By Paul Richards March 17, 2020
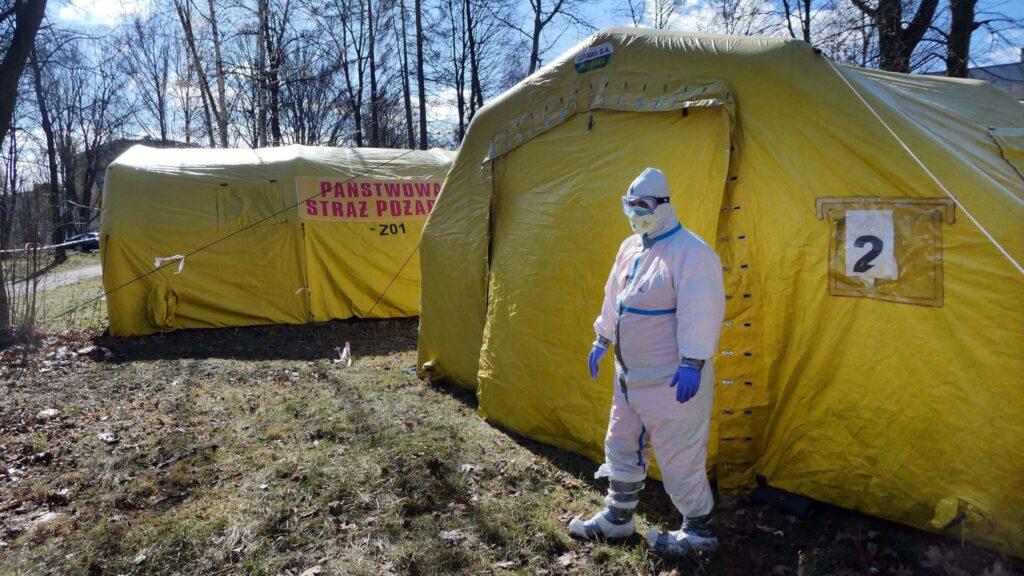
A medical official outside an emergency tent installed for patients infected by COVID-19 in Poland- Credit Sky News
Covid-19 is a flu-like illness (symptoms include fever, cough, and breathing problems) caused by a corona virus (SARS CoV-2). Like Ebola, the virus causing Covid-19 circulates within populations of bats and crossed over to humans via the bush meat trade. The first human cases were identified in China in December 2019, and the infection has now (March 2020) reached more than 100 countries.
The disease is now recognised by the World Health Organization as a pandemic. Up to 80 percent of the population of some countries might eventually become infected. Most cases will be mild, and recovery spontaneous. About 5 percent of cases will be life-threatening. Death rates appear to be around 1-2 percent. The elderly are most at risk.[1]
Currently, attention is focused on reducing the rate at which Covid-19 spreads. One aim is to delay the peak of infection beyond the winter flu period in the northern hemisphere, when medical help is stretched. Slowing the epidemic also allows more time for preparation of health systems to cope with large numbers, and for work on vaccine development.
Predictably, some politicians have demanded border closures against immigrants and refugees, even though spread is associated with tourism and normal business travel. Africans internationally stigmatised by Ebola might feel aggrieved that cases of Covid-19 have been introduced from Europe and Asia. But in a globally connected and inter-dependent world blaming and stigmatising helps no one. It is better to share ideas about what can be done to protect.
This is where Africa’s experience of Ebola has something to offer. Communities experiencing Ebola in West Africa in 2014-15 rapidly learnt from scratch how to cope with a deadly new infection, and this provides the rest of the world with important information on strategies to address novel disease threats more generally.
Like Ebola, Covid-19 is a family disease, in the sense that many infections occur in the home. Restrictions on travel can slow the spread of the disease, but it also helps if individuals and families understand infection pathways and implement domestic precautions. This is something in which West Africans confronted by Ebola have had much experience.
History of Pandemics – credit Virtual Capitalists
The name for Ebola in Mende, one of the main languages of Sierra Leone, the worst affected country in 2014-15, was bonda wote, literally ‘family turn round’. In other words, it was clearly recognised that this was a disease requiring families to change behaviour in major ways, especially in how they cared for the sick.
Covid-19 will require similar changes at the family level, especially in terms of how the elderly are protected. The buzz words for epidemic responders include self-isolation and social distancing, but the details of how to implement these vague concepts have been left to local social imagination.
Answers are required for both the uninfected elderly, and for others who are sick.
Should grandpa be packed off to a shed in the garden away from the family for his own protection? What happens when grandma gets lonely and wants to see the grandchildren? Who does the shopping? How does the daily-paid worker ‘self-isolate’ when there is no sick pay? Who collects the children from school when a single mum is sick?
Much depends on actual family arrangements and housing stock. So African solutions for Ebola will not work directly in other parts of the world. But it is important to know that under the challenge of Ebola local people showed much inventiveness in devising solutions to such problems.
Evidence shows that ways can be found to reduce family risks of infection, even with a disease 30 times more deadly than Covid-19.[2]For Ebola, these ranged from the elbow knock that replaced shaking of hands as a public greeting, to the appointment of a single carer in the household to look after the sick while waiting for help, to the carefully choreographed ‘safe and respectful’ funerals that allowed some element of local ritual back into the burial process, a major source of infection.
Every encouragement should be given to this local adaptive creativity, and the authorities should listen carefully to information from below about what would help to make a difference.
However, Covid-19 is not Ebola, and differences have to be taken into account. Some of the major questions about how the disease spreads are as yet unknown, and citizens and households need to be listening for this information as it becomes available and helped to adapt to its implications in real time.
This implies having very good means of two-way communication. In Sierra Leone a telephone helpline, ‘117’, played an important part in arranging emergency Ebola response, but it was much poorer at harvesting feedback from communities about what could be done better.
It seems that the lesson has not been learnt with Covid-19. In Britain, the National Health Service helpline, ‘111’ has now been ‘stood down’ for Covid-19 enquiries relating to domestic testing, since the epidemic is deemed to have passed into a new phase. How then are the authorities to have a conversation with families about the resources most needed for adaptation at household level?
Case-handling is a second area of difference. Ebola does not spread easily. The virologist Peter Piot put it well when he stated that he would have no problem sitting next to someone with Ebola provided they were not vomiting over him. Infection spreads only through contact with body fluids. Covid-19, however, spreads through the air, as well as via bodily contact, and case numbers will be much higher.
With Ebola in West Africa the number of cases turning up at specialist Ebola care facilities at the height of the epidemic numbered in tens or hundreds per week. With Covid-19 the numbers of cases requiring intensive care at the peak of the epidemic may amount to hundreds of thousands.
Even if stretched out over several months infection on this scale implies a large extra demand for medical care.
Ebola taught that epidemics cause deaths from other diseases through their impact on health systems. In all there were about 12,000 Ebola deaths in Upper West Africa (Guinea, Liberia, Sierra Leone) in 2014-15 but many additional fatalities resulted from, for example, closure of facilities such as maternity clinics.
So contingency planning is required. A key challenge for Covid-19 is how health system care should best be organized, without severely disrupting other forms of health provision.
For Ebola, the first response was to build large field hospitals (Ebola Treatment Centres).[3]These were seen as the safest option. But they were shunned by families, because so few patients came out alive. They were also often in the wrong place (built behind, not ahead, of the epidemic).
Information started to filter through that some communities were taking their own steps to reduce infection and bury the dead. This raised the question whether there was more scope for community care.
Family do-it-yourself responses proved controversial. International responders were adamant that there would be nothing resembling home care; it was too dangerous. Local communities were equally adamant that there would have to be some form of home care; they could not stand by and watch family members die, when an ambulance to take a patient to an ETC might take days to arrive over bad or non-existent roads.
Families saw it as their duty to be involved in care of the sick. So, they repeatedly asked what to do while waiting for help to arrive. Could they not prepare food for the sick? Could they not be trained to safely bury the dead?
No, they were told. Ebola required specialist management.
Communities answered back. They pointed to areas at the outset of the epidemic, where the epidemic was rolled back with only local resources. In Kailahun District, for example, an intense initial outbreak was reduced to a trickle of cases by local responders organizing quarantine and burial with improvised resources. That cases then declined without outside help implied either that the disease burnt out more readily than anticipated, or that local improvisation worked better than expected. There is evidence to support both interpretations.[4]
Experts knew that Ebola control required prompt diagnosis, before the ‘wet’ symptoms of the disease became apparent. Something had to be done to speed up the presentation of cases. The answer was to build much smaller community care centres (CCC) close to where active transmission was taking place.[5]This also changed the relationship between families and Ebola responders from fear to active cooperation.
Staff of CCC were for the most part local volunteers – trained nurses who had not been absorbed on to the payroll of the Ministry of Health, or villagers willing to take on high-risk chores for a decent wage. The fact that staffing was local meant patients saw familiar faces, and this built trust. CCC also normalized Ebola by bringing treatment within a framework of general medical assistance.
As a result, patients were presented more promptly than was the case with the distant ETC. Ebola (indistinguishable from malaria or typhoid in its early phase) was more rapidly identified and isolated. One study estimates that CCC contributed up to one third of the infection control ending the epidemic in Sierra Leone.[6]
This example of responders modifying their approach to infection control better to accommodate family requirements may hold lessons for Covid-19.
Specifically, cases may have to be kept out of main hospitals as much as possible, Thus, there may be a need for field treatment facilities not dissimilar to CCC, as a half-way house between home isolation and intensive care. In effect these facilities would isolate and triage the most vulnerable cases, as was the case with Ebola CCC.
There is also a possibility that any such facilities might be run up by military personnel[7]and staffed by medically trained ‘volunteers’ (retired doctors and nurses), as in Sierra Leone.
Interesting to note, the chief medical advisor for England was previously one of the proponents of the introduction of CCC in Sierra Leone, and we may be about to see some lessons directly transferred.[8]
Quarantine for Ebola in Sierra Leone is also an issue from which Covid-19 responders might wish to draw lessons. Much of it was organised and imposed by the state, and was at times heavy-handed. But communities also organised their own quarantine. They understood that self-isolation was in their own interest, and this sometimes worked surprisingly effectively.
Use was made of an approach used during the civil war of 1991-2002 of mobilising community youth to identify infiltrators. Visitors who might have been carrying the virus were turned away. But in other cases the approach was more focused on sequestering those who were well. Rural families sometimes decamped from villages with outbreaks to settle down for a few weeks in their farms, where sleeping quarters were sometimes built for the purpose.
In this respect, Sierra Leonean rural communities showed a clear appreciation of the fact that there were two distinct kinds of quarantine – self-isolation and protective sequestration. Both kinds are being used as part of the response to Covid-19, but at times without adequate discussion of how the two types differ and have different social motivations – self-protection and altruism towards neighbours. It is not wise to talk about self-isolation for the sick and the elderly in the same breath. The different motivations need to be more clearly explained.
In conclusion, it is also important to say something about what Africa can learn from its own experience of Ebola. The point made above should be reiterated – about the differences as well as similarities between Covid-19 and Ebola.
Prompt case finding, contact tracing and quarantine are being applied to Covid-19 as they were for Ebola.[9]Good hygiene practices, such as hand washing, also remain applicable. African countries with experience of Ebola know how to do these things, and this will be helpful in dealing with early cases.
However, African countries also have to be prepared to learn to adapt to the specific features of this new disease as more data emerge. This will pose more of a challenge, since this will require rapid knowledge-based domestic adaptation to new information on how Covid-19 spreads (perhaps most notably, why it affects the old more than the young, and how older people might be best protected from its effects).
The main lesson for both Africa and other parts of the world from Ebola for Covid-19, however, is that shared learning between communities and medical professionals is a key aspect of human adaptive response to emergent diseases. In any disease in which community mobilization is an important aspect families need to think like epidemiologists, but equally epidemiologists need to think like families.

Paul Richards’ Ebola book front cover, part of the African Arguments book series
References:
[1]Xu, J., Zhao, S., Teng T., Abdalla, A.E., Zhu, W., Xie, L., Wang, Y., Guo, X. (2020) ‘Systematic comparison of two animal-to-human transmitted human coronaviruses: SARS-CoV-2 and SARS-CoV’, Viruses 12, 244.
[2]Richards, P. (2016) Ebola: How a People’s Science Helped End an Epidemic, London: Zed Books.
[3]Richards, P., Mokuwa, E., Welmers, P., Maat, H., Beisel, U. (2019) ‘Trust, and distrust, of Ebola Treatment Centers: a case-study from Sierra Leone’, PLoS ONE14(12): e0224511. https://doi.org/10.1371/journal.pone.0224511.
[4]Glynn, Judith R. et al. (2017) ‘Asymptomatic infection and unrecognised Ebola virus disease in Ebola-affected households in Sierra Leone: a cross-sectional study using a new non-invasive assay for antibodies to Ebola virus’,Lancet Infectious Diseases17(6), 645-653. On local case finding, quarantine and burial procedures see Richards (2016) op. cit.
[5]Mokuwa, E.Y., Maat, H. (2020) ‘Rural populations exposed to Ebola Virus Disease respond positively to localised case handling: evidence from Sierra Leone’, PLoS Negl Trop Dis 14(1): e0007666. https://doi.org/10.1371/journal.pntd.0007666.
[6]Pronyk, P., Rogers, B., Lee, S., Bhatnagar, A., Wolman, Y., Monasch, R., Hipgrave, D., Salama, P., Kucharski, A., Chopra, M., and on behalf of the UNICEF Sierra Leone Ebola Response Team, (2016) ‘The effect of community-based prevention and care on Ebola transmission in Sierra Leone’,American Journal of Public Health 106, 727–32, https://doi.org/10.2105/AJPH.2015.303020.
[7]Aaaron Walawalkar and Jamie Grierson, The Guardian,8 March 2020, 14.12 GMT.
[8]Whitty, C.J.M., Farrar, J., Ferguson, N., Edmunds, W.J., Piot, P., Leach, M., Davies, S.C. (2014) ‘Tough choices to reduce Ebola transmission’, Nature515, 13 November, 192–4; see also Ian Sample and Lisa O’Carroll ‘Prof Chris Whitty – the expert we need in the coronavirus crisis’, Guardian,4 March 2020.
[9]Hellewell, J. et al. (2020) ‘Feasibility of controlling Covid-19 outbreaks by isolation of cases and contacts’, Lancet, 28 February 2020, https://doi.org/10.1016/S2214-109X(20)30074-7.

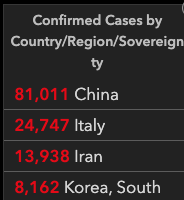







 Foto: Marcelo Casal Jr/Agência Brasil
Foto: Marcelo Casal Jr/Agência Brasil 




















Você precisa fazer login para comentar.