times
Many scientists are expecting another rise in infections. But this time the surge will be blunted by vaccines and, hopefully, widespread caution. By summer, Americans may be looking at a return to normal life.
Published Feb. 25, 2021Updated Feb. 26, 2021, 12:07 a.m. ET
Across the United States, and the world, the coronavirus seems to be loosening its stranglehold. The deadly curve of cases, hospitalizations and deaths has yo-yoed before, but never has it plunged so steeply and so fast.
Is this it, then? Is this the beginning of the end? After a year of being pummeled by grim statistics and scolded for wanting human contact, many Americans feel a long-promised deliverance is at hand.
Americans will win against the virus and regain many aspects of their pre-pandemic lives, most scientists now believe. Of the 21 interviewed for this article, all were optimistic that the worst of the pandemic is past. This summer, they said, life may begin to seem normal again.
But — of course, there’s always a but — researchers are also worried that Americans, so close to the finish line, may once again underestimate the virus.
So far, the two vaccines authorized in the United States are spectacularly effective, and after a slow start, the vaccination rollout is picking up momentum. A third vaccine is likely to be authorized shortly, adding to the nation’s supply.
But it will be many weeks before vaccinations make a dent in the pandemic. And now the virus is shape-shifting faster than expected, evolving into variants that may partly sidestep the immune system.
The latest variant was discovered in New York City only this week, and another worrisome version is spreading at a rapid pace through California. Scientists say a contagious variant first discovered in Britain will become the dominant form of the virus in the United States by the end of March.
The road back to normalcy is potholed with unknowns: how well vaccines prevent further spread of the virus; whether emerging variants remain susceptible enough to the vaccines; and how quickly the world is immunized, so as to halt further evolution of the virus.
But the greatest ambiguity is human behavior. Can Americans desperate for normalcy keep wearing masks and distancing themselves from family and friends? How much longer can communities keep businesses, offices and schools closed?
Covid-19 deaths will most likely never rise quite as precipitously as in the past, and the worst may be behind us. But if Americans let down their guard too soon — many states are already lifting restrictions — and if the variants spread in the United States as they have elsewhere, another spike in cases may well arrive in the coming weeks.
Scientists call it the fourth wave. The new variants mean “we’re essentially facing a pandemic within a pandemic,” said Adam Kucharski, an epidemiologist at the London School of Hygiene and Tropical Medicine.
The declines are real, but they disguise worrying trends.
Credit: Daniel Dreifuss for The New York Times
The United States has now recorded 500,000 deaths amid the pandemic, a terrible milestone. As of Wednesday morning, at least 28.3 million people have been infected.
But the rate of new infections has tumbled by 35 percent over the past two weeks, according to a database maintained by The New York Times. Hospitalizations are down 31 percent, and deaths have fallen by 16 percent.
Yet the numbers are still at the horrific highs of November, scientists noted. At least 3,210 people died of Covid-19 on Wednesday alone. And there is no guarantee that these rates will continue to decrease.
“Very, very high case numbers are not a good thing, even if the trend is downward,” said Marc Lipsitch, an epidemiologist at the Harvard T.H. Chan School of Public Health in Boston. “Taking the first hint of a downward trend as a reason to reopen is how you get to even higher numbers.”
In late November, for example, Gov. Gina Raimondo of Rhode Island limited social gatherings and some commercial activities in the state. Eight days later, cases began to decline. The trend reversed eight days after the state’s pause lifted on Dec. 20.
The virus’s latest retreat in Rhode Island and most other states, experts said, results from a combination of factors: growing numbers of people with immunity to the virus, either from having been infected or from vaccination; changes in behavior in response to the surges of a few weeks ago; and a dash of seasonality — the effect of temperature and humidity on the survival of the virus.
The vaccines were first rolled out to residents of nursing homes and to the elderly, who are at highest risk of severe illness and death. That may explain some of the current decline in hospitalizations and deaths.
Credit: Joao Silva/The New York Times
But young people drive the spread of the virus, and most of them have not yet been inoculated. And the bulk of the world’s vaccine supply has been bought up by wealthy nations, which have amassed one billion more doses than needed to immunize their populations.
Vaccination cannot explain why cases are dropping even in countries where not a single soul has been immunized, like Honduras, Kazakhstan or Libya. The biggest contributor to the sharp decline in infections is something more mundane, scientists say: behavioral change.
Leaders in the United States and elsewhere stepped up community restrictions after the holiday peaks. But individual choices have also been important, said Lindsay Wiley, an expert in public health law and ethics at American University in Washington.
“People voluntarily change their behavior as they see their local hospital get hit hard, as they hear about outbreaks in their area,” she said. “If that’s the reason that things are improving, then that’s something that can reverse pretty quickly, too.”
The downward curve of infections with the original coronavirus disguises an exponential rise in infections with B.1.1.7, the variant first identified in Britain, according to many researchers.
“We really are seeing two epidemic curves,” said Ashleigh Tuite, an infectious disease modeler at the University of Toronto.
The B.1.1.7 variant is thought to be more contagious and more deadly, and it is expected to become the predominant form of the virus in the United States by late March. The number of cases with the variant in the United States has risen from 76 in 12 states as of Jan. 13 to more than 1,800 in 45 states now. Actual infections may be much higher because of inadequate surveillance efforts in the United States.
Buoyed by the shrinking rates over all, however, governors are lifting restrictions across the United States and are under enormous pressure to reopen completely. Should that occur, B.1.1.7 and the other variants are likely to explode.
“Everybody is tired, and everybody wants things to open up again,” Dr. Tuite said. “Bending to political pressure right now, when things are really headed in the right direction, is going to end up costing us in the long term.”
Another wave may be coming, but it can be minimized.
Credit: Lyndon French for The New York Times
Looking ahead to late March or April, the majority of scientists interviewed by The Times predicted a fourth wave of infections. But they stressed that it is not an inevitable surge, if government officials and individuals maintain precautions for a few more weeks.
A minority of experts were more sanguine, saying they expected powerful vaccines and an expanding rollout to stop the virus. And a few took the middle road.
“We’re at that crossroads, where it could go well or it could go badly,” said Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases.
The vaccines have proved to be more effective than anyone could have hoped, so far preventing serious illness and death in nearly all recipients. At present, about 1.4 million Americans are vaccinated each day. More than 45 million Americans have received at least one dose.
A team of researchers at Fred Hutchinson Cancer Research Center in Seattle tried to calculate the number of vaccinations required per day to avoid a fourth wave. In a model completed before the variants surfaced, the scientists estimated that vaccinating just one million Americans a day would limit the magnitude of the fourth wave.
“But the new variants completely changed that,” said Dr. Joshua T. Schiffer, an infectious disease specialist who led the study. “It’s just very challenging scientifically — the ground is shifting very, very quickly.”
Natalie Dean, a biostatistician at the University of Florida, described herself as “a little more optimistic” than many other researchers. “We would be silly to undersell the vaccines,” she said, noting that they are effective against the fast-spreading B.1.1.7 variant.
But Dr. Dean worried about the forms of the virus detected in South Africa and Brazil that seem less vulnerable to the vaccines made by Pfizer and Moderna. (On Wednesday, Johnson & Johnson reported that its vaccine was relatively effective against the variant found in South Africa.)
Credit: Pete Kiehart for The New York Times
About 50 infections with those two variants have been identified in the United States, but that could change. Because of the variants, scientists do not know how many people who were infected and had recovered are now vulnerable to reinfection.
South Africa and Brazil have reported reinfections with the new variants among people who had recovered from infections with the original version of the virus.
“That makes it a lot harder to say, ‘If we were to get to this level of vaccinations, we’d probably be OK,’” said Sarah Cobey, an evolutionary biologist at the University of Chicago.
Yet the biggest unknown is human behavior, experts said. The sharp drop in cases now may lead to complacency about masks and distancing, and to a wholesale lifting of restrictions on indoor dining, sporting events and more. Or … not.
“The single biggest lesson I’ve learned during the pandemic is that epidemiological modeling struggles with prediction, because so much of it depends on human behavioral factors,” said Carl Bergstrom, a biologist at the University of Washington in Seattle.
Taking into account the counterbalancing rises in both vaccinations and variants, along with the high likelihood that people will stop taking precautions, a fourth wave is highly likely this spring, the majority of experts told The Times.
Kristian Andersen, a virologist at the Scripps Research Institute in San Diego, said he was confident that the number of cases will continue to decline, then plateau in about a month. After mid-March, the curve in new cases will swing upward again.
In early to mid-April, “we’re going to start seeing hospitalizations go up,” he said. “It’s just a question of how much.”
Summer will feel like summer again, sort of.
Credit: Kendrick Brinson for The New York Times
Now the good news.
Despite the uncertainties, the experts predict that the last surge will subside in the United States sometime in the early summer. If the Biden administration can keep its promise to immunize every American adult by the end of the summer, the variants should be no match for the vaccines.
Combine vaccination with natural immunity and the human tendency to head outdoors as weather warms, and “it may not be exactly herd immunity, but maybe it’s sufficient to prevent any large outbreaks,” said Youyang Gu, an independent data scientist, who created some of the most prescient models of the pandemic.
Infections will continue to drop. More important, hospitalizations and deaths will fall to negligible levels — enough, hopefully, to reopen the country.
“Sometimes people lose vision of the fact that vaccines prevent hospitalization and death, which is really actually what most people care about,” said Stefan Baral, an epidemiologist at the Johns Hopkins Bloomberg School of Public Health.
Even as the virus begins its swoon, people may still need to wear masks in public places and maintain social distance, because a significant percent of the population — including children — will not be immunized.
“Assuming that we keep a close eye on things in the summer and don’t go crazy, I think that we could look forward to a summer that is looking more normal, but hopefully in a way that is more carefully monitored than last summer,” said Emma Hodcroft, a molecular epidemiologist at the University of Bern in Switzerland.
Imagine: Groups of vaccinated people will be able to get together for barbecues and play dates, without fear of infecting one another. Beaches, parks and playgrounds will be full of mask-free people. Indoor dining will return, along with movie theaters, bowling alleys and shopping malls — although they may still require masks.
The virus will still be circulating, but the extent will depend in part on how well vaccines prevent not just illness and death, but also transmission. The data on whether vaccines stop the spread of the disease are encouraging, but immunization is unlikely to block transmission entirely.
Credit: Pete Kiehart for The New York Times
“It’s not zero and it’s not 100 — exactly where that number is will be important,” said Shweta Bansal, an infectious disease modeler at Georgetown University. “It needs to be pretty darn high for us to be able to get away with vaccinating anything below 100 percent of the population, so that’s definitely something we’re watching.”
Over the long term — say, a year from now, when all the adults and children in the United States who want a vaccine have received them — will this virus finally be behind us?
Every expert interviewed by The Times said no. Even after the vast majority of the American population has been immunized, the virus will continue to pop up in clusters, taking advantage of pockets of vulnerability. Years from now, the coronavirus may be an annoyance, circulating at low levels, causing modest colds.
Many scientists said their greatest worry post-pandemic was that new variants may turn out to be significantly less susceptible to the vaccines. Billions of people worldwide will remain unprotected, and each infection gives the virus new opportunities to mutate.
“We won’t have useless vaccines. We might have slightly less good vaccines than we have at the moment,” said Andrew Read, an evolutionary microbiologist at Penn State University. “That’s not the end of the world, because we have really good vaccines right now.”
For now, every one of us can help by continuing to be careful for just a few more months, until the curve permanently flattens.
“Just hang in there a little bit longer,” Dr. Tuite said. “There’s a lot of optimism and hope, but I think we need to be prepared for the fact that the next several months are likely to continue to be difficult.”
SAO PAULO (Thomson Reuters Foundation) – As farms expand into the Amazon rainforest, felled trees and expanding pastures may open the way for new Brazilian exports beyond beef and soybeans, researchers say: pandemic diseases.
Changes in the Amazon are driving displaced species of animals, from bats to monkeys to mosquitoes, into new areas, while opening the region to arrivals of more savanna-adapted species, including rodents.
Those shifts, combined with greater human interaction with animals as people move deeper into the forest, is increasing the chances of a virulent virus, bacteria or fungus jumping species, said Adalberto Luís Val a researcher at INPA, the National Institute for Research in the Amazon, based in Manaus.
Climate change, which is driving temperature and rainfall changes, adds to the risks, the biologist said.
“There is a great concern because … there is a displacement of organisms. They try to adapt, face these new challenging scenarios by changing places,” Val told the Thomson Reuters Foundation in a telephone interview.
The Evandro Chagas Institute, a public health research organization in the city of Belém, has identified about 220 different types of viruses in the Amazon, 37 of which can cause diseases in humans and 15 of which have the potential to cause epidemics, the researcher said.
They include a range of different encephalitis varieties as well as West Nile fever and rocio, a Brazilian virus from the same family that produces yellow fever and West Nile, he noted in an article published in May by the Brazilian Academy of Sciences.
Val said he was especially concerned about arboviruses, which can be transmitted by insects such as the mosquitoes that carry dengue fever and Zika.
‘SPILLOVER’
Cecília Andreazzi, a researcher at the Oswaldo Cruz Foundation (FIOCRUZ), a major public health institute in Brazil, said the current surge in deforestation and fires in the Amazon can lead to new meetings between species on the move – each a chance for an existing pathogen to transform or jump species.
The ecologist maps existing infectious agents among Brazil’s animals and constructs mathematical models about how the country’s changing landscape “is influencing the structure of these interactions”.
What she is looking for is likely “spillover” opportunities, when a pathogen in one species could start circulating in another, potentially creating a new disease – as appears to have happened in China with the virus that causes COVID-19, she said.
“Megadiverse countries with high social vulnerability and growing environmental degradation are prone to pathogen spillover from wildlife to humans, and they require policies aimed at avoiding the emergence of zoonoses,” she and other researchers wrote in a letter in The Lancet, a science journal, in September.
Brazil, they said, had already seen “clear warnings” of a growing problem, with the emergence of a Brazilian hemorrhagic fever, rodent-carried hantaviruses, and a mosquito-transmitted arbovirus called oropouche.
Brazil’s Amazon has registered some of the worst fires in a decade this year, as deforestation and invasions of indigenous land grow under right-wing President Jair Bolsonaro, who has urged that the Amazon be developed as a means of fighting poverty.
In a speech before the U.N. General Assembly last month, he angrily denied the existence of fires in the Amazon rainforest, calling them a “lie,” despite data produced by his own government showing thousands of blazes surging across the region.
‘BLAME THE BAT’
João Paulo Lima Barreto, a member of the Tukano indigenous people, said one way of combatting the emergence of new pandemic threats is reviving old knowledge about relationships among living things.
Barreto, who is doing doctoral research on shamanistic knowledge and healing at the Federal University of Amazonas, created Bahserikowi’i, an indigenous medicine center that brings the knowledge of the Upper Rio Negro shamans to Manaus, the Amazon’s largest city.
He has called for indigenous knowledge systems to be taken seriously.
“The model of our relationship with our surroundings is wrong,” he told the Thomson Reuters Foundation in a telephone interview.
“It is very easy for us to blame the bat, to blame the monkey, to blame the pig” when a new disease emerges, Barreto said. “But in fact, the human is causing this, in the relationship that we build with the owners of the space”.
Without adequate preservation of forests, rivers and animals, imbalance and disease are generated, he said, as humans fail to respect nature entities known to shamans as “wai-mahsã”.
Andreazzi said particularly strong disease risks come from converting Amazonian forest into more open, savanna-like pastures and fields, which attract marsupials and also rodents, carriers of hantaviruses.
“If you transform the Amazon into a field, you are creating this niche” and species may expand their ranges to fill it, she said, with “the abundance of these species greatly increasing”.
In the face of deforestation, animals are “relocating, moving. And the pathogen, the virus… is looking for hosts” – a situation that creates “very high adaptive capacity”, she said.
But Andreazzi worries about old diseases, as well as new ones.
As the Amazon changes, new outbreaks of threats such as malaria, leishmaniasis and Chagas disease – transmitted by a “kissing bug” and capable of causing heart damage – have been registered, she said.
“We don’t even need to talk about the new diseases. The old ones already carry great risks,” she added.
Reporting by Fabio Zuker ; editing by Laurie Goering : Please credit the Thomson Reuters Foundation, the charitable arm of Thomson Reuters. Visit news.trust.org/climate
But some things are improving, and it will not go on for ever
Sep 26th 2020
AS THE AUTUMNAL equinox passed, Europe was battening down the hatches for a gruelling winter. Intensive-care wards and hospital beds were filling up in Madrid and Marseille—a city which, a few months ago, thought it had more or less eliminated covid-19. Governments were implementing new restrictions, sometimes, as in England, going back on changes made just a few months ago. The al-fresco life of summer was returning indoors. Talk of a second wave was everywhere.
Across the Atlantic the United States saw its official covid-19 death toll—higher than that of all western Europe put together—break the 200,000 barrier. India, which has seen more than half a million new cases a week for four weeks running, will soon take America’s unenviable laurels as the country with the largest official case count.
The world looks set to see its millionth officially recorded death from covid-19 before the beginning of October. That is more than the World Health Organisation (WHO) recorded as having died from malaria (620,000), suicide (794,000) or HIV/AIDS (954,000) over the whole of 2017, the most recent year for which figures are available.
Those deaths represent just over 3% of the recorded covid-19 cases, which now number over 32m. That tally is itself an underestimate of the number who have actually been infected by SARS–CoV-2, the virus which causes covid 19. Many of the infected do not get sick. Many who do are never seen by any health system.
A better, if still imperfect, sense of how many infections have taken place since the outbreak began at the end of last year can be gleaned from “serosurveys” which scientists and public-health officials have undertaken around the world. These look for antibodies against SARS–CoV-2 in blood samples which may have been taken for other purposes. Their presence reveals past exposure to the virus.
Various things make these surveys inaccurate. They can pick up antibodies against other viruses, inflating their totals—an effect which can differ from place to place, as there are more similar-looking viruses circulating in some regions than in others. They can mislead in the other direction, too. Some tests miss low levels of antibody. Some people (often young ones) fight off the virus without ever producing antibodies and will thus not be recorded as having been infected. As a result, estimates based on serosurveys have to be taken with more than a grain of salt.
But in many countries it would take a small sea’s worth of the stuff to bring the serosurvey figures into line with the official number of cases. The fact that serosurvey data are spotty—there is very little, for example, openly available from China—means it is not possible to calculate the global infection rate directly from the data at hand. But by constructing an empirical relationship between death rates, case rates, average income—a reasonable proxy for intensity of testing—and seropositivity it is possible to impute rates for countries where data are not available and thus estimate a global total.
The graphic on this page shows such an estimate based on 279 serosurveys in 19 countries. It suggests that infections were already running at over 1m a day by the end of January—when the world at large was only just beginning to hear of the virus’s existence. In May the worldwide rate appears to have been more than 5m a day. The uncertainties in the estimate are large, and become greater as you draw close to the present, but all told it finds that somewhere between 500m and 730m people worldwide have been infected—from 6.4% to 9.3% of the world’s population. The WHO has not yet released serosurvey-based estimates of its own, though such work is under way; but it has set an upper bound at 10% of the global population.
As the upper part of the following data panel shows, serosurvey results which can be directly compared with the diagnosed totals are often a great deal bigger. In Germany, where cases have been low and testing thorough, the seropositivity rate was 4.5 times the diagnosed rate in August. In Minnesota a survey carried out in July found a multiplier of seven. A survey completed on August 23rd found a 6.02% seropositivity rate in England, implying a multiplier of 12. A national serosurvey of India conducted from the middle of May to early June found that 0.73% were infected, suggesting a national total of 10m. The number of registered cases at that time was 226,713, giving a multiplier of 44. Such results suggest that a global multiplier of 20 or so is quite possible.
If the disease is far more widespread than it appears, is it proportionately less deadly than official statistics, mainly gathered in rich countries, have made it look? Almost certainly. On the basis of British figures David Spiegelhalter, who studies the public understanding of risk at Cambridge University, has calculated that the risk of death from covid increases by about 13% for every year of age, which means a 65-year-old is 100 times more likely to die than a 25-year-old. And 65-year-olds are not evenly distributed around the world. Last year 20.5% of the EU’s population was over 65, as opposed to just 3% of sub-Saharan Africa’s.
But it is also likely that the number of deaths, like the number of cases, is being seriously undercounted, because many people will have died of the disease without having had a positive test for the virus. One way to get around this is by comparing the number of deaths this year with that which would be predicted on the basis of years past. This “excess mortality” method relies on the idea that, though official statistics may often be silent or misleading as to the cause of death, they are rarely wrong about a death actually having taken place.
The excessive force of destiny
The Economist has gathered all-cause mortality data from countries which report them weekly or monthly, a group which includes most of western Europe, some of Latin America, and a few other large countries, including the United States, Russia and South Africa (see lower part of data panel). Between March and August these countries recorded 580,000 covid-19 deaths but 900,000 excess deaths; the true toll of their share of the pandemic appears to have been 55% greater than the official one. This analysis suggests that America’s official figures underestimate the death toll by 30% or more (America’s Centres for Disease Control and Prevention have provided a similar estimate). This means that the real number of deaths to date is probably a lot closer to 300,000 than 200,000. That is about 10% of the 2.8m Americans who die each year—or, put another way, half the number who succumb to cancer. And there is plenty of 2020 still to go.
Add to all this excess mortality unreported deaths from countries where record keeping is not good enough to allow such assessments and the true death toll for the pandemic may be as high as 2m.
What can be done to slow its further rise? The response to the virus’s original vertiginous ascent was an avalanche of lockdowns; at its greatest extent, around April 10th, at least 3.5bn people were being ordered to stay at home either by national governments or regional ones. The idea was to stop the spread of the disease before health-care systems collapsed beneath its weight, and in this the lockdowns were largely successful. But in themselves they were never a solution. They severely slowed the spread of the disease while they were in place, but they could not stay in place for ever.
Stopping people interacting with each other at all, as lockdowns and limits on the size of gatherings do, is the first of three ways to lower a disease’s reproduction number, R—the number of new cases caused by each existing case. The second is reducing the likelihood that interactions lead to infection; it requires mandated levels of social distancing, hygiene measures and barriers to transmission such as face masks and visors. The third is reducing the time during which an infectious person can interact with people under any conditions. This is achieved by finding people who may recently have been infected and getting them to isolate themselves.
Ensuring that infectious people do not have time to do much infecting requires a fast and thorough test-and-trace system. Some countries, including Canada, China, Germany, Italy, Japan, Singapore and Taiwan, have successfully combined big testing programmes which provide rapid results with a well developed capacity for contact tracing and effective subsequent action. Others have foundered.
Networks and herds
Israel provides a ready example. An early and well-enforced lockdown had the expected effect of reducing new infections. But the time thus bought for developing a test-and-trace system was not well used, and the country’s emergence from lockdown was ill-thought-through. This was in part because the small circle around prime minister Binyamin Netanyahu into which power has been concentrated includes no one with relevant expertise; the health ministry is weak and politicised.
Things have been made worse by the fact that social distancing and barrier methods are being resisted by some parts of society. Synagogues and Torah seminaries in the ultra-Orthodox community and large tribal weddings in the Arab-Israeli community have been major centres of infection. While unhappy countries, like Tolstoy’s unhappy families, all differ, the elements of Israel’s dysfunction have clear parallels elsewhere.
Getting to grips with “superspreader” events is crucial to keeping R low. Close gatherings in confined spaces allow people to be infected dozens at a time. In March almost 100 were infected at a biotech conference in Boston. Many of them spread the virus on: genetic analysis subsequently concluded that 20,000 cases could be traced to that conference.
Nipping such blooms in the bud requires lots of contact tracing. Taiwan’s system logs 15-20 contacts for each person with a positive test. Contact tracers in England register four to five close contacts per positive test; those in France and Spain get just three. It also requires that people be willing to get tested in the first place. In England only 10-30% of people with covid-like symptoms ask for a test through the National Health Service. One of the reasons is that a positive test means self-isolation. Few want to undergo such restrictions, and few are good at abiding by them. In early May a survey in England found that only a fifth of those with covid symptoms had self-isolated as fully as required. The government is now seeking to penalise such breaches with fines of up to £10,000 ($12,800). That will reduce the incentive to get tested in the first place yet further.
As much of Europe comes to terms with the fact that its initial lockdowns have not put an end to its problems, there is increased interest in the Swedish experience. Unlike most of Europe, Sweden never instigated a lockdown, preferring to rely on social distancing. This resulted in a very high death rate compared with that seen in its Nordic neighbours; 58.1 per 100,000, where the rate in Denmark is 11.1, in Finland 6.19 and in Norway 4.93. It is not clear that this high death rate bought Sweden any immediate economic advantage. Its GDP dropped in the second quarter in much the same way as GDPs did elsewhere.
It is possible that by accepting so many deaths upfront Sweden may see fewer of them in the future, for two reasons. One is the phenomenon known, in a rather macabre piece of jargon, as “harvesting”. Those most likely to succumb do so early on, reducing the number of deaths seen later. The other possibility is that Sweden will benefit from a level of herd immunity: once the number of presumably immune survivors in the population grows high enough, the spread of the disease slows down because encounters between the infected and the susceptible become rare. Avoiding lockdown may conceivably have helped with this.
On the other hand, one of the advantages of lockdowns was that they provided time not just for the development of test-and-trace systems but also for doctors to get better at curing the sick. In places with good health systems, getting covid-19 is less risky today than it was six months ago. ISARIC, which researches infectious diseases, has analysed the outcomes for 68,000 patients hospitalised with covid-19; their survival rate increased from 66% in March to 84% in August. The greatest relative gains have been made among the most elderly patients. Survival rates among British people 60 and over who needed intensive care have risen from 39% to 58%.
This is largely a matter of improved case management. Putting patients on oxygen earlier helps. So does reticence about using mechanical ventilators and a greater awareness of the disease’s effects beyond the lungs, such as its tendency to provoke clotting disorders.
Nouvelle vague
As for treatments, two already widely available steroids, dexamethasone and hydrocortisone, increase survival by reducing inflammation. Avigan, a Japanese flu drug, has been found to hasten recovery. Remdesivir, a drug designed to fight other viruses, and convalescent plasma, which provides patients with antibodies from people who have already recovered from the disease, seem to offer marginal benefits.
Many consider antibodies tailor-made for the job by biotech companies a better bet; over the past few years they have provided a breakthrough in the treatment of Ebola. The American government has paid $450m for supplies of a promising two-antibody treatment being developed by Regeneron. That will be enough for between 70,000 and 300,000 doses, depending on what stage of the disease the patients who receive it have reached. Regeneron is now working with Roche, another drug company, to crank up production worldwide. But antibodies will remain expensive, and the need to administer them intravenously limits their utility.
It is tempting to look to better treatment for the reason why, although diagnosed cases in Europe have been climbing steeply into what is being seen as a second wave, the number of deaths has not followed: indeed it has, as yet, barely moved. The main reason, though, is simpler. During the first wave little testing was being done, and so many infections were being missed. Now lots of testing is being done, and vastly more infections are being picked up. Correct for this distortion and you see that the first wave was far larger than what is being seen today, which makes today’s lower death rate much less surprising (see data panel).
The coming winter is nevertheless worrying. Exponential growth can bring change quickly when R gets significantly above one. There is abundant evidence of what Katrine Bach Habersaat of the WHO calls “pandemic fatigue” eating away at earlier behavioural change, as well as increasing resentment of other public-health measures. YouGov, a pollster, has been tracking opinion on such matters in countries around the world. It has seen support for quarantining people who have had contact with someone infected fall a bit in Asia and rather more in the West, where it is down from 78% to 63%. In America it has fallen to 55%.
It is true that infection rates are currently climbing mostly among the young. But the young do not live in bubbles. Recent figures from Bouches-du-Rhône, the French department which includes Marseille, show clearly how a spike of cases in the young becomes, in a few weeks, an increase in cases at all ages.
As the fear of such spikes increases, though, so does the hope that they will not be recurring all that much longer. Pfizer, which has promising vaccine candidate in efficacy trials, has previously said that it will seek regulatory review of preliminary results in October, though new standards at the Food and Drug Administration may not allow it to do so in America quite that soon. Three other candidates, from AstraZeneca, Moderna and J&J, are nipping at Pfizer’s heels. The J&J vaccine is a newcomer; it entered efficacy trials only on September 23rd. But whereas the other vaccines need a booster a month after the first jab, the J&J vaccine is administered just once, which will make the trial quicker; it could have preliminary results in November.
None of the companies will have all the trial data they are planning for until the first quarter of next year. But in emergencies regulators can authorise a vaccine’s use based on interim analysis if it meets a minimum standard (in this case, protection of half those who are vaccinated). Authorisation for use under such conditions would still make such a vaccine more credible than those already in use in China and Russia, neither of which was tested for efficacy at all. But there have been fears that American regulators may, in the run up to the presidential election, set the bar too low. Making an only-just-good-enough vaccine available might see social-distancing collapse and infections increase; alternatively, a perfectly decent vaccine approved in a politically toxic way might not be taken up as widely as it should be.
In either case, though, the practical availability of a vaccine will lag behind any sort of approval. In the long run, billions of doses could be needed. A global coalition of countries known as Covax wants to distribute 2bn by the end of 2021—which will only be enough for 1bn people if the vaccine in question, like Pfizer’s or AstraZeneca’s, needs to be administered twice. The world’s largest manufacturer of vaccines, the Serum Institute in India, recently warned that there will not be enough supplies for universal inoculation until 2024 at the earliest.
Even if everything goes swimmingly, it is hard to see distribution extending beyond a small number of front-line health and care workers this year. But the earlier vaccines are pushed out, the better. The data panel on this page looks at the results of vaccinating earlier versus later in a hypothetical population not that unlike Britain’s. Vaccination at a slower rate which starts earlier sees fewer eventual infections than a much more ambitious campaign started later. At the same time increases in R—which might come about if social distancing and similar measures fall away as vaccination becomes real—make all scenarios worse.
By next winter the covid situation in developed countries should be improved. What level of immunity the vaccines will provide, and for how long, remains to be seen. But few expect none of them to work at all.
Access to the safety thus promised will be unequal, both within countries and between them. Some will see loved ones who might have been vaccinated die because they were not. Minimising such losses will require getting more people vaccinated more quickly than has ever been attempted before. It is a prodigious organisational challenge—and one which, judging by this year’s experience, some governments will handle considerably better than others. ■
This article appeared in the Briefing section of the print edition under the headline “Grim tallies”
Earlier this summer, the Summit supercomputer at Oak Ridge National Lab in Tennessee set about crunching data on more than 40,000 genes from 17,000 genetic samples in an effort to better understand Covid-19. Summit is the second-fastest computer in the world, but the process — which involved analyzing 2.5 billion genetic combinations — still took more than a week.
When Summit was done, researchers analyzed the results. It was, in the words of Dr. Daniel Jacobson, lead researcher and chief scientist for computational systems biology at Oak Ridge, a “eureka moment.” The computer had revealed a new theory about how Covid-19 impacts the body: the bradykinin hypothesis. The hypothesis provides a model that explains many aspects of Covid-19, including some of its most bizarre symptoms. It also suggests 10-plus potential treatments, many of which are already FDA approved. Jacobson’s group published their results in a paper in the journal eLife in early July.
According to the team’s findings, a Covid-19 infection generally begins when the virus enters the body through ACE2 receptors in the nose, (The receptors, which the virus is known to target, are abundant there.) The virus then proceeds through the body, entering cells in other places where ACE2 is also present: the intestines, kidneys, and heart. This likely accounts for at least some of the disease’s cardiac and GI symptoms.
But once Covid-19 has established itself in the body, things start to get really interesting. According to Jacobson’s group, the data Summit analyzed shows that Covid-19 isn’t content to simply infect cells that already express lots of ACE2 receptors. Instead, it actively hijacks the body’s own systems, tricking it into upregulating ACE2 receptors in places where they’re usually expressed at low or medium levels, including the lungs.
In this sense, Covid-19 is like a burglar who slips in your unlocked second-floor window and starts to ransack your house. Once inside, though, they don’t just take your stuff — they also throw open all your doors and windows so their accomplices can rush in and help pillage more efficiently.
The renin–angiotensin system (RAS) controls many aspects of the circulatory system, including the body’s levels of a chemical called bradykinin, which normally helps to regulate blood pressure. According to the team’s analysis, when the virus tweaks the RAS, it causes the body’s mechanisms for regulating bradykinin to go haywire. Bradykinin receptors are resensitized, and the body also stops effectively breaking down bradykinin. (ACE normally degrades bradykinin, but when the virus downregulates it, it can’t do this as effectively.)
The end result, the researchers say, is to release a bradykinin storm — a massive, runaway buildup of bradykinin in the body. According to the bradykinin hypothesis, it’s this storm that is ultimately responsible for many of Covid-19’s deadly effects. Jacobson’s team says in their paper that “the pathology of Covid-19 is likely the result of Bradykinin Storms rather than cytokine storms,” which had been previously identified in Covid-19 patients, but that “the two may be intricately linked.” Other papers had previously identified bradykinin storms as a possible cause of Covid-19’s pathologies.
Covid-19 is like a burglar who slips in your unlocked second-floor window and starts to ransack your house.
As bradykinin builds up in the body, it dramatically increases vascular permeability. In short, it makes your blood vessels leaky. This aligns with recent clinical data, which increasingly views Covid-19 primarily as a vascular disease, rather than a respiratory one. But Covid-19 still has a massive effect on the lungs. As blood vessels start to leak due to a bradykinin storm, the researchers say, the lungs can fill with fluid. Immune cells also leak out into the lungs, Jacobson’s team found, causing inflammation.
And Covid-19 has another especially insidious trick. Through another pathway, the team’s data shows, it increases production of hyaluronic acid (HLA) in the lungs. HLA is often used in soaps and lotions for its ability to absorb more than 1,000 times its weight in fluid. When it combines with fluid leaking into the lungs, the results are disastrous: It forms a hydrogel, which can fill the lungs in some patients. According to Jacobson, once this happens, “it’s like trying to breathe through Jell-O.”
This may explain why ventilators have proven less effective in treating advanced Covid-19 than doctors originally expected, based on experiences with other viruses. “It reaches a point where regardless of how much oxygen you pump in, it doesn’t matter, because the alveoli in the lungs are filled with this hydrogel,” Jacobson says. “The lungs become like a water balloon.” Patients can suffocate even while receiving full breathing support.
The bradykinin hypothesis also extends to many of Covid-19’s effects on the heart. About one in five hospitalized Covid-19 patients have damage to their hearts, even if they never had cardiac issues before. Some of this is likely due to the virus infecting the heart directly through its ACE2 receptors. But the RAS also controls aspects of cardiac contractions and blood pressure. According to the researchers, bradykinin storms could create arrhythmias and low blood pressure, which are often seen in Covid-19 patients.
The bradykinin hypothesis also accounts for Covid-19’s neurological effects, which are some of the most surprising and concerning elements of the disease. These symptoms (which include dizziness, seizures, delirium, and stroke) are present in as many as half of hospitalized Covid-19 patients. According to Jacobson and his team, MRI studies in France revealed that many Covid-19 patients have evidence of leaky blood vessels in their brains.
Bradykinin — especially at high doses — can also lead to a breakdown of the blood-brain barrier. Under normal circumstances, this barrier acts as a filter between your brain and the rest of your circulatory system. It lets in the nutrients and small molecules that the brain needs to function, while keeping out toxins and pathogens and keeping the brain’s internal environment tightly regulated.
If bradykinin storms cause the blood-brain barrier to break down, this could allow harmful cells and compounds into the brain, leading to inflammation, potential brain damage, and many of the neurological symptoms Covid-19 patients experience. Jacobson told me, “It is a reasonable hypothesis that many of the neurological symptoms in Covid-19 could be due to an excess of bradykinin. It has been reported that bradykinin would indeed be likely to increase the permeability of the blood-brain barrier. In addition, similar neurological symptoms have been observed in other diseases that result from an excess of bradykinin.”
Increased bradykinin levels could also account for other common Covid-19 symptoms. ACE inhibitors — a class of drugs used to treat high blood pressure — have a similar effect on the RAS system as Covid-19, increasing bradykinin levels. In fact, Jacobson and his team note in their paper that “the virus… acts pharmacologically as an ACE inhibitor” — almost directly mirroring the actions of these drugs.
By acting like a natural ACE inhibitor, Covid-19 may be causing the same effects that hypertensive patients sometimes get when they take blood pressure–lowering drugs. ACE inhibitors are known to cause a dry cough and fatigue, two textbook symptoms of Covid-19. And they can potentially increase blood potassium levels, which has also been observed in Covid-19 patients. The similarities between ACE inhibitor side effects and Covid-19 symptoms strengthen the bradykinin hypothesis, the researchers say.
ACE inhibitors are also known to cause a loss of taste and smell. Jacobson stresses, though, that this symptom is more likely due to the virus “affecting the cells surrounding olfactory nerve cells” than the direct effects of bradykinin.
Though still an emerging theory, the bradykinin hypothesis explains several other of Covid-19’s seemingly bizarre symptoms. Jacobson and his team speculate that leaky vasculature caused by bradykinin storms could be responsible for “Covid toes,” a condition involving swollen, bruised toes that some Covid-19 patients experience. Bradykinin can also mess with the thyroid gland, which could produce the thyroid symptoms recently observed in some patients.
The bradykinin hypothesis could also explain some of the broader demographic patterns of the disease’s spread. The researchers note that some aspects of the RAS system are sex-linked, with proteins for several receptors (such as one called TMSB4X) located on the X chromosome. This means that “women… would have twice the levels of this protein than men,” a result borne out by the researchers’ data. In their paper, Jacobson’s team concludes that this “could explain the lower incidence of Covid-19 induced mortality in women.” A genetic quirk of the RAS could be giving women extra protection against the disease.
The bradykinin hypothesis provides a model that “contributes to a better understanding of Covid-19” and “adds novelty to the existing literature,” according to scientists Frank van de Veerdonk, Jos WM van der Meer, and Roger Little, who peer-reviewed the team’s paper. It predicts nearly all the disease’s symptoms, even ones (like bruises on the toes) that at first appear random, and further suggests new treatments for the disease.
As Jacobson and team point out, several drugs target aspects of the RAS and are already FDA approved to treat other conditions. They could arguably be applied to treating Covid-19 as well. Several, like danazol, stanozolol, and ecallantide, reduce bradykinin production and could potentially stop a deadly bradykinin storm. Others, like icatibant, reduce bradykinin signaling and could blunt its effects once it’s already in the body.
Interestingly, Jacobson’s team also suggests vitamin D as a potentially useful Covid-19 drug. The vitamin is involved in the RAS system and could prove helpful by reducing levels of another compound, known as REN. Again, this could stop potentially deadly bradykinin storms from forming. The researchers note that vitamin D has already been shown to help those with Covid-19. The vitamin is readily available over the counter, and around 20% of the population is deficient. If indeed the vitamin proves effective at reducing the severity of bradykinin storms, it could be an easy, relatively safe way to reduce the severity of the virus.
Other compounds could treat symptoms associated with bradykinin storms. Hymecromone, for example, could reduce hyaluronic acid levels, potentially stopping deadly hydrogels from forming in the lungs. And timbetasin could mimic the mechanism that the researchers believe protects women from more severe Covid-19 infections. All of these potential treatments are speculative, of course, and would need to be studied in a rigorous, controlled environment before their effectiveness could be determined and they could be used more broadly.
Covid-19 stands out for both the scale of its global impact and the apparent randomness of its many symptoms. Physicians have struggled to understand the disease and come up with a unified theory for how it works. Though as of yet unproven, the bradykinin hypothesis provides such a theory. And like all good hypotheses, it also provides specific, testable predictions — in this case, actual drugs that could provide relief to real patients.
The researchers are quick to point out that “the testing of any of these pharmaceutical interventions should be done in well-designed clinical trials.” As to the next step in the process, Jacobson is clear: “We have to get this message out.” His team’s finding won’t cure Covid-19. But if the treatments it points to pan out in the clinic, interventions guided by the bradykinin hypothesis could greatly reduce patients’ suffering — and potentially save lives.
Here’s the most depressing map you’re likely to see this week, courtesy of Anthony Fauci, head of the U.S. National Institute of Allergy and Infectious Diseases. The map, packaged in a recent paper co-written by Fauci, showcases the many other emerging diseases besides covid-19 that pose a threat to our health.
The paper, released over the weekend as a preprint in the journal Cell (meaning it may be revised before its final publication), is intended to lay out the environmental and human factors that led to covid-19 erupting on the world stage in late 2019. Fauci’s co-author is David Morens, senior scientific advisor at Office of the Director at NIAID. It’s an educational read, delving into how newly emerging diseases like covid-19 and familiar enemies like influenza can become so dangerous to humankind.
A map showing newly emerging and reemerging infectious diseases that have recently or could someday pose a serious threat to people’s health. The dots indicate where they were discovered or are most relevant currently. Image: Anthony Fauci, David Morens/Cell
Viruses like the flu, for instance, quickly mutate into new strains that can easily swap genes with other flu viruses and pick up just the right assortment of genetic tricks that make them more lethal than the seasonal flu and help them spread widely from person to person. Coronaviruses aren’t quite so erratic, but their ability to infect a wide variety of host species makes them more likely to spill over into people—and that’s the leading theory behind how covid-19 entered the picture.
In fact, it’s more than possible, Fauci and Morens note, that the common cold coronaviruses we have today once caused major and deadly epidemics in the past. Though that could provide some comfort, seeing as these viruses are now relatively harmless, not all dangerous viruses become more tame over time, and those that do often take a long time to mellow out.
That brings us to the aforementioned map, an exhaustive but by no means complete illustration of the emerging and reemerging diseases that have recently caused us trouble or are still plaguing us (the danger of weaponized anthrax is highlighted as a “deliberately emerging” disease). Many of these aren’t particularly likely to become a pandemic, at least at the moment. Ebola, for instance, is highly fatal but remains relatively hard to transmit between people. Bacterial diseases like gonorrhea are worrisome because they’re becoming resistant to antibiotics, but they’re not especially lethal.
Far from being a vanishingly rare event, though, humankind has experienced a pandemic on average every 20 years in the last hundred years, with the last, the H1N1 flu, showing up 10 years ago.
None of this is to say that we’re powerless against the coming germ tide—there’s much we can do to prepare, and in fact, many people predicted something like covid-19 happening as recently as last October. But without learning from our mistakes this time around, there’s no telling just how bad the next pandemic will be.
“Science will surely bring us many life-saving drugs, vaccines, and diagnostics; however, there is no reason to think that these alone can overcome the threat of ever more frequent and deadly emergencies of infectious diseases,” Fauci and Morens wrote. “Covid-19 is among the most vivid wake-up calls in over a century. It should force us to begin to think in earnest and collectively about living in more thoughtful and creative harmony with nature, even as we plan for nature’s inevitable, and always unexpected, surprises.”
Data from those tested at a storefront medical office in Queens is leading to a deeper understanding of the outbreak’s scope in New York.
Credit…Victor J. Blue for The New York Times
July 9, 2020; Updated 7:37 a.m. ET
At a clinic in Corona, a working-class neighborhood in Queens, more than 68 percent of people tested positive for antibodies to the new coronavirus. At another clinic in Jackson Heights, Queens, that number was 56 percent. But at a clinic in Cobble Hill, a mostly white and wealthy neighborhood in Brooklyn, only 13 percent of people tested positive for antibodies.
As it has swept through New York, the coronavirus has exposed stark inequalities in nearly every aspect of city life, from who has been most affected to how the health care system cared for those patients. Many lower-income neighborhoods, where Black and Latino residents make up a large part of the population, were hard hit, while many wealthy neighborhoods suffered much less.
But now, as the city braces for a possible second wave of the virus, some of those vulnerabilities may flip, with the affluent neighborhoods becoming most at risk of a surge. According to antibody test results from CityMD that were shared with The New York Times, some neighborhoods were so exposed to the virus during the peak of the epidemic in March and April that they might have some protection during a second wave.
“Some communities might have herd immunity,” said Dr. Daniel Frogel, a senior vice president for operations at CityMD, which plays a key role in the city’s testing program.
The CityMD statistics — which Dr. Frogel provided during an interview and which reflect tests done between late April and late June — appear to present the starkest picture yet of how infection rates have diverged across neighborhoods in the city.
As of June 26, CityMD had administered about 314,000 antibody tests in New York City. Citywide, 26 percent of the tests came back positive.
But Dr. Frogel said the testing results in Jackson Heights and Corona seemed to “jump off the map.”
While stopping short of predicting that those neighborhoods would be protected against a major new outbreak of the virus — a phenomenon known as herd immunity — several epidemiologists said that the different levels of antibody prevalence across the city are likely to play a role in what happens next, assuming that antibodies do in fact offer significant protection against future infection.
“In the future, the infection rate should really be lower in minority communities,” said Kitaw Demissie, an epidemiologist and the dean of the School of Public Health at SUNY Downstate Medical Center in Brooklyn.
Dr. Ted Long, the executive director of the city’s contact-tracing program, said that while much remained unknown about the strength and duration of the protection that antibodies offer, he was hopeful that hard-hit communities like Corona would have some degree of protection because of their high rate of positive tests. “We hope that that will confer greater herd immunity,” he said.
Neighborhoods that had relatively low infection rates — and where few residents have antibodies — are especially vulnerable going forward. There could be some degree of “catch up” among neighborhoods, said Prof. Denis Nash, an epidemiology professor at the CUNY School of Public Health.
But he added that even if infection rate were to climb in wealthier neighborhoods, “there are advantages to being in the neighborhoods that are hit later.” For one, doctors have become somewhat more adept at treating severe cases.
Credit…Brittainy Newman/The New York Times
Some epidemiologists and virologists cautioned that not enough data exists to conclude that any areas have herd immunity. For starters, the fact that 68.4 percent of tests taken at an urgent care center in Corona came back positive does not mean that 68.4 percent of residents had been infected.
“For sure, the persons who are seeking antibody testing probably have a higher likelihood of being positive than the general population,” said Professor Nash. “If you went out in Corona and tested a representative sample, it wouldn’t be 68 percent.”
So far, the federal government has released relatively little data from antibody testing — making the CityMD data all the more striking. The Centers for Disease Control and Prevention, for instance, has published limited data that suggested that 6.93 percent of residents in New York City and part of Long Island had antibodies. But that survey was based on samples collected mainly in March, before many infected New Yorkers might have developed antibodies.
New York State conducted a more comprehensive survey on antibody rates, which involved testing some 28,419 people across the state. That survey suggested that roughly 21.6 percent of New York City residents had antibodies. But it also revealed a much higher rate in some neighborhoods. While the state has released little data from Queens, its numbers showed that in Flatbush, Brooklyn, for example, about 45 percent of those tested had antibodies.
The CityMD data provides similar conclusions. At a location in Bushwick, a Brooklyn neighborhood which has a large Hispanic population and where the median household income is below the citywide average, some 35 percent of antibody tests were positive, according to Dr. Frogel.
Credit…Juan Arredondo for The New York Times
Dr. Frogel said that across the Bronx, which has had the city’s highest death rate from Covid-19, about 37 percent of antibody tests were turning up positive.
The CityMD in Corona, on Junction Boulevard, serves a predominantly Hispanic neighborhood whose residents include many construction workers and restaurant employees. Many had to work throughout the pandemic, raising their risk of infection.
Angela Rasmussen, a virologist at Columbia University, called the high positive rate in Corona “a stunning finding.” Epidemiologists said the rate showed the limits of New York’s strategy in curtailing the virus: While public health measures may have slowed the spread in some neighborhoods, they did far less for others.
For residents of Corona, the main sources of employment are jobs in hospitality, including restaurants, as well as construction and manufacturing, according to a 2019 report by the Citizens’ Committee for Children of New York. Many construction workers and restaurant employees showed up to work throughout the pandemic, elevating their risk of infection.
“Our plan did not really accommodate essential workers as it did people privileged enough — for lack of a better word — to socially distance themselves,” Professor Nash said. He said that one lesson of the past few months was that the city needed to better protect essential workers — everyone from grocery store employees to pharmacy cashiers — and make sure they had sufficient protective equipment.
Epidemiologists have estimated that at least 60 percent of a population — and perhaps as much as 80 percent — would need immunity before “herd immunity” is reached, and the virus can no longer spread widely in that community.
But scientists say it would be a mistake to base public health decisions off antibody rates across a population.
“Just looking at seroprevalence alone can’t really be used to make actionable public health decisions,” Dr. Rasmussen, the virologist at Columbia, said.
One reason is that the accuracy of the antibody tests is not fully known, nor is the extent of immunity conferred by antibodies or how long that immunity lasts. Dr. Rasmussen noted that the “magical number of 60 percent for herd immunity” assumes that everyone infected has complete protection from a second infection. “But what about people with partial protection?” she asked. “They may not get sick, but they can get infected and pass it along.”
“It is premature to discuss herd immunity, since we are still learning what the presence of Covid-19 antibodies means to an individual and whether, or for how long, that conveys immunity; and we don’t know how the level of immunity in a single community translates into herd immunity,” said Jonah Bruno, a spokesman for the state Department of Health.
He said he was unsurprised by the high rate in Corona, and senior officials with the city’s contact-tracing program and public hospital system agree. “We know this area was disproportionately affected,” said Dr. Andrew Wallach, a senior official in the city’s public hospital system, “so this just confirms what we’ve seen clinically.”
Joseph Goldstein covers health care in New York, following years of criminal justice and police reporting for the Metro desk. He also spent a year in The Times’ Kabul bureau, reporting on Afghanistan. @JoeKGoldstein
Depoimento concedido a Christina Queiroz. 5 de julho de 2020
“A chegada da Covid-19 causou um impacto muito forte em todos os meus colegas na Universidade Federal do Amazonas [Ufam]. Com minha esposa, estou fazendo um isolamento rigoroso em Manaus, porque tenho quase 60 anos, tomo remédios para controlar pressão e diabetes. Vivemos semanas muito tristes, marcadas por muita dor e sofrimento. Como indígena, sigo perdendo amigos, familiares e lideranças de longa data. Fomos pegos de surpresa. Não acreditávamos na possibilidade de uma tragédia humanitária como essa. Faço parte de uma geração de indígenas que tem fé no poder da ciência, da tecnologia e acredita nos avanços proporcionados pela modernidade. No nosso pensamento, o vírus representa um elemento a mais da natureza. E, por causa da nossa fé no poder da ciência e da medicina científica, não esperávamos uma submissão tão grande da humanidade a um elemento tão pequeno e invisível. Assim, a primeira consequência da chegada da pandemia foi pedagógica e causou reflexões sobre nossa compreensão do mundo e de nós mesmos.
Como pesquisadores acadêmicos, também precisamos ter a humildade de assumir que nos deparamos com os limites da técnica e da ciência. Ter humildade não significa se apequenar, mas, sim, buscar complementar os conhecimentos acadêmicos com outros saberes, para além da ciência eurocêntrica, e isso inclui as ciências indígenas. Ficou evidente o quanto é perigosa a trajetória que a humanidade está tomando, um caminho à deriva, sem lideranças, sem horizonte claro à possibilidade da própria existência humana. Somos uma sociedade que caminha para sua autodestruição. A natureza mostrou sua força, evidenciou que a palavra final é dela, e não dos humanos.
Com o passar das semanas, essa ideia foi sendo incorporada em nossa maneira de compreender, explicar, aceitar e conviver com a nova realidade. Os povos indígenas apresentam cosmovisões milenares, mas que são atualizadas de tempos em tempos, como tem acontecido na situação atual. Passamos a olhar para a nova situação como uma oportunidade para empreender uma revisão cosmológica, filosófica, ontológica e epistemológica da nossa existência e buscar formas pedagógicas para sofrer menos. Nós, indígenas, somos profundamente emotivos. Amamos a vida e nossa existência não é pautada pela materialidade. O momento atual representa uma situação única de formação, pois afeta nossas emoções e valores. Ficamos surpresos com o pouco amor à vida das elites econômicas e de parte dos governantes, mas também de uma parcela significativa da população. A pandemia revelou essas deficiências.
Por outro lado, um dos elementos que emergiu desse processo é uma profunda solidariedade, que tem permitido aos povos indígenas sobreviver no contexto atual. Identificamos fragilidades e limites. Também potencializamos nossas fortalezas. Uma delas, a valorização do conhecimento tradicional, considerado elemento do passado. Redescobrimos o valor do Sistema Único de Saúde [SUS], com toda a fragilidade que foi imposta a ele por diferentes governos. O SUS tem sido um gigante em um momento muito difícil para toda a sociedade.
Coordeno o curso de formação de professores indígenas da Faculdade de Educação da Ufam e me envolvo diariamente em discussões como essas com os alunos. São mais de 300 estudantes que fazem parte desse programa, divididos em cinco turmas. Recentemente, um deles morreu por conta de complicações causadas pelo novo coronavírus. No Amazonas, há mais de 2 mil professores indígenas atuando nas escolas das aldeias. Tenho muito trabalho com atividades burocráticas, para atualizar o registro acadêmico dos alunos e analisar suas pendências. Estamos planejando como fazer a retomada das atividades presenciais de ensino, mas essa retomada só deve acontecer em 2021. Enquanto isso, seminários on-line permitem dar continuidade ao processo de ensino-aprendizagem e ajudam a fomentar a volta de um espírito de solidariedade entre os estudantes indígenas, a valorização da natureza e a recuperação de saberes tradicionais sobre plantas e ervas medicinais. Em condições normais, a possibilidade de participar de tantos seminários e discussões não seria possível. Essas reflexões realizadas durante os encontros virtuais vão se transformar em material didático e textos publicados. Escrever esses textos me ajuda na compreensão da realidade e permite que esse saber seja compartilhado.
Estamos realizando uma pesquisa para identificar quantos alunos do programa dispõem de equipamentos e acesso à internet. Muitos estão isolados em suas aldeias, alguns deles se refugiaram em lugares ainda mais remotos e só acessam a internet em situações raras e pontuais, quando precisam ir até as cidades. Em Manaus, constatamos que apenas 30% dos estudantes da Faculdade de Educação da Ufam dispõem de equipamento pessoal para utilizar a internet. No interior, entre os alunos dos territórios, esse percentual deve ser de menos de 10%. Devemos ter os resultados desse levantamento nas próximas semanas. Sou professor há 30 anos e trabalho com organizações e lideranças indígenas e vejo como esse fator dificulta o planejamento de qualquer atividade remota. Quando tivermos os resultados dessa pesquisa, a ideia é ter uma base de dados para que o movimento indígena se organize para solucionar o problema. Essa situação de ensino remoto pode se prolongar e precisamos estar preparados para não prejudicar os direitos dos alunos e vencer a batalha da inclusão digital.
Há 50 dias, vivíamos o pico da pandemia em Manaus. Estávamos apavorados, com 140 mortes diárias e as pessoas sendo enterradas em valas coletivas. Essa semana foi a primeira que sentimos um alívio. Hoje, 25 de junho, foi o primeiro dia em que nenhuma morte por coronavírus foi registrada na cidade. O medo agora é que pessoas desinformadas, ou menos sensíveis à vida, com o relaxamento das regras de isolamento, provoquem uma segunda onda de contaminação. Percebemos que as pessoas abandonaram as práticas de isolamento e muitas nem sequer utilizam máscaras. Mas começamos a sair do fundo do poço, inclusive o existencial. As estruturas montadas para o caos, como os hospitais de campanha, estão sendo desmontadas.
Tivemos perdas de lideranças e pajés indígenas irreparáveis e insubstituíveis. Com a morte desses sábios, universos de sabedoria milenar desapareceram. Os pajés são responsáveis por produzir e manter o conhecimento tradicional, que só é repassado para alguns poucos herdeiros escolhidos, que precisam ser formados em um processo ritualístico longo e repleto de sacrifícios. As gerações mais jovens apresentam dificuldades para seguir esses protocolos e, por causa disso, o conhecimento tradicional tem enfrentado dificuldades em ser repassado. Eu e meus colegas da Ufam e dos movimentos indígenas estamos incentivando a nova geração a criar estratégias para absorver essa sabedoria, porque muitos sábios seguirão vivos. Escolas e universidades também podem colaborar com o processo, reconhecendo a importância desses saberes. Com os jovens, estamos insistindo que chegou a hora de garantir a continuidade dos saberes tradicionais.
Com a melhoria da situação em Manaus, minha preocupação agora se voltou para o interior, onde foram notificadas 24 mortes nas últimas 24 horas. A população do interior representa menos de 50% da do Amazonas, estado onde as principais vítimas têm sido indígenas, do mesmo modo que acontece em Roraima. Toda minha família vive em São Gabriel da Cachoeira, incluindo minha mãe de 87 anos. A cidade já registrou mais de 3 mil casos e 45 mortes e ainda não atingiu o pico da pandemia. Há cerca de 800 comunidades no entorno do município e sabemos que o vírus já se espalhou por quase todas elas.
Porém há algo que nos alivia. Inicialmente ficamos apavorados, pensando que o vírus causaria um genocídio na população da cidade e seus entornos. O único hospital de São Gabriel não possui leitos de UTI [Unidade de Terapia Intensiva]. Passados 45 dias da notificação do primeiro caso na cidade, apesar das perdas significativas, vemos que as pessoas têm conseguido sobreviver à doença se cuidando em suas próprias casas, com medicina tradicional e fortalecendo laços de solidariedade. Minha mãe ficou doente, apresentou os sintomas da Covid-19. Também meus irmãos e uma sobrinha de minha mãe de 67 anos. Eles não foram testados. Decidiram permanecer em suas casas e cuidar uns dos outros, se valendo de ervas e cascas de árvores da medicina tradicional. Sobreviveram. Sabiam que ir para o hospital lotado naquele momento significaria morrer, pois a estrutura é precária e eles ficariam sozinhos. Ao optar por permanecer em casa, possivelmente transmitiram a doença um ao outro, mas a solidariedade fez a diferença. Um cuidou do outro. Culturalmente, a ideia de isolar o doente é algo impossível para os indígenas, pois seria interpretado como abandono, falta de solidariedade e desumanidade, o que é reprovável. Os laços de solidariedade vão além do medo de se contaminar.”
Todos os anos, os povos do chamado Alto do Xingu, no Parque Nacional do Xingu, passam seis meses se preparando para a festa mais importante do ano, o Kuarup. A celebração que normalmente se estende de julho a setembro é o ritual sagrado no qual todos os mortos do último ano são homenageados. É a maneira que os índios das 11 etnias do Alto Xingu têm de celebrá-los. Com o Kuarup, as famílias que passaram os últimos 12 meses em luto, podem voltar à rotina normal.
Numa decisão histórica ocorrida no início desta semana, em conversas via rádio amador, os caciques das etnias participantes do Kuarup decidiram cancelar o ritual pela primeira vez. Aquilo que já era temido se confirmou: o coronavírus chegou ao Parque do Xingu, reserva indígena no norte do Mato Grosso, com mais de 7.000 habitantes de 16 etnias.
No último fim de semana, o cacique Vanité Kalapalo e seu Yarurú, da aldeia Sapezal, foram internados no Hospital Regional de Água Boa (MT), a 736 Km de Cuiabá, com sintomas agudos da Covid-19.
Outras pessoas da aldeia Sapezal, uma das mais próximas da cidade de Querência (MT), também fizeram testes com suspeita da doença.
O povo Kalapalo foi isolado, mas segundo especialistas e lideranças de outros povos, a previsão é que o coronavírus se espalhe pela primeira grande terra indígena demarcada pelo governo federal, em 1961, e considerada patrimônio nacional.
“O cenário é de possível genocídio”, afirma o médico sanitarista Douglas Rodrigues, da Unifesp (Universidade Federal de São Paulo), que há 40 anos trabalha no Xingu. “Se a taxa de transmissão do vírus seguir em alta como aconteceu nas aldeias da Amazônia, num pior cenário teremos 2.000 infectados e poderemos chegar a cem óbitos.”
Segundo o sanitarista, o potencial de propagação do coronavírus no Xingu dependerá da organização dos próprios índios, da Sesai (Secretaria Especial de Saúde Indígena), do DSEI (Distrito Sanitário Especial Indígena), e da Funai (Fundação Nacional do Índio).
“Mesmo com orientação e avisos sobre a pandemia, pedindo para que a circulação fosse evitada, não foi possível fazer com que alguns índios, principalmente os mais jovens, não deixassem suas aldeias. Parte das pessoas não acreditou no potencial da pandemia, há também desinformação e fake news circulando”, diz Rodrigues. “Também nesta época do ano são comuns surtos de gripe e de infecções respiratórias no parque. Há quase dois meses, quando muitos começaram a ficar doentes em uma das aldeias Kalapalo, pedimos à Sesai testes para Covid-19, mas isso não foi feito. Então não sabemos se a doença chegou ali há mais tempo.”
O professor de antropologia da Unicamp (Universidade Estadual de Campinas), Antonio Guerreiro, que pesquisa os Kalapalo desde 2006, também vê com muita preocupação a chegada do coronavírus ao Xingu e o risco de um possível genocídio.
“Os riscos do coronavírus se espalhar são enormes se compararmos a situação atual com a última grande epidemia que atingiu o Xingu, a de sarampo, em 1954, que dizimou ao menos 20% da população. Com a criação do Parque do Xingu em 1961, as aldeias ficaram mais próximas e hoje há uma intensa circulação entre seus habitantes e com a cidade, onde comprar alimentos, combustível, material para pesca. E o coronavírus tem uma propagação rápida”, diz Guerreiro, atualmente pesquisador na Universidade de Oxford, na Inglaterra.
Os dois Kalapalo com Covid-19 receberam alta no fim da tarde desta terça (9) e foram encaminhados para a Casai (Casa de Saúde e Apoio ao Índio) em Canarana (MT). A recomendação era que ficassem por lá para cumprir a quarentena, já que os primeiros sintomas surgiram no dia 3 de junho. O isolamento recomendado pelas principais organizações de saúde, no entanto, esbarra em resistência cultural.
Os índios não aceitaram fazer a quarentena por lá e voltaram para a aldeia com a promessa de ficarem numa casa isolada e usando máscaras. “Índio é muito complicado. Eles disseram que estavam bem e precisavam voltar para casa”, diz o também indígena e técnico de enfermagem Tafuraki Nahukuá, que trabalha na Casai.
Para Guerreiro, não dá para fazer uma simplificação dessa escolha em voltar para a aldeia apenas como sendo uma vontade ou capricho. Há questões culturais complexas que podem explicar o fato dos dois índios terem optado por voltar para casa.
“Estou especulando, porque não consegui contato com eles ainda. Mas, pelo que já pesquisei e ouvi dos Kalapalo, eles não gostam de ficar na Casai, porque além de ter uma infraestrutura péssima, eles ficam afastados da família e dos cuidados e supervisão que os parentes têm de perto com os doentes. E também porque temem feitiçaria por parte de algum índio de outra etnia que pode estar eventualmente internado ali”, diz.
Rodrigues explica como é complicado o cenário de isolamento social dentro do Xingu. Os indígenas da região moram em ocas coletivas, com 30, 40 pessoas dentro e compartilham objetos e comida. Muitos não têm acesso à água e sabão para lavar as mãos.
“Faltam EPI [equipamento de proteção individual], treinamento, comunicação, faltam testes e cilindros maiores de oxigênio para os atendimentos que precisarem de mais cuidados e para possíveis remoções até a cidade mais próxima, entre outras coisas.”
A Unifesp, o ISA (Instituto SocioAmbiental), a SPDM (Associação Paulista para o Desenvolvimento da Medicina), o DSEI Xingu, a Coordenação Nacional do Xingu, da Funai, e Atix (Associação da Terra Indígena Xingu) montaram um comitê de crise e com realocação de recursos próprios estão enviando testes para Covid-19, concentradores de oxigênio, oxímetros, EPIs, equipamentos de pesca, máscaras e alimentos.
A universidade, por meio de seu Projeto Xingu, da Escola Paulista de Medicina, está dando treinamento a distância para agentes de saúde e também enviará 500 testes para Covid-19. O ISA mandará outros 380 testes.
“Faltariam no mínimo mais mil”, diz Paulo Junqueira, coordenador do projeto Xingu no ISA, que há 20 anos trabalha na região.
Para Junqueira, a questão agora é ganhar tempo até que as aldeias consigam se organizar melhor e receber equipamentos necessários para conter a doença. Existem dez casas de apoio para isolamento sendo construídas no parque.
O povo Kuikuro está construindo numa aldeia uma oca específica para colocar possíveis infectados em isolamento. Também preparou uma cartilha com informações sobre o coronavírus, em português e na língua Kuikuro.
A AIKAX (Associação Indígena Kuikuro do Alto Xingu) recebeu 28 mil libras (cerca de R$ 176 mil) de ajuda por meio de uma iniciativa comandada pela People’s Palace Project (PPP), organização vinculada à Universidade Queen Mary, de Londres, que trabalha há seis anos com os Kuikuro. “Estamos organizando o envio de suprimentos para evitar ao máximo a exposição das pessoas dali ao vírus”, diz Thiago Jesus, da PPP.
O cacique Yanama Kuikuro, da aldeia Ipatse, diz que a preocupação é grande e que estão correndo contra o tempo para conseguir equipamentos e construir a casa de quarentena rapidamente. Ele conta que com a ajuda do doutor Rodrigues, da Unifesp, está fazendo a compra dos suprimentos necessários e orientando o seu povo. “É uma tristeza enorme termos que cancelar o Kuarup, isso nunca aconteceu. Mas todas lideranças conversaram e vimos que é muito perigoso fazer aglomeração”, fala Yanama.
O povo Yawalapiti também está devastado com o cancelamento do Kuarup. “É o ritual mais sagrado do povo do Alto Xingu. Mas não teve outro jeito”, diz Tapi Yawalapiti, filho do cacique Aritana e uma das lideranças locais.
Ele conta que há dois meses vinham pedindo para as pessoas da aldeia evitarem ir à cidade por causa do vírus, mas que os mais jovens não acreditavam que a doença era grave e poderia atingir os índios. “Eles pegavam as motos e iam escondido. Agora está proibido, precisa de autorização.”
Tapi também conta que na segunda eles fecharam de vez a estrada próxima à aldeia que vai até a cidade. “Ontem já não deixamos nem o carro da Funai passar.”
Segundo ele, nas aldeias Yawalapiti não há máscaras, álcool em gel, remédios ou equipamentos básicos.
O técnico indígena de enfermagem Leonardo Kamaiurá também relata falta de suprimentos e equipamentos de prevenção nas Unidades Básicas de Saúde. “Temos poucas máscaras, o álcool em gel temos que dividir metade do pote para mandar para outros postos. Falta o básico.”
O profissional conta que ouve de muitos índios que o coronavírus seria uma doença apenas de não-indígenas, que seriam mais fracos. “Há uma resistência grande por aqui também para acreditar na pandemia, como acontece no resto do Brasil.”
Todas lideranças indígenas e profissionais de saúde ouvidos pelas Folha dizem que o governo não tem ajudado e que falta informação correta.
A disseminação de notícias falsas ou incorretas, segundo alguns indígenas, está levando medo à população. Em um áudio ao qual a Folha teve acesso, o presidente da Atix, Ianukulá Kaiabi Suiá, diz que há pessoas falando em não reportar sintomas aos agentes de saúde, porque, se isso acontecer, “eles serão levados aos hospitais, serão entubados e vão morrer”.
A médica Daphne Andrade, do DSEI Xingu, diz que não ouviu isso nas aldeias do Alto Xingu nas quais ela trabalha. “Rodei muitas aldeias levando informação sobre corona, fazendo alguns testes e não ouvi isso. Eles falam sim que têm medo de intubar, porque isso todos nós temos, né? Mas não ouvi isso de não reportar sintomas.”
A reportagem tentou contato com alguma liderança dos Kalapalo, mas por problemas de comunicação no local, não conseguiu.
Em nota, o Ministério da Saúde, por meio da Sesai (Secretaria Especial de Saúde Indígena), diz trabalhar em articulação com o estado, tanto que está prevista a instalação de ala indígena em hospital do Mato Grosso. E que o Distrito Sanitário Especial Indígena do Xingu já recebeu 720 testes para Covid-19 e que estão sendo enviados mais mil. E que enviará mais 36 cilindros de 50 litros de oxigênio.
Graças às iniciativas dos moradores da favela, taxa de mortalidade por Covid-19 é menor do que no resto da capital paulista. Em outras regiões pobres, porém, o cenário é diferente
Redação Galileu
25 Jun 2020 – 14h44 Atualizado em 25 Jun 2020 – 14h51
Paraisópolis tem melhor controle da pandemia do que a cidade de São Paulo (Foto: Wikimedia Commons)
A favela de Paraisópolis, em São Paulo, tem melhor controle da pandemia de Covid-19 do que outros bairros da capital paulista. Em 18 de maio de 2020, a taxa de mortalidade pelo novo coronavírus na região era de 21,7 pessoas por 100 mil habitantes, enquanto a média municipal era de 56,2. Os números são do Instituto Pólis, organização da sociedade civil que realiza pesquisas no Brasil e no exterior.
“Desde a confirmação dos primeiros casos em São Paulo, logo em março, a associação de moradores de Paraisópolis desenvolveu estratégias para suprir a falta de políticas públicas para a comunidade”, explicam os responsáveis pelo estudo em um relatório publicado em junho.
Logo no início da pandemia, os moradores da favela criaram o sistema de “presidentes de rua”, em que uma pessoa de cada rua ficou responsável por monitorar e ajudar as outras, orientando sobre os sintomas da doença, distribuindo cestas básicas e até combatendo a disseminação de fake news.
Além disso, a comunidade contratou ambulâncias para atender os sintomáticos e recrutou médicos e enfermeiros para suprir a favela 24 horas. Outros 240 moradores foram treinados como socorristas para apoiar as 60 bases de emergência criadas com a presença de bombeiros civis.
Com mais de 70 mil habitantes, a densidade demográfica de Paraisópolis chega a 61 mil hab/km². Tendo isso em vista, a associação de moradores pediu ao governo estadual para utilizar duas escolas públicas como centro de isolamento de pessoas infectadas. A medida possibilitou que os sintomáticos se isolassem de forma eficaz, sem colocar pessoas próximas e familiares em perigo.
Para os pesquisadores, as ações tomadas pelos moradores de Paraisópolis deixam claro que iniciativas de atenção básica à saúde e ações voltadas para garantir a segurança alimentar e outras despesas são essenciais em tempos de pandemia. “A favela, apesar das condições de precariedade e vulnerabilidade, tem sido eficiente em baixar a média de mortalidade do distrito como um todo”, afirma o relatório.
Outras regiões, outra realidade Enquanto em Paraisópolis a situação parece estar menos preocupante, em outras regiões pobres da capital paulista o cenário não é o mesmo. Um documento divulgado também neste mês pelo Instituto Pólis indica que as áreas com maior situação de precariedade urbana são as mais castigadas pela Covid-19. As mais afetadas são Brasilândia, Sapopemba, Grajaú, Capão Redondo e Jardim Ângela.
Dentre as explicações para isso está a impossibilidade de distanciamento social, tanto pela alta densidade demográfica quanto pelo fato de que os trabalhos exercidos pelos moradores dessas regiões não pemitiram que ficassem em casa. a precariedade do saneamento básico, a baixa renda e a falta de acesso à saúde também contribuem para a realidade preocupante.
Número de óbitos por Covid-19 a cada 100 mil habitantes nos bairros de São Paulo (Foto: Instituto Pólis)
Em relação às taxas de óbitos a cada 100 mil habitantes, o mapa de Covid-19 se concentra em outras regiões de São Paulo, nos bairros Pari, Brás, Belém, Campo Belo e Limão. “Por haver mais pessoas morando nas regiões periféricas, o maior número de mortes absoluto pode fazer com que se pense que apenas a periferia está vulnerável”, disse Danielle Klintowitz, do Instituto Pólis, em comunicado. “Mas há de se analisar o contágio em territórios precários mais centrais para que a situação não fuja do controle.”
Alunos do ensino médio voltam à sala de aula em Wuham, província de Hubei, na China, nesta quarta-feira (6). Fonte: AFP.
Após decretarem o afrouxamento do isolamento social para conter a transmissão do novo coronavírus, países que estão voltando às aulas adotam medidas de prevenção para evitar uma nova onda de contaminação.
O G1 analisou a experiência de países como China, Coreia do Sul, Dinamarca, Finlândia, França, Portugal e Israel para saber quais cuidados estão sendo tomados na volta às aulas. No Brasil, as aulas estão suspensas em todos os estados e as escolas seguem fechadas.
Entre as medidas, estão:
desinfecção de escolas
tendas de desinfecção dos alunos na entrada
controle de temperatura
uso de máscaras
lavagem de mãos e instalação de torneiras
grupos menores de alunos
distanciamento
horários diferentes de entrada e saída
arejar a sala
afastar professores do grupo de risco
A reabertura das escolas é um marco no fim do isolamento porque permite que os pais possam voltar ao mercado de trabalho. Apesar dos esforços, ao menos dois dos países analisados voltaram a registrar casos de transmissão de coronavírus: Coreia do Sul e França.
Na Coreia do Sul, mais de 200 escolas foram fechadas nesta sexta-feira (29) dias após reabrirem, devido ao surgimento de novos casos de contaminação. Com isso, Seul adotou novas medidas para evitar a transmissão de casos, como limitar o número de alunos por sala, enquanto os demais ficam em casa, aprendendo por atividades remotas.
As regras de confinamento impostas para conter o avanço da disseminação do novo coronavírus deixaram mais de 1,5 bilhão de crianças e adolescentes fora da escola em 188 países, segundo balanço da Unesco divulgado em abril.
Desinfecção de escolas
20 de maio – trabalhador desinfeta escola em Parque Ivory, na África do Sul. — Foto: Siphiwe Sibeko/Reuters
Medidas extras de limpeza são uma recomendação comum. Em diversas partes do mundo, a desinfecção das escolas ocorre antes dos alunos chegarem e durante a permanência deles.
Na França, as orientações do Ministério da Educação contêm inclusive quais produtos a serem utilizados para desinfecção das escolas e a frequência da higienização: o chão deve ser limpo uma vez por dia enquanto maçanetas, sanitários e interruptores devem ser higienizados várias vezes.
Tenda de desinfecção dos alunos
China tem volta às aulas do ensino médio com medidas de segurança e medo do coronavírus. — Foto: GREG BAKER / AFP
Na China, escolas instalaram tendas de desinfecção por onde os estudantes precisam passar antes de entrarem na escola.
Controle de temperatura
Termômetro usado para medir a temperatura das pessoas e fazer controle da Covid-19.. — Foto: Steve Parsons / Pool / AFP
O controle da temperatura para detectar se o aluno está com febre, um dos mais comuns sintomas da Covid-19, é uma preocupação em vários países.
Em Pequim,pulseiras inteligentes, que fazem essa medição em tempo real, estão sendo testadas. Os pais monitoram a situação por meio de um aplicativo. Caso a temperatura passe de 37ºC, um alerta é enviado para os professores, que são orientados a alertar a polícia.
Uso de máscara
China retoma aulas do ensino médio em Pequim e Xangai nesta segunda-feira (27). — Foto: GREG BAKER / AFP
O uso de máscaras em geral também é recomendado, mas os critérios variam de país para país.
Na China, as crianças utilizam máscaras o tempo todo, inclusive dentro da sala de aula.
Coronavírus na educação: na França, professora leciona com máscara nesta segunda-feira (18). — Foto: Sebastien Bozon/AFP
Em Israel, as crianças da 4ª série em diante tem que usar essa proteção. Na França, as crianças menores também estão dispensadas. No entanto, a escola deve ter máscaras à disposição dos alunos caso eles apresentem sintomas durante as aulas e estejam aguardando para serem retirados.
Uma exceção é a Dinamarca, país onde não existe a recomendação para utilização de máscaras em ambientes públicos.
Lavagem de mãos e instalação de torneiras
Crianças lavam as mãos na escola Gudenåskolen, na Dinamarca — Foto: Lone Mathiesen/ Divulgação/ Embaixada da Dinamarca no Brasil
O incentivo à higiene e lavagem de mãos está sendo constante nas escolas que voltam às aulas.
Na Dinamarca, as escolas chegaram a instalar torneiras fora dos edifícios para que as crianças lavem as mãos quando chegam à escola.
18 de maio de 2020 – Alunos usam máscara em sala de aula no colégio D. Pedro V, em Lisboa, no dia em que parte dos estudantes volta a ter aula em meio à pandemia do novo coronavírus (COVID-19) em Portugal — Foto: Rafael Marchante/Reuters
Alguns países adotaram a medida de dividir os estudantes em grupos menores para evitar contatos mais próximos entre eles, como na Finlândia.
Na Dinamarca, as turmas, que têm entre 20 e 28 alunos, foram divididas para que os alunos possam interagir apenas dentro desse espectro menor.
Em Seul, na Coreia do Sul, os jardins de infância e escolas do ensino básico, fundamental e médio poderão receber apenas um aluno a cada três e os demais terão que seguir com o ensino a distância.
Distanciamento
15 de maio – Estudantes conversam enquanto praticam o distanciamento social no pátio de uma escola secundária durante sua reabertura em Bruxelas, na Bélgica, durante o surto do coronavírus (COVID-19) — Foto: Yves Herman/Reuters
Em geral, as salas de aula foram reorganizadas de maneira que as mesas dos alunos fiquem a pelo menos um metro de distância entre elas. A recomendação é feita pelo governos da França, Dinamarca. Em Israel, essa distância é de dois metros.
Na Dinamarca, além da distância de um metro entre as mesas dos alunos, o professor deve ficar a dois metros do estudante que senta mais próximo dele.
Alguns países adotam inclusive paredes acrílicas para evitar que gotículas da fala sejam trocadas entre os estudantes e entre estudantes e professores, como é o caso da Coreia do Sul.
Alunos retomam aulas na Coreia do Sul; em algumas escolas, carteiras têm divisórias — Foto: Yonhap / AFP Photo
Para estudantes menores, mantê-los afastados é um desafio. Uma solução lúdica, feita com asas de papelão, foi adotada na província de Shanxi, na China, para lembrá-los a distância que precisam ficar uns dos outros.
Alunos do ensino fundamental usam asas para manter o distanciamento na sala de aula em Taiyuan, na província de Shanxi, no norte da China. Foto tirada em 20 de maio de 2020 — Foto: AFP
A mesma medida foi adotada pelos governo da Finlândia e Israel, que determinaram o estabelecimento de horários diferentes para intervalos, entrada e saída para evitar aglomeração.
Na Dinamarca, além dos horários variados, novos portões estão sendo utilizados para que a entrada e saída dos grupos não coincidam. Os pais também são orientados a se despedir dos filhos fora da escola e devem pedir permissão, caso necessitem entrar no estabelecimento.
Arejar a sala
Na França, as escolas são orientadas a manter as janelas abertas antes das aulas, durante o intervalo e depois da partida dos alunos.
Afastamento de professores do grupo de risco
27 de abril – Médicos de um hospital coletam amostras de professores do ensino médio para testes em uma escola após o surto da doença por coronavírus em Yichang, província de Hubei, na China — Foto: China Daily via Reuters
Em Israel, professoras com mais de 65 anos não retomaram as atividades. A medida é para evitar que eles fiquem expostos à uma possível nova onda de circulação do coronavírus.
Gravediggers work during a mass burial of people who passed away due to the coronavirus disease (COVID-19), at the Parque Taruma cemetery in Manaus, Brazil, May 26, 2020. Picture taken with a drone. REUTERS/Bruno Kelly
BRASILIA (Reuters) – As Brazil’s daily COVID-19 death rate climbs to the highest in the world, a University of Washington study is warning its total death toll could climb five-fold to 125,000 by early August, adding to fears it has become a new hot spot in the pandemic.
The forecast from the University of Washington’s Institute for Health Metrics and Evaluation (IHME), released as Brazil’s daily death toll climbed past that of the United States on Monday, came with a call for lockdowns that Brazil’s president has resisted.
“Brazil must follow the lead of Wuhan, China, as well as Italy, Spain, and New York by enforcing mandates and measures to gain control of a fast-moving epidemic and reduce transmission of the coronavirus,” wrote IHME Director Dr. Christopher Murray.
Without such measures, the institute’s model shows Brazil’s daily death toll could keep climbing to until mid-July, driving shortages of critical hospital resources in Brazil, he said in a statement accompanying the findings.
On Monday, Brazil’s coronavirus deaths reported in the last 24 hours were higher than fatalities in the United States for the first time, according to the health ministry. Brazil registered 807 deaths and 620 died in the United States.
The U.S. government on Monday brought forward to Tuesday midnight enforcement of restrictions on travel to the United States from Brazil as the South American country reported the highest death toll in the world for that day.
Washington’s ban applies to foreigners traveling to the United States if they had been in Brazil in the last two weeks. Two days earlier, Brazil overtook Russia as the world’s No. 2 coronavirus hot spot in number of confirmed cases, after the United States.
Murray said the IHME forecast captures the effects of social distancing mandates, mobility trends and testing capacity, so projections could shift along with policy changes.
The model will be updated regularly as new data is released on cases, hospitalizations, deaths, testing and mobility.
Reporting by Anthony Boadle; Editing by Brad Haynes and Steve Orlofsky
(CNN) As the novel coronavirus has spread across the globe, President Trump has repeated one phrase like a mantra: It will go away.
Since February Trump has said the virus will “go away” at least 15 times, most recently on May 15.
“It’s going to disappear one day,” he said on February 27. “It’s like a miracle.”
Invoking a miracle is an understandable response during a pandemic, but to some, the President’s insistence that the coronavirus will simply vanish sounds dangerously like magical thinking — the popular but baffling idea that we can mold the world to our liking, reality be damned.
The coronavirus, despite Trump’s predictions, has not disappeared. It has spread rapidly, killing more than 90,000 Americans.
In that light, Trump’s response to the pandemic, his fulsome self-praise and downplaying of mass death seems contrary to reality. But long ago, his biographers say, Trump learned how to craft his own version of reality, a lesson he learned in an unlikely place: a church.
It’s called the “power of positive thinking,” and Trump heard it from the master himself: the Rev. Norman Vincent Peale, a Manhattan pastor who became a self-help juggernaut, the Joel Osteen of the 1950s.
“He thought I was his greatest student of all time,” Trump has said.
Undoubtedly, the power of positive thinking has taken Trump a long way — through multiple business failures to the most powerful office in the world.
Trump has repeatedly credited Peale — who died in 1993 — and positive thinking with helping him through rough patches.
Norman Vincent Peale wrote the bestselling 1952 self-help book, “The Power of Positive Thinking.” It sold millions of copies.
“I refused to be sucked into negative thinking on any level, even when the indications weren’t great,” Trump said of the early 1990s, when his casinos were tanking and he owed creditors billions of dollars.
But during a global public health crisis there can be a negative side to positive thinking.
“Trump pretending that this pandemic will just go away is not just an unacceptable fantasy,” said Christopher Lane, author of “Surge of Piety: Norman Vincent Peale and the Remaking of American Religious Life.”
“It is in the realm of dangerous delusion.”
Trump says Peale has made him feel better about himself
Though they were professed Presbyterians, it’s more accurate to call Trump’s family Peale-ites.
On Sundays, Trump’s businessman father drove the family from Queens to Peale’s pulpit at Marble Collegiate Church in Manhattan.
The centuries-old edifice was, and remains, the closest thing Trump has to a family church. Funerals for both of his parents were held there, and Peale presided over Trump’s marriage to Ivana at Marble Collegiate in 1977. Two of his siblings were also married in the sanctuary.
The draw, Trump’s biographers say, was Peale, who elevated businessmen like the Trumps to saint-like status as crusaders of American capitalism.
Known as “God’s Salesman,” Peale wrote many self-help books, including “The Power of Positive Thinking,” that sold millions of copies.
From left to right, Donald Trump, Ivana Trump, Ruth Peale and Dr. Norman V. Peale at Peale’s 90th birthday party in 1988.
Peale drew throngs of followers, but also sharp criticism from Christians who accused him of cherry-picking Bible verses and peddling simplistic solutions.
But the young Donald Trump was hooked.
“He would instill a very positive feeling about God that also made me feel positive about myself,” Trump writes in “Great Again,” one of his books. “I would literally leave that church feeling like I could listen to another three sermons.”
Peale peppered his sermons with pop psychology. Sin and guilt were jettisoned in favor of “spirit-lifters,” “energy-producing thoughts” and “7 simple steps” to happy living.
“Attitudes are more important than facts,” Peale preached, a virtual prophecy of our post-truth age.”Formulate and stamp indelibly on your mind a mental picture of yourself as succeeding,” Peale writes in “The Power of Positive Thinking.”
“Hold this picture tenaciously. Never permit it to fade.”
Peale has also influenced Trump’s spiritual advisers
To this day, Trump surrounds himself with Peale-like figures, particularly prosperity gospel preachers.
One of his closest spiritual confidantes, Florida pastor Paula White, leads the White House’s faith-based office and is a spiritual descendent of Peale’s positive thinking — with a Pentecostal twist.
White, a televangelist, belongs to the Word of Faith movement, which teaches that God bestows health and wealth on true believers.
In a Rose Garden ceremony for the National Day of Prayer earlier this month, White quoted from the Bible’s Book of Job: “If you decree and declare a thing, it will be established.”
“I declare no more delays to the deliverance of Covid-19,” White continued. “No more delays to healing and a vaccination.”
Paula White, a televangelist and religious adviser to President Trump.
The Book of Job, a parable of human suffering and powerlessness, may be a strange book for a preacher to cite while “declaring” an end to the pandemic. If it were so easy, Job’s story would involve fewer boils and tortures.
But in a way, White perfectly captures the problem with positive thinking: It tries to twist every situation into a “victory,” even when reality demonstrates otherwise.
“Positive thinking can help people focus on goals and affirm one’s merits,” said Lane, author of the book on Peale. “But it does need a reality check, and to be based in fact.
“Sometimes, the reality is that you’ve failed and need to change course. But to Peale, that wasn’t an option. Even self-doubt was a sin, he taught, an affront to God.
“He had a huge problem with failure,” Lane said. “He would berate people for even talking about it.”
Peale’s teachings can explain why Trump won’t accept criticism
You can hear echoes of Peale’s no-fail philosophy in Trump’s angry response to reporters’ questions about his handling of the coronavirus pandemic, said Trump biographer Michael D’Antonio.
“Nothing is an exchange of ideas or discussion of facts,” D’Antonio said. “Everything is a life or death struggle for the definition of reality. For him, being wrong feels like being obliterated.”
President Donald Trump answers questions with members of the White House Coronavirus Task Force on April 3, 2020 in Washington.
And that’s one reason why the President refuses to accept any criticism or admit to any failure. To do so would puncture his bubble of positivity, not to mention his self-image.
Instead, he has misled the public, claiming in February that the situation was “under control” when it was not; promising a vaccine is coming “very soon,” which it is not; and falsely insisting that “anyone can get tested,” when they could not and many still cannot.
Com mais de 300 mil mortes confirmadas no mundo, espalhadas por todos os continentes, a covid-19 já é mais letal que desastres naturais, atentados terroristas e guerras
Renato Vasconcelos e Paulo Beraldo
15 de maio de 2020 | 05h00
Apandemia do novo coronavírus já tem envergadura de desastre. Com mais de 300 mil mortes confirmadas até esta quinta-feira, 14, a covid-19 já matou mais pessoas do que guerras, desastres naturais e atentados terroristas que marcaram a história. Apesar da letalidade da doença, uma grande quantidade de pessoas, incluindo líderes mundiais, continuam a minimizar ou negar a pandemia – que continua a fazer vítimas diárias em todos os continentes.
Para o professor de história da Universidade Federal de Santa Maria (UFSM), João Malaia, o quanto um evento trágico impressiona alguém depende de fatores como a duração, a proximidade de quem morre e a distância física do fenômeno em si. “Muitas mortes em um período curto também tendem a impressionar mais. No caso de uma pandemia, as mortes diárias vão diluindo o sentimento da tragédia, a não ser para aqueles que perdem pessoas próximas”, explica o pesquisador, que coordena um projeto de pesquisa sobre a gripe espanhola no Brasil, o ‘Mais História, por favor!’.
Segundo Malaia, a normalização da morte nos discursos de autoridades como o presidente da República acaba reforçando o sentimento de conformação de parte da população. Olhando para o passado, vê semelhanças na forma como o Brasil lidou com a gripe espanhola. “O governo brasileiro foi muito criticado na época por setores da imprensa por demorar a tomar medidas, principalmente no Rio de Janeiro, então capital federal, quando já se sabia dos casos”, diz.
Imagem aérea mostra o dano causado pelo tsunami na cidade turística de Phuket, na Tailândia, em 26 de dezembro de 2004Reuters
O número de mortes pelo mundo já ultrapassou qualquer desastre natural da história recente. O tsunami de 2004, que varreu países banhados pelo Oceano Índico e considerado o mais mortal da história, vitimou cerca de 230 mil pessoas. O cenário não é muito diferente se observados os contextos regionais e nacionais.
MAIS BAIXAS QUE OS CIVIS DO IRAQUE
Soldado americano observa a derrubada da estátua de Saddam Hussein no centro de Bagdá, em 9 de abril de 2003Goran Tomasevic/Reuters
Na Europa, continente com mais mortos até o momento, somados os quatro países mais afetados pela pandemia – Reino Unido, Itália, França e Espanha – o número de vítimas é maior do que o total de civis mortos nos últimos dez anos da Guerra do Iraque (2009-2019).
EUA
PIOR QUE O VIETNÃ
Corpos de soldados americanos mortos na Batalha do vale Ia Drang, primeira grande derrota do país no Vietnã, em 15 de novembro de 1965Neil Sheehan/The New York Times
Nos Estados Unidos, o número de vítimas do novo coronavírus entre fevereiro e maio – menos de 120 dias – já é maior do que o de militares americanos mortos na Guerra do Vietña (58 mil), que durou 20 anos.
QUASE 30 VEZES O 11 DE SETEMBRO
Equipe de resgate retira homem de uma das torres do World Trade Center, em Nova York, logo após o atentado de 11 de setembro de 2001Shannon Stapleton/Reuters
Seriam necessários mais de 28 atentados iguais aos de 11 de setembro de 2001, que destruiu as torres gêmeas do World Trade Center, para igualar o número de mortos pela covid-19 nos EUA. Já o Estado de Nova York, palco da catástrofe, precisaria presenciar mais de 9 atentados para igualar o número de mortos pela pandemia.
MAIS DE 100 GUERRAS
Parentes de soldados argentinos mortos na Guerra das Malvinas visitam cemitério na ilha pela primeira vez, em 19 de março de 1991Reuters
O Reino Unido, que tomou o posto da Itália de país mais afetado pela pandemia no continente, teria que lutar mais de 130 Guerras das Malvinas para ter o mesmo número de baixas provocadas pelo coronavírus. Se contarmos o número total de mortos na guerra (britânicos e argentinos), seriam necessários mais de 36 conflitos idênticos ao disputado no Atlântico sul.
CUSTO MAIOR QUE A INDEPENDÊNCIA
Quadro retrata a Batalha de San MartinoLuigi Norfini
A Segunda Guerra de Independência da Itália, iniciada em 1859, foi o último episódio no processo de unificação do país. Estima-se que mais de 12 mil vidas foram perdidas durante o conflito, o que equivale a menos da metade das vítimas da pandemia.
1500 ANOS DE TERRORISMO
Mascarados, guerrilheiros do ETA leem anúncio ao vivo na televisão espanhola em 18 de fevereiro de 2004Vincent West/Reuters
Na Espanha, as vítimas da covid-19 somam um número 30 vezes maior do que os mortos em atentados promovidos pela Pátria Basca e Liberdade (ETA). Em 50 anos de atividade, as ações do grupo terrorista vitimaram 584 pessoas. Caso ainda existisse e mantivesse a mesma média de letalidade, o ETA só conseguiria igualar o número de mortes provocadas pela pandemia em 1.586 anos de terrorismo.
ATENTADOS DO ISIS EM PARIS
Brigadistas prestam socorro a feridos perto da boate Bataclan, em 13 de novembro de 2015Christian Hartmann/Reuters
Comparativamente, os mortos pela covid-19 na França correspondem a, aproximadamente, 300 ataques terroristas iguais ao que ocorreu na boate Bataclan, em 25 de novembro de 2015, quando o grupo jihadista Estado Islâmico (ISIS) fez um de seus mais famosos atentados até então.
BRASIL E SÃO PAULO
No caso brasileiro, os mais de 13 mil mortos fazem desastres como o de Brumadinho ficarem pequenos. Teriam que ter ocorrido 52 acidentes iguais ao da cidade mineira para alcançar a mortalidade. O mesmo pode ser dito do massacre do Carandiru. Seriam precisas 122 chacinas para que o número de mortos se igualasse ao do país. Já São Paulo teria que lutar quatro Revoluções Constitucionalistas para igualar as baixas.
REVOLUÇÃO CONSTITUCIONALISTA DE 1932
Soldados paulistas combateram, com armamento precário, as poderosas colunas inimigas. Reprodução feita no dia 02 de junho de 2013, dos originais publicados pelo jornal ‘O Estado de S. Paulo’ durante a cobertura da Revolução Constitucionalista de 1932ARQUIVO/AE
Os corpos dos detentos mortos há dois dias são acondicionados de salas e corredores do IML (Instituto Médico Legal)EPITÁCIO PESSOA/ESTADÃO
Helicóptero do Corpo de Bombeiros e agentes da defesa civil trabalham no resgate dos corpos das vítimas encontrados em um ônibus de funcionários da VALE na região onde ficavam os escritórios da empresa em BrumadinhoWILTON JUNIOR/ ESTADÃO
REVOLUÇÃO TEOCRÁTICA DO IRÃ
Apoiadores do aiatolá Khomeini mostra sua imagem em Teerã, no Irã, durante a revolução islâmica de 1979REUTERS
Na Ásia, onde a pandemia começou, a mortalidade também alcançou níveis históricos. O número de mortos no Irã é duas vezes superior ao número de mortos da Revolução Teocrática que mudou o regime do país em 1979.
EXÉRCITO DE TERRACOTA
Imagem de parte do Exército de Soldados de Terracota de Xian, na ChinaLudovic Marin/ AFP
Na China, o número de mortos sepultados no país já é o equivalente a metade das estátuas do Exército de Terracota, enterradas no túmulo do imperador Qin Shi Huang.
Expediente
Editor executivo multimídia Fabio Sales / Editora de infografia multimídia Regina Elisabeth Silva / Editores assistentes multimídia Adriano Araujo, Carlos Marin, Glauco Lara e William Marioto / Editor de Internacional Cristiano Dias / Reportagem Renato Vasconcelos, Rodrigo Turrer e Paulo Beraldo / Edição de fotografia Sérgio Neves / Foto da capa Juan Carlos Ulate/Reuters / SEO Brenda Zacharias / Designer multimídia Lucas Almeida
O ano de 2020 será lembrado como o ano em que a pandemia causada pelo vírus SARS-CoV-2 precipitou uma ruptura maior no funcionamento das sociedades contemporâneas. Será provavelmente lembrado também como o momento de uma ruptura da qual nossas sociedades não mais se recuperaram completamente. Isso porque a atual pandemia intervém num momento em que três crises estruturais na relação entre as sociedades hegemônicas contemporâneas e o sistema Terra se reforçam reciprocamente, convergindo em direção a uma regressão econômica global, ainda que com eventuais surtos conjunturais de recuperação. Essas três crises são, como reiterado pela ciência, a emergência climática, a aniquilação em curso da biodiversidade e o adoecimento coletivo dos organismos, intoxicados pela indústria química.i Os impactos cada vez mais avassaladores decorrentes da sinergia entre essas três crises sistêmicas deixarão doravante as sociedades, mesmo as mais ricas, ainda mais desiguais e mais vulneráveis, menos aptas, portanto, a recuperar seu desempenho anterior. São justamente tais perdas parciais, cada vez mais frequentes, de funcionalidade na relação das sociedades com o meio ambiente que caracterizam essencialmente o processo de colapso socioambiental em curso (Homer-Dixon et al. 2015; Steffen et al. 2018; Marques 2015/2018 e 2020).
O ano da pandemia é o do mais crucial ponto de inflexão da história humana
Por sua extensão global e pelo rastro de mortes deixadas em sua passagem, superior a 250 mil vítimas (oficialmente notificadas) em pouco mais de quatro meses, a atual pandemia é um fato cuja gravidade seria difícil exagerar, tanto mais porque novos surtos podem ainda ocorrer nos próximos dois anos, segundo um relatório do Center for Infectious Disease Research and Policy (CIDRAP), da Universidade de Minnesota (Moore, Lipsitch, Barry & Osterholm 2020).
Mas ainda mais grave que o saldo imenso de mortes, é o momento da incidência da pandemia na história humana. Outras pandemias, algumas muito mais letais, ocorreram no século XX, sem afetar profundamente a capacidade de recuperação das sociedades. O que singulariza a atual pandemia é o fato de se somar a diversas crises sistêmicas que ameaçam a humanidade, e isso justamente no momento em que não é mais possível postergar decisões que afetarão crucialmente, e muito em breve, a habitabilidade do planeta. A ciência condiciona a possibilidade de estabilizar o aquecimento médio global dentro, ou não muito além, dos limites almejados pelo Acordo de Paris a um fato incontornável: as emissões de CO2 devem atingir seu pico em 2020 e começar a declinar fortemente em seguida. O IPCC traçou 196 cenários através dos quais podemos limitar o aquecimento médio global a cerca de 0,5oC acima do aquecimento médio atual em relação ao período pré-industrial (1,2oC em 2019). Nenhum deles, lembram Tom Rivett-Carnac e Christiana Figueres, admite que o pico de emissões de gases de efeito estufa (GEE) seja protelado para além de 2020 (Hooper 2020). Ninguém exprime o significado dessa data-limite de modo mais peremptório que Thomas Stocker, co-diretor do IPCC entre 2008 e 2015:ii
“Mitigação retardada ou insuficiente impossibilita limitar o aquecimento global permanentemente. O ano de 2020 é crucial para a definição das ambições globais sobre a redução das emissões. Se as emissões de CO2 continuarem a aumentar além dessa data, as metas mais ambiciosas de mitigação tornar-se-ão inatingíveis”.
Já em 2017, Jean Jouzel, ex-vice-presidente do IPCC, advertia que “para manter alguma chance de permanecer abaixo dos 2oC é necessário que o pico das emissões seja atingido no mais tardar em 2020” (Le Hir 2017). Em outubro do ano seguinte, comentando o lançamento do relatório especial do IPCC, intitulado Global Warming 1.5oC, Debra Roberts, co-diretora do Grupo de Trabalho 2 desse relatório, reforçava essa percepção: “Os próximos poucos anos serão provavelmente os mais importantes de nossa história”. E Amjad Abdulla, representante dos Pequenos Estados Insulares em Desenvolvimento (SIDS) nas negociações climáticas, acrescentava: “Não tenho dúvidas de que os historiadores olharão retrospectivamente para esses resultados [do relatório especial do IPCC de 2018] como um dos momentos definidores no curso da história humana” (Mathiesen & Sauer 2018). Em The Second Warning: A Documentary Film (2018), divulgação do manifesto The Scientist’s Warning to Humanity: A Second Notice, lançado por William Ripple e colegas em 2017 e endossado por cerca de 20 mil cientistas, a filósofa Kathleen Dean Moore faz suas as declarações acima mencionadas: “Estamos vivendo um ponto de inflexão. Os próximos poucos anos serão os mais importantes da história da humanidade”.
Em abril de 2017, um grupo de cientistas, coordenados por Stephan Rahmstorf, lançava The Climate Turning Point, em cujo Prefácio se reafirma a meta mais ambiciosa do Acordo de Paris (“manter o aumento da temperatura média global bem abaixo de 2oC em relação ao período pré-industrial”), esclarecendo que: “essa meta é considerada necessária para evitar riscos incalculáveis à humanidade, e é factível – mas, realisticamente, apenas se as emissões globais atingirem um pico até o ano de 2020, no mais tardar”. Esse documento norteou então a criação, por diversas lideranças científicas e diplomáticas, da Missão 2020 (https://mission2020.global/). Ela definia metas básicas em energia, transporte, uso da terra, indústria, infraestrutura e finanças, de modo a tornar declinante, a partir de 2020, a curva das emissões de gases de efeito estufa e colocar o planeta numa trajetória consistente com o Acordo de Paris. “Com radical colaboração e teimoso otimismo”, escreve Christiana Figueres e colegas da Missão 2020, “dobraremos a curva das emissões de gases de efeito estufa até 2020, possibilitando à humanidade florescer.” De seu lado, António Guterres, cumprindo sua missão de incentivar e coordenar os esforços de governança global, alertava em setembro de 2018: “Se não mudarmos nossa rota até 2020, corremos o risco de deixar passar o momento em que é ainda possível evitar uma mudança climática desenfreada (arunaway climate change), com consequências desastrosas para a humanidade e para os sistemas naturais que nos sustentam”.
Pois bem, 2020, enfim, chegou. Fazendo em 2019 um balanço dos progressos realizados em direção às metas da Missão 2020, o World Resources Institute (Ge et al., 2019) escreve que “na maioria dos casos, a ação foi insuficiente ou o progresso foi nulo” (in most cases action is insufficient or progress is off track). Nenhuma das metas, em suma, foi alcançada e, em dezembro passado, a COP25 em Madri varreu definitivamente, em grande parte por culpa dos governos dos EUA, Japão, Austrália e Brasil (Irfan 2019), as últimas esperanças de uma diminuição iminente das emissões globais de GEE.
A pandemia entra em cena
Mas eis que a Covid-19 irrompe, deslocando, paralisando e adiando tudo, inclusive a COP26. E em pouco mais de três meses resolveu pelo caos e pelo sofrimento o que mais de três décadas de fatos, de ciência, de campanhas e de esforços diplomáticos para diminuir as emissões de GEE mostraram-se incapazes de realizar (já a Conferência de Toronto, de 1988, recomendava “ações específicas” nesse sentido). Ao invés de um decrescimento econômico racional, gradual e democraticamente planejado, o decrescimento econômico abrupto imposto pela pandemia afigura-se já, segundo Kenneth S. Rogoff, como “a mais profunda queda da economia global em 100 anos” (Goodman 2020). Em 15 de abril, o Carbon Brief estimou que a crise econômica deve provocar uma diminuição estimada em cerca de 5,5% nas emissões globais de CO2 em 2020. Em 30 de abril, a Global Energy Review 2020 – The impacts of the Covid-19 crisis on global energy demand and CO2 emissions, da Agência Internacional de Energia (AIE), vai mais longe e estima que “as emissões globais de CO2 devem cair ainda mais rapidamente ao longo dos nove meses restantes do ano, atingindo 30,6 Gt [bilhões de toneladas] em 2020, quase 8% mais baixas que em 2019. Este seria o nível mais baixo desde 2010. Tal redução seria a maior de todos os tempos, seis vezes maior que a redução precedente de 0,4 Gt em 2009, devido à crise financeira e duas vezes maior que todas as reduções anteriores desde o fim da Segunda Guerra Mundial”. (https://www.iea.org/reports/global-energy-review-2020/global-energy-and-co2-emissions-in-2020). A Figura 1 indica como essa redução das emissões globais de CO2 reflete a queda na demanda de consumo global de energia primária, comparada com as quedas anteriores.
Figura 1 – Taxas de mudança (%) na demanda global de energia primária, 1900 – 2020
Fonte: AIE, Global Energy Review 2020 The impacts of the Covid-19 crisis on global energy demand and CO emissions, Abril 2020, p. 11
A redução das emissões globais de CO2 projetada pela AIE para 2020 equivale ou é até pouco maior que os 7,6% de redução anual até 2030 que o IPCC considera imprescindível para conter o aquecimento aquém de níveis catastróficos (Evans 2020). O relatório da AIE apressa-se, contudo, em advertir que, “tal como nas crises precedentes, (…) o repique das emissões pode ser maior que o declínio, a menos que a onda de investimentos para retomar a economia seja dirigido a uma infraestrutura energética mais limpa e resiliente”. Salvo raras exceções, os fatos até agora não autorizam a expectativa de uma ruptura com os paradigmas energéticos e socioeconômicos anteriores. Malgrado o colapso do preço do petróleo, ou justamente por isso, as petroleiras estão se movendo com vertiginosa velocidade para tirar partido desse momento, obtendo, por exemplo, investimentos de USD 1,1 bilhão para financiar a conclusão do famigerado oleoduto Keystone XL, que ligará o petróleo canadense ao Golfo do México (McKibben 2020). Os exemplos desse tipo de oportunismo são inúmeros, inclusive no Brasil, onde os ruralistas se aproveitam da situação para fazer aprovar da Medida Provisória 910, que anistia a grilagem e eleva ainda mais as ameaças aos indígenas. Como bem afirma Laurent Joffrin, em sua Lettre politique de 30 de abril para o jornal Libération (Le monde d’avant, en pire?), o mundo pós-pandemia “corre o risco de parecer furiosamente, a curto prazo ao menos, com o mundo de antes, mas em versão piorada”. E Joffrin emenda: “o ‘mundo de após’ não mudará sozinho. Como para o ‘mundo de antes’, seu futuro dependerá de um combate político, paciente e árduo”. Político e árduo, sem dúvida, mas definitivamente não há mais tempo para paciência.
De qualquer modo, uma redução de quase 8% nas emissões globais de CO2 num ano apenas não abriu sequer um dente na curva cumulativa das concentrações atmosféricas desse gás, medidas em Mauna Loa (Havaí). Elas bateram mais um recorde em abril de 2020, atingindo 416,76 partes por milhão (ppm), 3,13 ppm acima de 2019, um dos maiores saltos desde o início de suas mensurações em 1958. Não se trata apenas de um número a mais na selva de indicadores climáticos convergentes. É o número decisivo. Como lembra Petteri Taalas, Secretário-Geral da Organização Meteorológica Mundial: “A última vez que a Terra apresentou concentrações atmosféricas de CO2 comparáveis às atuais foi há 3 a 5 milhões de anos. Nessa época, a temperatura estava 2oC a 3oC [acima do período pré-industrial] e o nível do mar estava 10 a 20 metros mais alto que hoje” (McGrath 2019). Faltam agora menos de 35 ppm para atingir 450 ppm, um nível de concentração atmosférica de CO2 largamente associado a um aquecimento médio global de 2oC acima do período pré-industrial, nível que pode ser atingido, mantida a trajetória atual, em pouco mais de 10 anos. O que nos aguarda por volta de 2030, mantida a engrenagem do sistema econômico capitalista globalizado e existencialmente dependente de sua própria reprodução ampliada, é nada menos que um desastre para a humanidade como um todo, bem como para inúmeras outras espécies. A palavra desastre não é uma hipérbole. O já mencionado Relatório do IPCC de 2018 (Global Warming 1.5oC) projeta que o mundo a 2oC em média acima do período pré-industrial terá quase 6 bilhões de pessoas expostas a ondas de calor extremo e mais de 3,5 bilhões de pessoas sujeitas à escassez hídrica, entre outras muitas adversidades. Desastre é a palavra que melhor define o mundo para o qual rumamos no horizonte dos próximos 10 anos (ou 20, pouco importa), e é exatamente o vocábulo empregado por Sir Brian Hoskins, diretor do Grantham Institute for Climate Change, do Imperial College em Londres: “Não temos evidência de que um aquecimento de 1,9oC é algo com que se possa lidar facilmente, e 2,1oC é um desastre” (Simms 2017).
Em consequência dessas altíssimas concentrações atmosféricas de CO2, o ano passado já foi o mais quente dos registros históricos na Europa (1,2oC acima do período 1981 – 2010!) e, mesmo sem El Niño, há agora, segundo o NOAA, 74,67% de chances de que 2020 venha a ser o ano mais quente em um século e meio de registros históricos na média global,iii batendo o recorde precedente de 2016 (1,24oC acima do período pré-industrial, segundo a NASA). Não é no espaço deste artigo que se podem elencar os muitos indícios de que 2020 será o primeiro ou segundo (após 2016) ano mais quente entre os sete mais quentes (2014-2020) da história da civilização humana desde a última deglaciação, cerca de 11.700 anos antes do presente. Baste aqui ter em mente que, se março de 2020 for representativo do ano, já perdemos a meta mais ambiciosa do Acordo de Paris, pois a temperatura média desse mês cravou globalmente 1,51oC acima do período 1880-1920, conforme mostra a Figura 2.
Figura 2 – Anomalias de temperatura em março de 2020 (1,51C na média global), em relação ao período 1880-1920. Fonte: GISS Surface Temperature Analysis (v4), NASA. <https://data.giss.nasa.gov/gistemp/maps/index_v4.html>.
O aquecimento global é uma arma apontada contra a saúde global. Como mostra Sara Goudarzi (2020), temperaturas mais elevadas favorecem a adaptação de micro-organismos a um mundo mais quente, diminuindo a eficácia de duas defesas básicas dos mamíferos contra os patógenos: (1) muitos micro-organismos não sobrevivem ainda a temperaturas superiores a 37oC, mas podem vir a se adaptar rapidamente a elas; (2) o sistema imune dos mamíferos, pois este perde eficiência em temperaturas mais elevadas. Além disso, o aquecimento global amplia o raio de ação de vetores de epidemias, como a dengue, zika e chikungunya, e altera a distribuição geográfica das plantas e animais, levando espécies animais terrestres a se deslocarem em direção a latitudes mais altas a uma taxa média de 17 km por década (Pecl et al. 2017). Aaron Bernstein, diretor do Harvard University’s Center of Climate, Health and the Global Environment, sintetiza bem a interação entre aquecimento global e desmatamento em suas múltiplas relações com novos surtos epidêmicos:iv
“À medida que o planeta se aquece (…) os animais deslocam-se para os polos fugindo do calor. Animais estão entrando em contato com animais com os quais eles normalmente não interagiriam, e isso cria uma oportunidade para patógenos encontrar outros hospedeiros. Muitas das causas primárias das mudanças climáticas também aumentam o risco de pandemias. O desmatamento, causado em geral pela agropecuária é a causa maior da perda de habitat no mundo todo. E essa perda força os animais a migrarem e potencialmente a entrar em contato com outros animais ou pessoas e compartilhar seus germes. Grandes fazendas de gado também servem como uma fonte para a passagem de infecções de animais para pessoas”.
Sem perder de vista as relações entre a emergência climática e essas novas ameaças sanitárias, foquemos em duas questões bem circunscritas e diretamente ligadas à pandemia atual.
A pandemia foi prevista e será, doravante, mais frequente
A primeira questão refere-se ao caráter, por assim dizer, antropogênico da pandemia. Bem longe de ser adventícia, ela é uma consequência, reiteradamente prevista, de um sistema socioeconômico crescentemente disfuncional e destrutivo. Josef Settele, Sandra Díaz, Eduardo Brondizio e Peter Daszak escreveram um artigo, a convite do IPBES, de leitura obrigatória e que me permito citar longamente:
“Há uma única espécie responsável pela pandemia Covid-19: nós. Assim como com as crises climáticas e o declínio da biodiversidade, as pandemias recentes são uma consequência direta da atividade humana – particularmente de nosso sistema financeiro e econômico global baseado num paradigma limitado, que preza o crescimento econômico a qualquer custo. (…) Desmatamento crescente, expansão descontrolada da agropecuária, cultivo e criação intensivos, mineração e aumento da infraestrutura, assim como a exploração de espécies silvestres criaram uma ‘tempestade perfeita’ para o salto de doenças da vida selvagem para as pessoas. (…) E, contudo, isso pode ser apenas o começo. Embora se estime que doenças transmitidas de outros animais para humanos já causem 700 mil mortes por ano, é vasto o potencial para pandemias futuras. Acredita-se que 1,7 milhão de vírus não identificados, dentre os que sabidamente infectam pessoas, ainda existem em mamíferos e pássaros aquáticos. Qualquer um deles pode ser a ‘Doença X’ – potencialmente ainda mais perturbadora e letal que a Covid-19. É provável que pandemias futuras ocorram mais frequentemente, propaguem-se mais rapidamente, tenham maior impacto econômico e matem mais pessoas, se não formos extremamente cuidadosos acerca dos impactos das escolhas que fazemos hoje” (https://ipbes.net/covid19stimulus).
Cada frase dessa citação encerra uma lição de ciência e de lucidez política. A maior frequência recente de epidemias e pandemias tem por causas centrais o desmatamento e a agropecuária, algo bem estabelecido também por Christian Drosten, atual coordenador do combate à Covid-19 na Alemanha, além de diretor do Instituto de Virologia do Hospital Charité de Berlim e um dos cientistas que identificou a pandemia SARS em 2003 (Spinney 2020).
“Desde que tenha oportunidade, o coronavírus está pronto para mudar de hospedeiro e nós criamos essa oportunidade através de nosso uso não natural de animais – a pecuária (livestock). Essa expõe os animais de criação à vida silvestre, mantém esses animais em grandes grupos que podem amplificar o vírus, e os humanos têm intenso contato com eles – por exemplo, através do consumo de carne –, de modo que tais animais certamente representam uma possível trajetória de emergência para o coronavírus. Camelos são animais de criação no Oriente Médio e são os hospedeiros do vírus MERS, assim como do coronavírus 229E – que é uma causa da gripe comum em humanos –, já o gado bovino foi o hospedeiro original do coronavírus OC43, outra causa de gripe”.
Nada disso é novidade para a ciência. Sabemos que a maioria das pandemias emergentes são zoonoses, isto é, doenças infecciosas causadas por bactérias, vírus, parasitas ou príons, que saltaram de hospedeiros não humanos, usualmente vertebrados, para os humanos. Como afirma Ana Lúcia Tourinho, pesquisadora da Universidade Federal de Mato Grosso (UFMT), o desmatamento é uma causa central e uma bomba-relógio em termos de zoonoses: “quando um vírus que não fez parte da nossa história evolutiva sai do seu hospedeiro natural e entra no nosso corpo, é o caos” (Pontes 2020). Esse risco, repita-se, é crescente. Basta ter em mente que “mamíferos domesticados hospedam 50% dos vírus zoonóticos, mas representam apenas 12 espécies” (Johnson et al. 2020). Esse grupo inclui porcos, vacas e carneiros. Em resumo, o aquecimento global, o desmatamento, a destruição dos habitats selvagens, a domesticação e a criação de aves e mamíferos em escala industrial destroem o equilíbrio evolutivo entre as espécies, facilitando as condições para saltos desses vírus de uma espécie a outra, inclusive a nossa.
4.As próximas zoonoses serão gestadas no Brasil?
O segundo ponto, com o qual concluo este artigo, são as consequências especificamente sanitárias da destruição em curso da Amazônia e do Cerrado. Entre as mais funestas está a crescente probabilidade de que o país se torne o foco das próximas pandemias zoonóticas. Na última década, as megacidades da Ásia do leste, principalmente na China, têm sido o principal “hotspot” de infecções zoonóticas (Zhang et al. 2019). Não por acaso. Esses países estão entre os que mais perderam cobertura florestal no mundo em benefício do sistema alimentar carnívoro e globalizado. O caso da China é exemplar. De 2001 a 2018, o país perdeu 94,2 mil km2 de cobertura arbórea, equivalente a uma diminuição de 5,8% em sua cobertura arbórea no período. “Extração de madeira e agropecuária consomem até 5 mil km2 de florestas virgens todo ano. Na China setentrional e central a cobertura florestal foi reduzida pela metade nas últimas duas décadas”.v Em paralelo com a destruição dos habitats selvagens, o crescimento econômico chinês desencadeou uma demanda por proteínas animais, incluindo as provenientes de animais exóticos (Cheng et al. 2007). Entre 1980 e 2015, o consumo de carne na China cresceu sete vezes e 4,7 vezes per capita (de 15 kg para 70 kg per capita por ano ao longo deste período). Com cerca de 18% da população mundial, a China era em 2018 responsável por 28% do consumo de carne no planeta (Rossi 2018). Segundo um relatório de 2017 do Rabobank, intitulado China’s Animal Protein Outlook to 2020: Growth in Demand, Supply and Trade, a demanda adicional por carne a cada ano na China será de cerca de um milhão de toneladas. “A produção local de carne bovina não consegue acompanhar o crescimento da demanda. Na realidade, a China tem uma escassez estrutural de oferta de carne bovina, que necessita ser satisfeita por importações crescentes”.
A cobertura vegetal dos trópicos tem sido destruída para sustentar essa dieta crescentemente carnívora, não apenas na China, mas em vários países do mundo e particularmente entre nós. No Brasil, a remoção de mais de 1,8 milhão de km2 da cobertura vegetal da Amazônia e do Cerrado nos últimos cinquenta anos, para converter suas magníficas paisagens naturais em zonas fornecedoras de carne e ração animal, em escala nacional e global, representa o mais fulminante ecocídio jamais perpetrado pela espécie humana. Nunca, de fato, em nenhuma latitude e em nenhum momento da história humana, destruiu-se tanta vida animal e vegetal em tão pouco tempo, para a degradação de tantos e para o benefício econômico de tão poucos. E nunca, mesmo para os pouquíssimos que enriqueceram com a devastação, esse enriquecimento terá sido tão efêmero, pois a destruição da cobertura vegetal já começa a gerar erosão dos solos e secas recorrentes, solapando as bases de qualquer agricultura nessa região (na realidade, no Brasil, como um todo).
Em decorrência dessa guerra de extermínio contra a natureza deflagrada pela insanidade dos ditadores militares e continuada pelos civis, atualmente o rebanho bovino brasileiro é de aproximadamente 215 milhões de cabeças, sendo que 80% de seu consumo é absorvido pelo mercado interno, que cresceu 14% nos últimos dez anos (Macedo 2019). Além disso, o Brasil tornou-se líder das exportações mundiais de carne bovina (20% dessas exportações) e de soja (56%), basicamente destinada à alimentação animal. A maior parte do rebanho bovino brasileiro concentra-se hoje nas regiões Norte e Centro-Oeste, com crescente participação da Amazônia. Em 2010, 14% do rebanho brasileiro já se encontrava na região norte do país. Em 2016, essa participação saltou para 22%. Juntas, a região norte e centro-oeste abrigam 56% do rebanho bovino brasileiro (Zaia 2018). Em 2017, apenas 19,8% da cobertura vegetal remanescente do Cerrado permanecia ainda intocada. A continuar a devastação, a pecuária e a agricultura de soja levarão em breve à extinção quase 500 espécies de plantas endêmicas – três vezes mais que todas as extinções documentadas desde 1500 (Strassburg et al. 2017). A Amazônia, que perdeu cerca de 800 mil km2 de cobertura florestal em 50 anos e perderá outras muitas dezenas de milhares sob a sanha ecocida de Bolsonaro, tornou-se, em sua porção sul e leste, uma paisagem desolada de pastos em vias de degradação. O caos ecológico produzido pelo desmatamento por corte raso de cerca de 20% da área original da floresta, pela degradação do tecido florestal de pelo menos outros 20% e pela grande concentração de bovinos na região cria as condições para tornar o Brasil um “hotspot” das próximas zoonoses. Em primeiro lugar porque os morcegos são um grande reservatório de vírus e, entre os morcegos brasileiros, cujo habitat são sobretudo as florestas (ou o que resta delas), circulam pelo menos 3.204 tipos de coronavírus (Maxman 2017). Em segundo lugar porque, como mostraram Nardus Mollentze e Daniel Streicker (2020), o grupo taxonômico dos Artiodactyla (de casco fendido), ao qual pertencem os bois, hospedam, juntamente com os primatas, mais vírus, potencialmente zoonóticos, do que seria de se esperar entre os grupos de mamíferos, incluindo os morcegos. Na realidade, a Amazônia já é um “hotspot” de epidemias não virais, como a leishmaniose e a malária, doenças tropicais negligenciadas, mas com alto índice de letalidade. Como afirma a OMS, “a leishmaniose está associada a mudanças ambientais, tais como o desmatamento, o represamento de rios, a esquemas de irrigação e à urbanização”,vi todos eles fatores que concorrem para a destruição da Amazônia e para o aumento do risco de pandemias. A relação entre desmatamento amazônico e a malária foi bem estabelecida em 2015 por uma equipe do IPEA: para cada 1% de floresta derrubada por ano, os casos de malária aumentam 23% (Pontes 2020).
A curva novamente ascendente desde 2013 da destruição da Amazônia e do Cerrado resultou da execrável aliança de Dilma Rousseff com o que há de mais retrógrado na economia brasileira. Já para a necropolítica de Bolsonaro, a destruição da vida, do que resta do patrimônio natural brasileiro, tornou-se um programa de governo e uma verdadeira obsessão. Bolsonaro está levando o país a dar um salto sem retorno no caos ecológico, de onde a necessidade inadiável de neutralizá-lo por impeachment ou qualquer outro mecanismo constitucional. Não há mais tempo a perder. Entre agosto de 2018 e julho de 2019, o desmatamento amazônico atingiu 9.762 km2, quase 30% acima dos 12 meses anteriores e o pior resultado dos últimos dez anos, segundo o INPE. No primeiro trimestre de 2020, que apresenta tipicamente os níveis mais baixos de desmatamento em cada ano, o sistema Deter, do INPE, detectou um aumento de 51% em relação ao mesmo período de 2019, o nível mais alto para esse período desde o início da série, em 2016. Segundo Tasso Azevedo, coordenador-geral do Projeto de Mapeamento Anual da Cobertura e Uso do Solo no Brasil (MapBiomas), “o mais preocupante é que no acumulado de agosto de 2019 até março de 2020, o nível do desmatamento mais do que dobrou” (Menegassi 2020). Ao monopolizar todas as atenções, a pandemia oferece a Bolsonaro uma oportunidade inesperada para acelerar sua obra de destruição da floresta e de seus povos (Barifouse 2020).
Recapitulemos. O que importa aqui, sobretudo, é entender que a pandemia intervém no momento em que o aquecimento global e todos os demais processos de degradação ambiental estão em aceleração. A pandemia pode acelerá-los ainda mais, na ausência de uma reação política vigorosa da sociedade. Ela acrescenta, em todo o caso, mais uma dimensão a esse feixe convergente de crises socioambientais que impõe à humanidade uma situação radicalmente nova. Pode-se assim formular essa novidade: não é mais plausível esperar, passada a pandemia, um novo ciclo de crescimento econômico global e ainda menos nacional. Se algum crescimento voltar a ocorrer, ele será conjuntural e logo truncado pelo caos climático, ecológico e sanitário. O próximo decênio evoluirá sob o signo de regressões socioeconômicas, pois mesmo a se admitir que a economia globalizada tenha trazido benefícios sociais, eles foram parcos e vêm sendo de há muito superados por seus malefícios. A pandemia é apenas um entre esses malefícios, mas certamente não o pior. Não são mais atuais, portanto, em 2020, as variadas agendas desenvolvimentistas, típicas dos embates ideológicos do século XX. É claro que a exigência de justiça social, bandeira histórica da esquerda, permanece mais que nunca atual. Além de ser um valor perene e irrenunciável, a luta pela diminuição da desigualdade social significa, antes de mais nada, retirar das corporações o poder decisório sobre os investimentos estratégicos (energia, alimentação, mobilidade etc.), assumir o controle democrático e sustentável desses investimentos e, assim, atenuar os impactos do colapso socioambiental em curso. É do aprofundamento da democracia que depende crucialmente, hoje, a sobrevivência de qualquer sociedade organizada num mundo que está se tornando sempre mais quente, mais empobrecido biologicamente, mais poluído e, por todas essas razões, mais enfermo. Sobreviver, no contexto de um processo de colapso socioambiental, não é um programa mínimo. Sobreviver requer, hoje, lutar por algo muito mais ambicioso que os programas socialdemocratas ou revolucionários do século XX. Supõe redefinir o próprio sentido e finalidade da atividade econômica, vale dizer, em última instância, redefinir nossa posição como sociedade e como espécie no âmbito da biosfera.
Referências
BARIFOUSE, Rafael, “Pandemia vai permitir aceleração do desmatamento na Amazônia, prevê consultoria”. BBC Brasil, 26/IV/2020.
CHENG, Vincent C. C. et al., “Severe Acute Respiratory Syndrome Coronavirus as an Agent of Emerging and Reemerging Infection”. Clinical Microbiology Reviews, October, 2007, pp. 660-694.
EVANS, Simon, “Analysis: Coronavirus set to cause largest ever annual fall in CO2 emissions”, Carbon Brief, 9/IV/2020, atualizado em 15 de abril.
GE, Mengpin. et al. , “Tracking Progress of the 2020 Climate Turning Point.” World Resources Institute, Washington D.C. 2019.
GOODMAN, Peter, “Why the Global Recession Could Last a Long Time”. The New York Times, 1/IV/2020.
GOUDARZI, Sara, “How a Warming Climate Could Affect the Spread of Diseases Similar to COVID-19”. Scientific American, 29/IV/2020.
HOMER-DIXON, Thomas et al., “Synchronous failure: the emerging causal architecture of global crisis. Ecology and Society, 20, 3, 2015.
HOOPER, Rowan, “Ten years to save the world”. New Scientist, 14/III/2020, pp. 45-47.
IRFAN, Umair, “The US, Japan, and Australia let the whole world down at the UN climate talks”. Vox, 18/XII/2019.
JOHNSON, Christine K. et al., “Global shifts in mammalian population trends reveal key predictors of virus spillover risk”. Proceedings of theRoyal Society B, 8/IV/2020.
LE HIR, Pierre, “Réchauffement climatique: la bataille des 2C est presque perdue”. Le Monde, 31/XII/2017.
MACEDO, Flávia, “Consumo de carne bovina no Brasil cresceu 14% em 10 anos, diz Cepea”. Canal Rural, 9/XII/2019.
MARQUES, Luiz, Capitalismo e Colapso Ambiental (2015). Campinas, Editora da Unicamp, 3ª ed. 2018.
MATHIESEN, Karl & SAUER, Natalie, “‘Most important years in history’: major UN report sounds last-minute climate alarm”. Climate Home News, 8/X/2018.
MAXMAN, Amy, “Bats Are Global Reservoir for Deadly Coronaviruses”. Scientific American, 12/VI/2017.
McGRATH, Matt, “Climate Change. Greenhouse gas concentrations again break records”. BBC, 25/XI/2019.
McKibben, Bill, “Big Oi lis using the coronavirus pandemic to push through the Keystone XL pipeline”. The Guardian, 5/IV/2020.
MENEGASSI, Duda, “Desmatamento na Amazônia atinge nível recorde no primeiro trimestre de 2020”. ((O)) eco, 13/IV/2020.
MOLLENTZE, Nardus & STREICKER, Daniel G., “Viral zoonotic risk is homogenous among taxonomic orders of mammalian and avian reservoir hosts”. PNAS, 13/IV/2020.
MOORE, Kristine A., LIPSITCH, Marc, BARRY, John & OSTERHOLM, Michael, COVID-19: The CIDRAP Viewpoint. University of Minnesota, 20/IV/2020.
MORIYAMA, Miyu & ICHINOHE, Takeshi, “High Ambient Temperature Dampens Adaptative Immune Responses to Influnza A Virus Infection”. PNAS, 116, 8, 19/II/2019, pp. 3118-3125.
PECL, Gretta et al., “Biodiversity redistribution under climate change: Impacts on ecosystems and human well-being”. Science, 355, 6332, 31/III/2017.
PONTES, Nádia, “O elo entre desmatamento e epidemias investigado pela ciência”. DW, 15/IV/2020.
ROSSI, Marcello, “The Chinese Are Eating More Meat Than Ever Before and the Planet Can’t Keep Up”. Mother Jones, 21/VII/2018.
SETTELE, J., DIAZ, S., BRONDIZIO, E. & DASZAK, Peter, “COVID-19 Stimulus Measures Must Save Lives, Protect Livelihoods, and Safeguard Nature to Reduce the Risk of Future Pandemics”. IPBES Expert Guest Article, 27/IV/2020.
SIMMS, Andrew, “A cat in hell’s chance – why we’re losing the battle to keep global warming below 2C”, The Guardian, 19/I/2017.
SPINNEY, Laura, “Germany’s Covid-19 expert: ‘For many, I’m the evil guy crippling the economy”. The Guardian, 26/IV/2020.
STEFFEN, Will et al., “Trajectories of the Earth System in the Anthropocene”. PNAS, 9/VIII/2018.
STRASSBURG, Bernardo B.N. et al., “Moment of truth for the Cerrado hotspot”. Nature Ecology & Evolution, 2017.
ZAIA, Marina, “Rebanho Brasileiro por Região”. Scot Consultoria, 16/IV/2018.
ZHANG, Juanjuan et al., “Patterns of human social contact and contact with animals in Shanghai, China”. Scientific Reports, 9, 2019.
i Segundo a Chemical Data Reporting (CDR) da EPA, nos EUA, em 2016 havia 8.707 substâncias ou compostos químicos largamente comercializados, aos quais somos cotidianamente expostos, ignorando na maior parte dos casos seus efeitos e os de suas interações sobre a saúde humana e demais espécies. <https://www.chemicalsafetyfacts.org/chemistry-context/debunking-myth-chemicals-testing-safety/>.
*** Luiz Marques é professor livre-docente do Departamento de História do IFCH /Unicamp. Pela editora da Unicamp, publicou Giorgio Vasari, Vida de Michelangelo (1568), 2011 e Capitalismo e Colapso ambiental, 2015, 3a edição, 2018. Coordena a coleção Palavra da Arte, dedicada às fontes da historiografia artística, e participa com outros colegas do coletivo Crisálida, Crises SocioAmbientais Labor Interdisciplinar Debate & Atualização (crisalida.eco.br).
Leading US biologist Thomas Lovejoy says to stop future outbreaks we need more respect for natural world
Caged civet cats in a wildlife market in Guangzhou, China. Photograph: Liu Dawei/AP
Phoebe Weston – Published on Sat 25 Apr 2020 06.00 BST
The vast illegal wildlife trade and humanity’s excessive intrusion into nature is to blame for the coronavirus pandemic, according to a leading US scientist who says “this is not nature’s revenge, we did it to ourselves”.
Scientists are discovering two to four new viruses are created every year as a result of human infringement on the natural world, and any one of those could turn into a pandemic, according to Thomas Lovejoy, who coined the term “biological diversity” in 1980 and is often referred to as the godfather of biodiversity.
“This pandemic is the consequence of our persistent and excessive intrusion in nature and the vast illegal wildlife trade, and in particular, the wildlife markets, the wet markets, of south Asia and bush meat markets of Africa… It’s pretty obvious, it was just a matter of time before something like this was going to happen,” said Lovejoy, a senior fellow at the United Nations Foundation and professor of environment science at George Mason University.
His comments were made to mark the release of a report by the Center for American Progress arguing that the US should step up efforts to combat the wildlife trade to help confront pandemics.
Wet markets are traditional markets selling live animals (farmed and wild) as well as fresh fruit, vegetables and fish, often in unhygienic conditions. They are found all over Africa and Asia, providing sustenance for hundreds of millions of people. The wet market in Wuhan believed to be the source of Covid-19 contained a number of wild animals, including foxes, rats, squirrels, wolf pups and salamanders.
Lovejoy said separating wild animals from farmed animals in markets would significantly lower the risk of disease transmission. This is because there would be fewer new species for viruses to latch on to. “[Domesticated animals] can acquire these viruses, but if that’s all there was in the market, it would really lower the probability of a leak from a wild animal to a domesticated animal.”
He told the Guardian: “The name of the game is reducing certain amounts of activity so the probability of that kind of leap becomes small enough that it’s inconsequential. The big difficulty is that if you just shut them down – which in many ways would be the ideal thing – they will be topped up with black markets, and that’s even harder to deal with because it’s clandestine.”
The pandemic will cost the global economy $1tn this year, according to the World Economic Forum, with vulnerable communities impacted the most, and nearly half of all jobs in Africa could be lost. “This is not nature’s revenge, we did it to ourselves. The solution is to have a much more respectful approach to nature, which includes dealing with climate change and all the rest,” Lovejoy said.
Experts are divided about how to regulate the vast trade in animals, with many concerned the poorest are most at risk from a crackdown. Urgent action on the wildlife trade is clearly needed, said Dr Amy Dickman, a conservation biologist from the University of Oxford, but she was “alarmed” by calls for indiscriminate bans on the wildlife trade.
She is one of more than 250 signatories of an open letter to the World Health Organization and United Nations Environment Programme saying any transition must contribute to – and not detract from – the livelihoods of the world’s most vulnerable people, many of whom depend on wild resources for survival. Other signatories include representatives from the African Wildlife Foundation, the Frankfurt Zoological Society and IUCN (International Union for Conservation of Nature).
The letter reads: “Covid-19 is inflicting unprecedented social and economic costs on countries and communities, with the poor and vulnerable hardest hit. The virus’s suspected links with a Chinese ‘wet market’ has led to calls to ban wet markets and restrict or end the trade, medicinal use and consumption of wildlife. However, indiscriminate bans and restrictions risk being inequitable and ineffective.”
Scientists and NGOs are concerned that over-simplistic and indiscriminate restrictions will exacerbate poverty and inequality, resulting in an increase in criminality. This could accelerate the exploitation and extinction of species in the wild, authors of the letter warn.
“People often seem more willing to point the finger at markets far away, as bans there will not affect their everyday lives – although they will often affect the rights of extremely vulnerable people,” said Dickman.
There are also concerns about the impacts of an outright ban on a number of indigenous populations, such as tribes in Orinoquia and Amazonia, with representatives describing it as an “attack” on their livelihoods.
Mama Mouamfon, who is based in Cameroon and directs an NGO called Fondation Camerounaise de la Terre Vivante (FCTV), said banning the trade would damage livelihoods: “Bush meat is very important for people in the forest because it’s one of the best ways to get animal protein. With this issue of poverty and people living in remote areas, it’s not easy for them to look for good meat,” he said.
“Sometimes people take decisions because they are sitting in an office and are very far from reality. If they knew our reality they would not take that [same] decision.”
Claudio Maierovitch Pessanha Henriques – 6 de maio de 2020
Desde o início da epidemia de doença causada pelo novo coronavírus (Covid-19), a grande pergunta tem sido “quando acaba?” Frequentemente, são divulgadas na mídia e nas redes sociais projeções as mais variadas sobre a famosa curva da doença em vários países e no mundo, algumas recentes, mostrando a tendência de que os casos deixem de surgir no início do segundo semestre deste ano.
Tais modelos partem do pressuposto de que há uma história, uma curva natural da doença, que começa, sobe, atinge um pico e começa a cair. Vamos analisar o sentido de tal raciocínio. Muitas doenças transmissíveis agudas, quando atingem uma população nova, expandem-se rapidamente, numa velocidade que depende de seu chamado número reprodutivo básico, ou R0 (“R zero”, que estima para quantas pessoas o portador de um agente infeccioso o transmite).
Quando uma quantidade grande de pessoas tiver adoecido ou se infectado mesmo sem sintomas, os contatos entre portadores e pessoas que não tiveram a doença começam a se tornar raros. Num cenário em que pessoas sobreviventes da infecção fiquem imunes àquele agente, sua proporção cresce e a transmissão se torna cada vez mais rara. Assim, a curva, que vinha subindo, fica horizontal e começa a cair, podendo até mesmo chegar a zero, situação em que o agente deixa de circular.
Em populações grandes, é muito raro que uma doença seja completamente eliminada desta forma, por isso a incidência cresce novamente de tempos em tempos. Quando a quantidade de pessoas que não se infectaram, somada à dos bebês que nascem e pessoas sem imunidade que vieram de outros lugares é suficientemente grande, então a curva sobe novamente.
É assim, de forma simplificada, que a ciência entende a ocorrência periódica de epidemias de doenças infecciosas agudas. A história nos ilustra com numerosos exemplos, como varíola, sarampo, gripe, rubéola, poliomielite, caxumba, entre muitos outros. Dependendo das características da doença e da sociedade, são ciclos ilustrados por sofrimento, sequelas e mortes. Realmente, nesses casos, é possível estimar a duração das epidemias e, em alguns casos, até mesmo prever as próximas.
A saúde pública tem diversas ferramentas para interferir em muitos desses casos, indicados para diferentes mecanismos de transmissão, como saneamento, medidas de higiene, isolamento, combate a vetores, uso de preservativos, extinção de fontes de contaminação, vacinas e tratamentos capazes de eliminar os microrganismos. A vacinação, ação específica de saúde considerada mais efetiva, simula o que acontece naturalmente, ao aumentar a quantidade de pessoas imunes na população até que a doença deixe de circular, sem que para isso pessoas precisem adoecer.
No caso da Covid-19, há estimativas de que para a doença deixar de circular intensamente será preciso que cerca de 70% da população seja infectada. Isso se chama imunidade coletiva (também se adota a desagradável denominação “imunidade de rebanho”). Quanto à situação atual de disseminação do coronavírus Sars-CoV-2, a Organização Mundial da Saúde (OMS) calcula que até a metade de abril apenas de 2% a 3% da população mundial terá sido infectada. Estimativas para o Brasil são um pouco inferiores a essa média.
Trocando em miúdos, para que a doença atinja naturalmente seu pico no país e comece a cair, será preciso esperar que 140 milhões de pessoas se infectem. A mais conservadora (menor) taxa de letalidade encontrada nas publicações sobre a Covid-19 é de 0,36%, mais ou menos um vigésimo daquela que os números oficiais de casos e mortes revelam. Isso significa que até o Brasil atingir o pico, contaremos 500 mil mortes se o sistema de saúde não ultrapassar seus limites —e, caso isso aconteça, um número muito maior.
Atingir o pico é sinônimo de catástrofe, não é uma aposta admissível, sobretudo quando constatamos que já está esgotada a capacidade de atendimento hospitalar em várias cidades, como Manaus, Rio de Janeiro e Fortaleza —outras seguem o mesmo caminho.
A única perspectiva aceitável é evitar o pico, e a única forma de fazê-lo é com medidas rigorosas de afastamento físico. A cota de contatos entre as pessoas deve ficar reservada às atividades essenciais, entre elas saúde, segurança, cadeias de suprimento de combustíveis, alimentos, produtos de limpeza, materiais e equipamentos de uso em saúde, limpeza, manutenção e mais um ou outro setor. Alguma dose de criatividade pode permitir ampliar um pouco esse leque, desde que os meios de transporte e vias públicas permaneçam vazios o suficiente para que seja mantida a distância mínima entre as pessoas.
O monitoramento do número de casos e mortes, que revela a transmissão com duas a três semanas de defasagem, deverá ser aprimorado e utilizado em conjunto com estudos baseados em testes laboratoriais para indicar o rigor das medidas de isolamento.
Se conseguirmos evitar a tragédia maior, vamos conviver com um longo período de restrição de atividades, mais de um ano, e teremos que aprender a organizar a vida e a economia de outras formas, além de passar por alguns períodos de “lockdown” —cerca de duas semanas cada, se a curva apontar novamente para o pico.
Hoje, a situação é grave e tende a se tornar crítica. O Brasil é o país com a maior taxa de transmissão da doença; é hora de ficar em casa e, se for imprescindível sair, fazer da máscara uma parte inseparável da vestimenta e manter rigorosamente todos os cuidados indicados.
Os indígenas chamam a pandemia de xawara. Um jovem da etnia morreu de Covid-19, em Boa Vista, Roraima.
A imagem é da Expedição Yanomami Okrapomai (Christian Braga/Midia Ninja/2014)
São Gabriel da Cachoeira (AM) – “A floresta protege porque ela tem um cheiro muito saudável, isso é a proteção que a floresta dá para nós Yanomami. A floresta tem mais proteção porque o ar não é contaminado. Muitos já foram para se proteger na floresta porque evitam de pegar gripe e outras doenças aqui na comunidade. Estão por lá se alimentando com caça, pesca, agora é muito açaí e muita fruta que está tendo na floresta”.
É assim, como se vê na fala da liderança Yanomami, José Mário Pereira Góes, que os indígenas estão se protegendo contra o coronavírus. Ele é presidente da Associação Yanomami do Rio Cauaburis e Afluentes (Ayrca), no Amazonas. Tal como os mais velhos fizeram para fugir de epidemias já enfrentadas no passado, como sarampo, gripes e coqueluche, os indígenas dessa etnia estão se refugiando no interior da floresta amazônica para se afastar do risco de contrair a Covid-19, a doença que causa uma pandemia no mundo e é responsável pela morte de um jovem da etnia.
Na comunidade Maturacá, localizada em São Gabriel da Cachoeira, no noroeste do Amazonas, pelo menos 12 famílias partiram para o interior da floresta. Outros grupos familiares se preparam para seguir o mesmo caminho. “O nosso povo Yanomami está alerta. A hora que chega em São Gabriel essa doença, vamos nos deslocar e estamos fazendo farinhada para a gente se isolar os 40 dias no mato. E a hora que tiver três casos, quatro casos, não vai ficar ninguém na comunidade. Só vai ficar pelotão, missão. Só isso que vai estar aqui na comunidade”, diz José Góes.
Assembleia para discutir turismo no Pico da Neblina, em Maturacá (Foto: João Claudio Moreira/Amazônia Real)
Em Boa Vista, capital de Roraima, o vice-presidente da Hutukara Associação Yanomami, Dario Vitório Kopenawa explica que esse movimento de isolamento no interior da floresta amazônica não é uma tarefa fácil para os Yanomami. Muitas das comunidades se fixaram perto de locais onde há posto de saúde. É por isso que há divisão entre quem se refugiou na floresta e quem permaneceu na comunidade. “Algumas minorias foram para o isolado. A maioria ainda está na comunidade, ficando isolado na maloca”, explica.
Dario acompanha a movimentação dos Yanomami para dentro da floresta, recebendo informações via radiofonia, da sede da Hutukara, e relata que a ida para o mato vem acontecendo no Marauiá (região do Rio Marauiá); Parawa-u e Demini, todos no Amazonas. Em Roraima, é o subgrupo Ninam que segue a mesma estratégia. A família de Dario – inclusive seu pai, a liderança e xamã Yanomami Davi Kopenawa -, está na região Demini, buscando proteção na floresta.
Também via rádio, o vice-presidente da Hutukara tem notícias de que os xamãs vêm trabalhando na tentativa de conhecer a doença. “Pandemia coronavírus para nós é xawara. Os Yanomami pajés e médicos da floresta estão trabalhando reconhecendo essa doença. Assim os xamãs me falaram”, diz Dario Kopenawa.
O isolamento em São Gabriel
Fiscais orientam população em São Gabriel da Cachoeira na terça-feira, 28 de abri (Foto: Paulo Desana/Dabakuri/Amazônia Real)
A viagem da sede de São Gabriel da Cachoeira para Maturacá leva cerca de 10 horas, dependendo das condições da estrada e de navegação pelo Rio Negro e seus afluentes. No domingo (26), a prefeitura do município confirmou os dois primeiros casos de coronavírus e, no dia seguinte, houve a confirmação outros dois. É grande a possibilidade de já estar havendo a transmissão comunitária. Desses quatro pacientes, três são indígenas e um é militar do Exército.
José Mário Góes, presidente da Associação Yanomami do Rio Cauaburis e Afluentes (Ayrca), está em Maturacá e respondeu à reportagem da Amazônia Real por meio da mensagem de áudio de WhatsApp. O acesso à internet é possível porque durante parte do dia eles conseguem captar o sinal pela proximidade com o 5º Pelotão Especial de Fronteira do Exército.
“Quando uma família vai, outras famílias vão, a vizinhada vai. Porque na comunidade somos todos parentes, então eles levaram toda a família”, disse a liderança indígena. Cada grupo está construindo pequenos abrigos para morar por cerca de 40 dias. Além de se manterem com frutas, caça e pesca, levam alimentos. Se for necessário, voltam à comunidade para reforçar os mantimentos. “Levaram alimentos principais como farinha, banana, tapioca, beiju, e também café, açúcar, arroz, feijão e materiais de caça e pesca. E quando acaba os alimentos eles vêm buscar banana, pegar estoque de farinha”, relata Góes.
“Deixar as casas e ficar por um tempo na floresta é uma estratégia que algumas famílias já estão fazendo. Diferente de nós que estamos enfrentando pela primeira vez uma epidemia, os Yanomami têm experiências recentes que dizimaram comunidades inteiras e os sobreviventes foram os que se isolaram no mato”, explica o assessor do Programa Rio Negro do Instituto Socioambiental (ISA), Marcos Wesley de Oliveira.
Essa estratégia pode ser comparada ao isolamento social recomendado pela Organização Mundial da Saúde (OMS) e pelo Ministério da Saúde, aponta Marcos Wesley. “Os Yanomami sabem que até o momento não há remédio ou vacina eficazes contra a Covid-19”, reforça.
O município de São Gabriel da Cachoeira tem uma população de mais de 45 mil habitantes, a maioria indígenas de 23 etnias, segundo a taxa atualizada do Censo do IBGE. Desse total, 25 mil moram nas aldeias e comunidades, em territórios demarcados, segundo a Federação das Organizações Indígenas do Rio Negro (Foirn).
Para evitar que os indígenas de Maturacá, cuja população total é de cerca de 2.000 pessoas, façam a viagem até São Gabriel para fazer compras, o ISA e a Foirn enviam cestas básicas e kits de higiene para a comunidade. Esse material será levado por avião do Exército, segundo protocolo de higienização e distribuição para evitar a contaminação da Covid-19.
Em artigo publicada na Amazônia Real, o antropólogo francês Bruce Albert citou um trecho do livro A queda do Céu, escrito em conjunto por ele e pelo xamã e líder Davi Kopenawa Yanomami, para falar sobre a morte do jovem, em Boa Vista. O adolescente foi sepultado sem o conhecimento dos pais e sem o respeito aos rituais de seu povo. Ao tratar do tema funeral, o antropólogo sugeriu ao leitor “reler A queda do Céu, pp. 267-68, onde Davi Kopenawa conta como sua mãe morreu numa epidemia de sarampo trazida pelos missionários da Novas Tribos do Brasil (aliás, Ethnos360) e como estes sepultaram o cadáver à revelia num lugar até hoje desconhecido: Por causa deles, nunca pude chorar a minha mãe como faziam nossos antigos. Isso é uma coisa muito ruim. Causou-me um sofrimento muito profundo, e a raiva desta morte fica em mim desde então. Foi endurecendo com o tempo, e só terá fim quando eu mesmo acabar. ”
Movimento nas ruas de São Gabriel da Cachoeira na manhã de segunda-feira (27/04/2020) (Foto: Paulo Desana/Dabakuri/Amazônia Real)
A morte do adolescente Yanomami despertou o temor desse povo, inclusive em Maturacá. “Essa morte traz alerta para que isso não acabe com povo Yanomami. Como aconteceu na região do Irokae, morrendo adultos, jovens e crianças, os idosos, como aconteceu isso não queremos que aconteça mais. Por isso estamos alerta por aqui”, afirma José Mário Góes.
Irokae é o primeiro acampamento para o Pico da Neblina, denominado pelos Yanomami de Yaripo, a Montanha de Vento. Essa trilha seria reaberta para o turismo em abril, mas foi adiada devido à pandemia. Anos atrás, na tentativa de fugir da coqueluche, os grupos seguiram por esse caminho, mas alguns acabaram morrendo.
“Essa doença de agora, o coronavírus, aqui em Maturacá, representa epidemia de coqueluche como aconteceu na região de Irokae. O que está acontecendo com os napë (forasteiro, homem branco), isso já aconteceu aqui para nós Yanomami na região do Irokae, onde fica a trilha do Yaripo”, relata José Mário. “Nossos avós já tiveram outra doença, como epidemia de coqueluche, que matou muitas crianças e os mais velhos. Eles não querem que repita essa história. Morreu até um pajé nessa epidemia. Então como fizeram agora, eles foram para a floresta, na região do frio, chegaram até lá no pico. É lá que ficam os restos mortais dos nossos parentes e por isso que nós falamos que temos histórias no caminho do Yaripo”, relata José Góes.
Outro problema enfrentado no passado foi o sarampo. “Aqui na comunidade, em Maturacá, onde está situado o polo base de saúde. Então era um xapono (casa coletiva) onde tivemos epidemia de sarampo. Também nós fizemos o movimento como estamos fazendo hoje aqui, mas não teve jeito. Pessoas fugiram, mas teve óbito nas crianças. Morreu muita criança e adulto. É a mesma história que eles não querem que repita. ”
Para os Yanomami, o vírus é um tipo de envenenamento. “Nós observamos que o próprio napë faz envenenamento no ser humano para dizer que é vírus. Isso é epidemia, é um vírus que afeta qualquer ser humano e acaba com a vida do ser humano. Isso tem na nossa realidade como aconteceu com nossos antepassados o que está acontecendo hoje no mundo inteiro. Até no Brasil e no exterior”, diz José Góes.
Em busca de proteção, os Yanomami recorrem a ensinamentos de seus antepassados. Após a confirmação dos casos em São Gabriel, as lideranças tradicionais iniciaram a chamada “recura’ para que a doença saia do lugar e seja levada pelo vento para onde não tem ser humano.
Summary: Ethicists are calling on the global research community to resist treating the urgency of the current COVID-19 outbreak as grounds for making exceptions to rigorous research standards in pursuit of treatments and vaccines.
Ethicists from Carnegie Mellon and McGill universities are calling on the global research community to resist treating the urgency of the current COVID-19 outbreak as grounds for making exceptions to rigorous research standards in pursuit of treatments and vaccines.
With hundreds of clinical studies registered on ClinicalTrials.gov, Alex John London, the Clara L. West Professor of Ethics and Philosophy and director of the Center for Ethics and Policy at Carnegie Mellon, and Jonathan Kimmelman, James McGill Professor and director of the Biomedical Ethics Unit at McGill University, caution that urgency should not be used as an excuse for lowering scientific standards. They argue that many of the deficiencies in the way medical research is conducted under normal circumstances seem to be amplified in this pandemic. Their paper, published online April 23 by the journal Science, provides recommendations for conducting clinical research during times of crises.
“Although crises present major logistical and practical challenges, the moral mission of research remains the same: to reduce uncertainty and enable care givers, health systems and policy makers to better address individual and public health,” London and Kimmelman said.
Many of the first studies out of the gate in this pandemic have been poorly designed, not well justified, or reported in a biased manner. The deluge of studies registered in their wake threaten to duplicate efforts, concentrate resources on strategies that have received outsized media attention and increase the potential of generating false positive results purely by chance.
“All crises present exceptional situations in terms of the challenges they pose to health and welfare. But the idea that crises present an exception to the challenges of evaluating the effects drugs and vaccines is a mistake,” London and Kimmelman said. “Rather than generating permission to carry out low-quality investigations, the urgency and scarcity of pandemics heighten the responsibility of key actors in the research enterprise to coordinate their activities to uphold the standards necessary to advance this mission.”
The ethicists provide recommendations for multiple stakeholder groups involved in clinical trials:
Sponsors, research consortia and health agencies should prioritize research approaches that test multiple treatments side by side. The authors argue that “master protocols” enable multiple treatments to be tested under a common statistical framework.
Individual clinicians should avoid off-label use of unvalidated interventions that might interfere with trial recruitment and resist the urge to carry out small studies with no control groups. Instead, they should seek out opportunities to join larger, carefully orchestrated studies.
Regulatory agencies and public health authorities should play a leading role in identifying studies that meet rigorous standards and in fostering collaboration among a sufficient number of centers to ensure adequate recruitment and timely results. Rather than making public recommendations about interventions whose clinical merits remain to be established, health authorities can point stakeholders to recruitment milestones to elevate the profile and progress of high-quality studies.
“Rigorous research practices can’t eliminate all uncertainty from medicine,” London and Kimmelman said, “but they can represent the most efficient way to clarify the causal relationships clinicians hope to exploit in decisions with momentous consequences for patients and health systems.”

































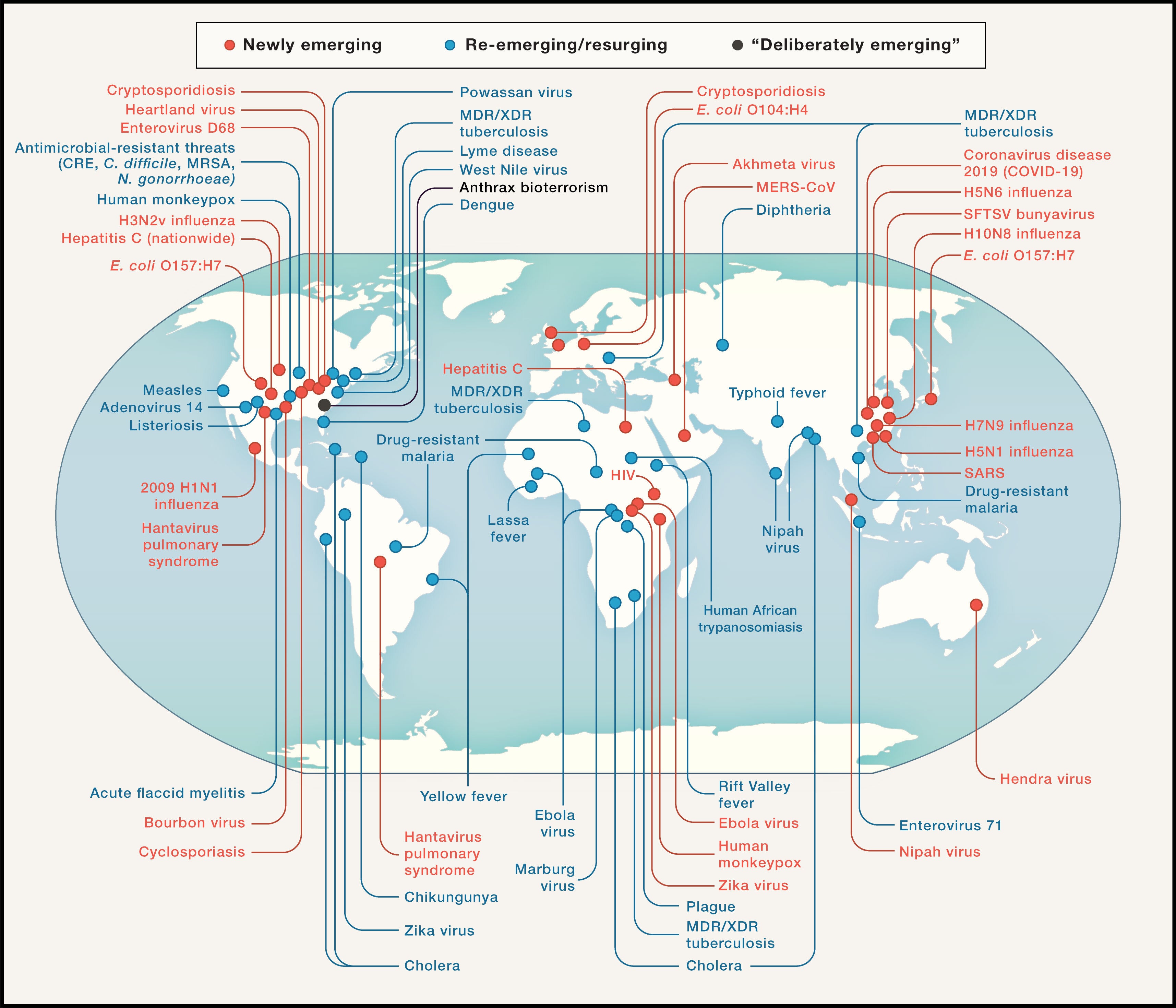



")
")
/i.s3.glbimg.com/v1/AUTH_59edd422c0c84a879bd37670ae4f538a/internal_photos/bs/2020/s/c/wUxBKDTaiIlLNK9x29fQ/wuhanaulas.jpg)
/i.s3.glbimg.com/v1/AUTH_59edd422c0c84a879bd37670ae4f538a/internal_photos/bs/2020/7/H/UeNmVASiin7zVCWpdAJw/2020-05-28t144506z-361001322-rc2qxg9fincr-rtrmadp-3-health-coronavirus-safrica.jpg)
/i.s3.glbimg.com/v1/AUTH_59edd422c0c84a879bd37670ae4f538a/internal_photos/bs/2020/y/7/qoIKPsT7GCtryEJUyYxg/000-1qu224.jpg)
/i.s3.glbimg.com/v1/AUTH_59edd422c0c84a879bd37670ae4f538a/internal_photos/bs/2020/4/6/6A8Zs5T9qBiAlwXu01IA/000-1sd0zw.jpg)
/i.s3.glbimg.com/v1/AUTH_59edd422c0c84a879bd37670ae4f538a/internal_photos/bs/2020/t/A/bUAgUGQwuPe3a7eZcCwQ/000-1qu2c5.jpg)
/i.s3.glbimg.com/v1/AUTH_59edd422c0c84a879bd37670ae4f538a/internal_photos/bs/2020/H/I/BFlIj7RBOdJcZ2nWNL3A/000-1ru1vc.jpg)
/i.s3.glbimg.com/v1/AUTH_59edd422c0c84a879bd37670ae4f538a/internal_photos/bs/2020/q/B/ZFi1jcT0CWfFx0lDSzYg/lavar-maos.jpg)
/i.s3.glbimg.com/v1/AUTH_59edd422c0c84a879bd37670ae4f538a/internal_photos/bs/2020/X/8/QE9FrdR7KeT10ah80f0w/2020-05-18t101008z-295272890-rc2yqg957d8k-rtrmadp-3-health-coronavirus-portugal.jpg)
/i.s3.glbimg.com/v1/AUTH_59edd422c0c84a879bd37670ae4f538a/internal_photos/bs/2020/6/4/gtmem5TQeubrA0gMqhog/2020-05-15t115216z-1634726545-rc2xog95qjse-rtrmadp-3-health-coronavirus-belgium-schools.jpg)
/i.s3.glbimg.com/v1/AUTH_59edd422c0c84a879bd37670ae4f538a/internal_photos/bs/2020/x/C/ScTmbFTTKQLsYi1IriSw/aula.jpg)
/i.s3.glbimg.com/v1/AUTH_59edd422c0c84a879bd37670ae4f538a/internal_photos/bs/2020/O/g/oryj7lQFGbHBJbJ9jD9Q/asas.jpg)
/i.s3.glbimg.com/v1/AUTH_59edd422c0c84a879bd37670ae4f538a/internal_photos/bs/2020/I/i/NcbMEoSRqxfjw2NA37fQ/coronavirus-27-04-2020-2020-04-27t115918z-411447450-rc2xcg9crq3w-rtrmadp-3-health-coronavirus-china-china-daily-reuters.jpg)







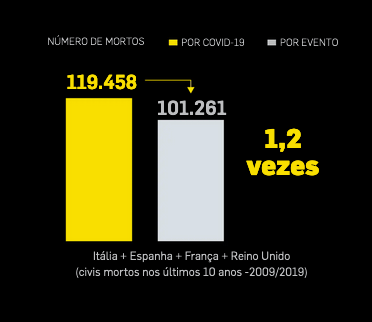





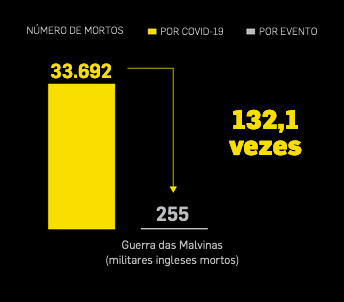











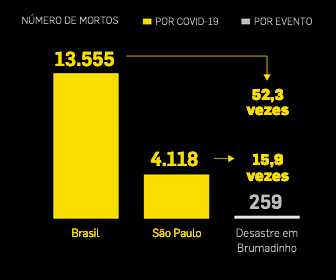




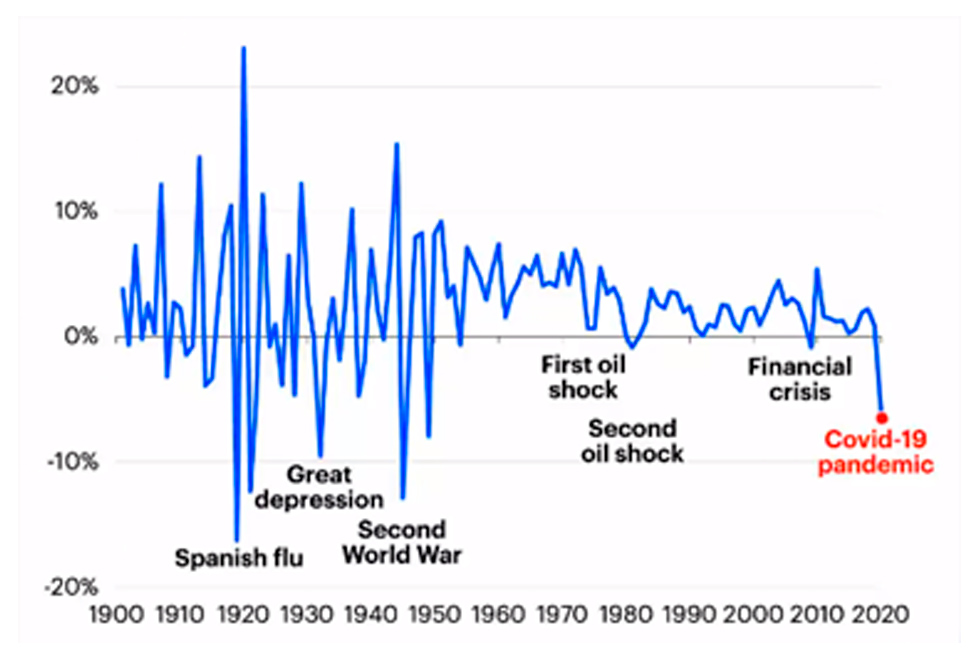
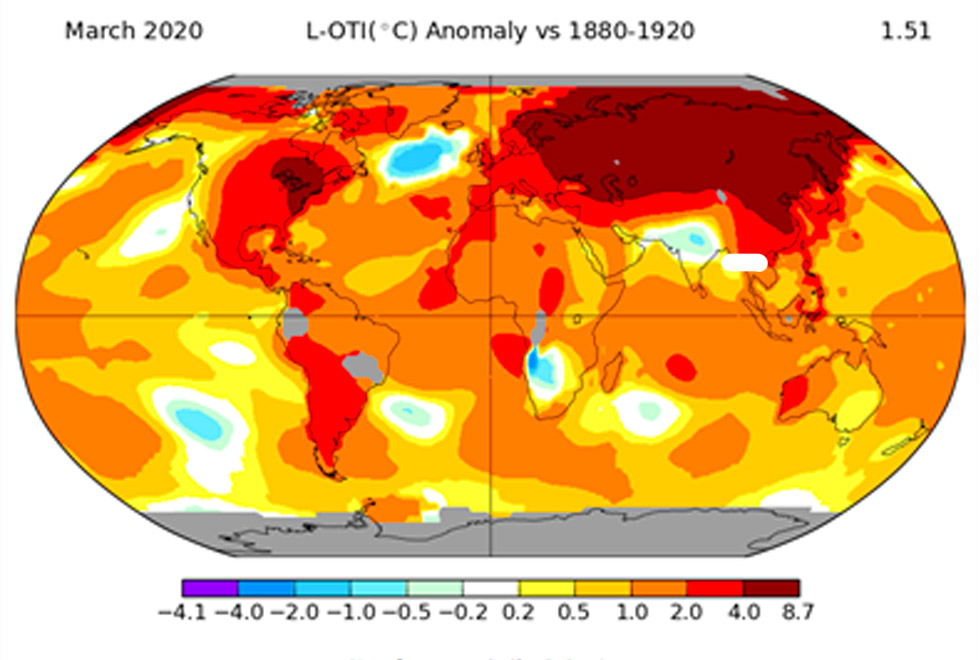







Você precisa fazer login para comentar.