We’ve made our coronavirus coverage free for all readers. To get all of HBR’s content delivered to your inbox, sign up for the Daily Alert newsletter.
Some of the HBR edit staff met virtually the other day — a screen full of faces in a scene becoming more common everywhere. We talked about the content we’re commissioning in this harrowing time of a pandemic and how we can help people. But we also talked about how we were feeling. One colleague mentioned that what she felt was grief. Heads nodded in all the panes.
If we can name it, perhaps we can manage it. We turned to David Kessler for ideas on how to do that. Kessler is the world’s foremost expert on grief. He co-wrote with Elisabeth Kübler-Ross On Grief and Grieving: Finding the Meaning of Grief through the Five Stages of Loss. His new book adds another stage to the process, Finding Meaning: The Sixth Stage of Grief. Kessler also has worked for a decade in a three-hospital system in Los Angeles. He served on their biohazards team. His volunteer work includes being an LAPD Specialist Reserve for traumatic events as well as having served on the Red Cross’s disaster services team. He is the founder of www.grief.com, which has over 5 million visits yearly from 167 countries.
Kessler shared his thoughts on why it’s important to acknowledge the grief you may be feeling, how to manage it, and how he believes we will find meaning in it. The conversation is lightly edited for clarity.
HBR: People are feeling any number of things right now. Is it right to call some of what they’re feeling grief?
Kessler: Yes, and we’re feeling a number of different griefs. We feel the world has changed, and it has. We know this is temporary, but it doesn’t feel that way, and we realize things will be different. Just as going to the airport is forever different from how it was before 9/11, things will change and this is the point at which they changed. The loss of normalcy; the fear of economic toll; the loss of connection. This is hitting us and we’re grieving. Collectively. We are not used to this kind of collective grief in the air.
You said we’re feeling more than one kind of grief?
Yes, we’re also feeling anticipatory grief. Anticipatory grief is that feeling we get about what the future holds when we’re uncertain. Usually it centers on death. We feel it when someone gets a dire diagnosis or when we have the normal thought that we’ll lose a parent someday. Anticipatory grief is also more broadly imagined futures. There is a storm coming. There’s something bad out there. With a virus, this kind of grief is so confusing for people. Our primitive mind knows something bad is happening, but you can’t see it. This breaks our sense of safety. We’re feeling that loss of safety. I don’t think we’ve collectively lost our sense of general safety like this. Individually or as smaller groups, people have felt this. But all together, this is new. We are grieving on a micro and a macro level.
What can individuals do to manage all this grief?
Understanding the stages of grief is a start. But whenever I talk about the stages of grief, I have to remind people that the stages aren’t linear and may not happen in this order. It’s not a map but it provides some scaffolding for this unknown world. There’s denial, which we say a lot of early on: This virus won’t affect us. There’s anger: You’re making me stay home and taking away my activities. There’s bargaining: Okay, if I social distance for two weeks everything will be better, right? There’s sadness: I don’t know when this will end. And finally there’s acceptance. This is happening; I have to figure out how to proceed.
Acceptance, as you might imagine, is where the power lies. We find control in acceptance. I can wash my hands. I can keep a safe distance. I can learn how to work virtually.
When we’re feeling grief there’s that physical pain. And the racing mind. Are there techniques to deal with that to make it less intense?
Let’s go back to anticipatory grief. Unhealthy anticipatory grief is really anxiety, and that’s the feeling you’re talking about. Our mind begins to show us images. My parents getting sick. We see the worst scenarios. That’s our minds being protective. Our goal is not to ignore those images or to try to make them go away — your mind won’t let you do that and it can be painful to try and force it. The goal is to find balance in the things you’re thinking. If you feel the worst image taking shape, make yourself think of the best image. We all get a little sick and the world continues. Not everyone I love dies. Maybe no one does because we’re all taking the right steps. Neither scenario should be ignored but neither should dominate either.
Anticipatory grief is the mind going to the future and imagining the worst. To calm yourself, you want to come into the present. This will be familiar advice to anyone who has meditated or practiced mindfulness but people are always surprised at how prosaic this can be. You can name five things in the room. There’s a computer, a chair, a picture of the dog, an old rug, and a coffee mug. It’s that simple. Breathe. Realize that in the present moment, nothing you’ve anticipated has happened. In this moment, you’re okay. You have food. You are not sick. Use your senses and think about what they feel. The desk is hard. The blanket is soft. I can feel the breath coming into my nose. This really will work to dampen some of that pain.
You can also think about how to let go of what you can’t control. What your neighbor is doing is out of your control. What is in your control is staying six feet away from them and washing your hands. Focus on that.
Finally, it’s a good time to stock up on compassion. Everyone will have different levels of fear and grief and it manifests in different ways. A coworker got very snippy with me the other day and I thought, That’s not like this person; that’s how they’re dealing with this.I’m seeing their fear and anxiety. So be patient. Think about who someone usually is and not who they seem to be in this moment.
One particularly troubling aspect of this pandemic is the open-endedness of it.
This is a temporary state. It helps to say it. I worked for 10 years in the hospital system. I’ve been trained for situations like this. I’ve also studied the 1918 flu pandemic. The precautions we’re taking are the right ones. History tells us that. This is survivable. We will survive. This is a time to overprotect but not overreact.
And, I believe we will find meaning in it. I’ve been honored that Elisabeth Kübler-Ross’s family has given me permission to add a sixth stage to grief: Meaning. I had talked to Elisabeth quite a bit about what came after acceptance. I did not want to stop at acceptance when I experienced some personal grief. I wanted meaning in those darkest hours. And I do believe we find light in those times. Even now people are realizing they can connect through technology. They are not as remote as they thought. They are realizing they can use their phones for long conversations. They’re appreciating walks. I believe we will continue to find meaning now and when this is over.
What do you say to someone who’s read all this and is still feeling overwhelmed with grief?
Keep trying. There is something powerful about naming this as grief. It helps us feel what’s inside of us. So many have told me in the past week, “I’m telling my coworkers I’m having a hard time,” or “I cried last night.” When you name it, you feel it and it moves through you. Emotions need motion. It’s important we acknowledge what we go through. One unfortunate byproduct of the self-help movement is we’re the first generation to have feelings about our feelings. We tell ourselves things like, I feel sad, but I shouldn’t feel that; other people have it worse. We can — we should — stop at the first feeling. I feel sad. Let me go for five minutes to feel sad. Your work is to feel your sadness and fear and anger whether or not someone else is feeling something. Fighting it doesn’t help because your body is producing the feeling. If we allow the feelings to happen, they’ll happen in an orderly way, and it empowers us. Then we’re not victims.
In an orderly way?
Yes. Sometimes we try not to feel what we’re feeling because we have this image of a “gang of feelings.” If I feel sad and let that in, it’ll never go away. The gang of bad feelings will overrun me. The truth is a feeling that moves through us. We feel it and it goes and then we go to the next feeling. There’s no gang out to get us. It’s absurd to think we shouldn’t feel grief right now. Let yourself feel the grief and keep going.
As of 2019, the Big Picture for humanity was approximately as follows. Homo sapiens (that’s us), a big-brained bipedal mammal, had spent the Pleistocene epoch (from 2.5 million years ago until 12,000 years ago) developing its ability to control fire, talk, paint pictures, play bone flutes, and make tools and clothes. Language dramatically enhanced our sociality and helped enable us to invade and inhabit every continent except Antarctica. During the Holocene epoch (the last 12,000 years), we started living in permanent settlements, developed agriculture, and built state societies with kings, slavery, economic inequality, full-time division of labor, money, religions, and armies. The Anthropocene epoch (more of a brief interlude, really) dawned only a couple of centuries ago as we humans started using fossil fuels, which empowered us dramatically to grow our population and per capita consumption rates, mechanize production and transport, and basically dominate the entire planet. The mechanization of agriculture, by making the landed peasantry redundant, led to mass urbanization and quickly pumped up the size of the middle class. However, the use of fossil fuels destabilized the global climate, while also vastly increasing existing problems like pollution, resource depletion, and the destruction of habitat for most wild creatures. In addition, over the past few decades we learned how to use debt to transfer consumption from the future to the present, based on the risky assumption that the economy will continue to grow forever, thereby enabling future generations to pay for the lifestyle we enjoy now.
In short, the Big Picture was one of ever-increasing power and peril. Suddenly it has changed. A pattern of furious economic growth, consistent over many decades since the dawn of the Anthropocene (with only occasional interruptions, primarily consisting of the Great Depression and two World Wars), has slammed precipitously into the wall of pandemic (un)preparedness. In an effort to limit mortality from the novel coronavirus, governments around the world have put their economies into a state of suspended animation, telling most workers to stay home and to avoid direct contact with others.
How is this development impacting trends that were already underway? Will future generations look back on the coronavirus pandemic as a blip or a game changer? Let’s review a few of the major trends that developed during the Anthropocene and engage in a little informed speculation about how they might be affected by the COVID-19 outbreak.
Climate change: In China, lockdowns of workers and closures of companies have led to a dramatic reduction in greenhouse gas emissions. Over the coming weeks, emissions for the world as a whole could fall by ten percent or more. Note to climate warriors: don’t cheer too loudly; folks who are out of work won’t appreciate gloating greenies.
The world’s response to the coronavirus undermines the argument that governments cannot reduce carbon emissions because doing so would hurt their economies. Clearly, national leaders felt that the more immediate (though, in the larger scheme of things, much less significant) threat of pandemic justified shutting down commerce. Climate activists should now feel emboldened to make the following case: If economic degrowth is what it takes to preserve a habitable biosphere, then world leaders can and must find fair and humane ways to reduce society’s scale of energy usage, resource extraction, manufacturing, and waste dumping—all of which contribute to climate change.
However, the pandemic is not good news for the transition to renewable energy. Supply chains for solar and wind companies have been disrupted, and demand for new installations is down. And with super-cheap oil and gas in the offing (see “Resource Depletion,” below), market forces are likely to hinder rather than help both the renewables industry and the shift to electric cars.
Economic inequality: For the gig economy, and for people living paycheck to paycheck (which includes up to 74 percent of Americans earning hourly wages), the coronavirus lockdown is a catastrophe. Over the short term, existing economic inequalities will result in highly unequal levels of sacrifice and suffering. It may be relatively easy for low-wage workers to rationalize a mandated week or two at home as a forced vacation, but if tens of millions of Americans with no savings experience several months without income, regional social stresses could build to the breaking point. That’s one reason government officials are talking about cash handouts.
Over the longer term, recent absurd levels of inequality could get seriously snipped. In his book The Great Leveler, historian Walter Scheidel argues that, in the past, economic inequality has been reversed most dramatically by what he calls the “Four Horsemen”—mass mobilization for warfare, transformative revolution, state collapse, and plague. Currently many governments are undertaking economic re-allocation efforts equivalent in scale to those seen in the World Wars. For example, Denmark is paying 75 percent of wages (for salaries up to ~$50k/year) for companies that would otherwise have to lay off workers, for a period of three months. This not only enables quarantined workers to survive, but allows them to stay on the payroll and not have to go through a rehiring process later.
Thus, the current pandemic might arguably qualify as two of Scheidel’s Horsemen (mass mobilization and plague). The investor class is witnessing capital destruction at a prodigious rate and scale, while government efforts at maintaining civility and social well-being may entail providing a safety net for those with the least. Of course, this isn’t the way social justice advocates envisioned reining in inequality, but the result may end up being equivalent to another New Deal, and possibly even a Green New Deal.
Biodiversity loss: The novel coronavirus pandemic almost certainly began in wild animal markets in Wuhan, China. As Carl Safina put it in a recent article, “Humans caused the pandemic by putting the world’s animals into a cruel blender and drinking that smoothie.” While there have been other zoonotic epidemics in recent years, including HIV, the Marburg virus, SARS, and the 2009 H1N1 “swine flu” pandemic, the global coronavirus outbreak could provide a teachable moment, when wildlife conservation organizations can call successfully for an international moratorium on the trade or sale of any non-domesticated animal species (with zoos providing a highly regulated exception).
Otherwise, don’t expect much of a change in the overall declining trend in the numbers of insects, reptiles, amphibians, and wild birds and mammals with which we share this little planet.
Overpopulation: A few cynical millennials have called the novel coronavirus the “Boomer Remover” due to its tendency to attack the elderly with greatest virulence. Because humanity has recently been adding 80 million new members per year (births minus deaths), an erasure of one year’s net growth in population is possible in a worst-case scenario. However, the potential for a short-term moderation of our overall pattern of demographic expansion could be at least partly offset by the results, starting nine months from now, of hundreds of millions of people of reproductive age worldwide staying home for weeks with little to keep them busy. For wealthy nations with falling fertility levels, a much bigger threat to human population stability will likely continue to be posed by the buildup of endocrine-disrupting chemicals in the environment. For poor nations with high population growth trends, equal education opportunities for everyone regardless of gender will substantially help reduce growth rates.
Resource depletion: With manufacturing on the skids, demand and hence prices for most commodities are plummeting. The world’s most economically crucial commodity, oil, has seen its price fall from $50 a barrel to close to $20 (as of this writing); some analysts are forecasting prices in the single digits. With oil usage crashing, petroleum storage capacity will run out, at which point producers will have no choice but to mothball some oil wells. Oil companies will likely be bailed out, but cannot be profitable under current conditions. The prospect of ever ramping world oil extraction rates back up to recent levels seems dim. It is likely, then, that the long-anticipated moment of the world oil production peak has already occurred, with little fanfare, in November, 2018.
Of course, the blowout in oil markets is a result of economic disaster rather than sound policies of resource conservation. Therefore, adaptation on the part of industry and society as a whole will be chaotic. The international implications are fraught and hard to predict: several key Middle Eastern nations will see their economies shredded by low oil prices, and Great Powers (specifically, China and Russia) may seek to take advantage of the moment by seeking to realign alliances in the region.
Pollution: Marshall Burke of Stanford University has recently written that “the reductions in air pollution in China caused by this economic disruption likely saved 20 times more lives in China than have currently been lost due to infection with the virus in that country.” Reduced rates of manufacturing and consumption should help to reduce overall pollution, but of course this is the side effect of crisis, not the result of sound policy. Therefore, without environmental policy interventions, there’s no reason to expect pollution reduction benefits to be sustained. Just one example of how some temporary benefits could be balanced by new harms: The use of single-use plastics is likely to increase during the pandemic response.
Global debt bomb: The world economy is again in a deflationary moment, as it was in 1932 and 2008. For central banks and governments, all fiscal efforts will be geared toward re-inflating an economy that is otherwise hissing and flattening. There is a heightened risk that investors will realize that, in a no-growth world, their financial instruments are inherently worthless, forcing not just a collapse of the market value of stocks, but a repudiation of the very rules of the game. However, since the coronavirus epidemic itself will eventually subside, the more likely outcome is a period of defaults and bankruptcies mitigated by heroic levels of Fed bond purchases, and government bailouts (of the oil and airline industries, just for starters) and deficit spending. Eventually, if money printing goes exponential, hyperinflation is a possibility, but not soon. Big takeaway: the financial system has been destabilized and, like the oil industry, may never return to “normal.”
* * *
Let’s return to the question posed above: Will humanity look back on the coronavirus pandemic as a blip or a game changer? The likely answer depends partly on how long the pandemic lasts, and that, in turn, will depend largely on how soon tests become widely available, and when treatments and vaccines are found. US Government documents marked “not for public release” suggest significant shortages not just of medical equipment, but also of general goods over the next 18 months for government, industry, and private citizens, if solutions are not quickly forthcoming.
The level at which the game is changed also depends on the degree of downturn in employment and GDP. Fred Bullard, President of the St. Louis Fed, has gone on record saying that the US unemployment rate may hit 30 percent in the second quarter because of shutdowns to fight the coronavirus, and that GDP could drop 50 percent. This would be economic carnage far beyond the scale of the Great Depression (the United States unemployment rate in 1933 was 25 percent; its GDP fell an estimated 15 percent). If the global economy falls that far, and remains locked down even for a few weeks, label the coronavirus “game changer, big time.”
But a change to what? Dystopian possibilities come only too readily to mind. However, in conversation, some of my think-tank colleagues have suggested the pandemic could turn out to be a “Goldilocks” crisis that would disrupt the global order just enough, and in such a way, as to foster a response that sets at least some societies on a trajectory toward cooperation, redistribution, and degrowth.
First, governments often deal with shortages (foreseen in the report cited above) through the tried-and-true strategy of quota rationing. As Stan Cox details in his indispensable book Any Way You Slice It: The Past, Present, and Future of Rationing, quota rationing doesn’t always work well; but when it does, the results can be fairly admirable. During both World Wars, Americans participated enthusiastically in rationing programs for food, tires, clothing, and more. Britain continued its rationing programs well after the end of WWII, and surveys showed that, during the period of rationing, Britons were generally better fed and healthier than either before or after. In most imaginary scenarios for deliberate economic degrowth, quota rationing programs for energy and materials figure prominently.
Cox concludes that rationing programs tend to be more successful when people are united against a common enemy, and when shortages are believed to be temporary. Despite President Trump’s efforts to dub it the “Chinese virus,” SARS-Cov-2 has no inherent nationality, nor is it Democrat or Republican. It is indeed a common enemy, and people tend to become more cooperative when faced with a collective threat. Further, epidemiologists agree that the threat will have an end point, even if we don’t know exactly when that will be. Therefore, conditions for success in rationing exist, and rationing could help foster more communitarian and cooperative attitudes overall.
Also, as discussed above, the pandemic has the potential for significant economic leveling. Historically, not all leveling moments featured increased cooperation: when initiated by state collapse or transformative revolution, leveling has been accompanied by widespread suffering and bloody conflict. However, during the great leveling moments of the twentieth century—the Depression and the two World Wars—Americans managed to pull together with a sense of shared sacrifice.
Over the longer term, we are still faced with the challenges of climate change, resource depletion, overpopulation, pollution, and biodiversity loss. While the pandemic might have minor or temporary spinoff effects that ameliorate these problems, it won’t solve them. Significant, sustained collective effort will still be required to transform energy systems, economies, and lifestyles (though the pandemic could transform economies and lifestyles in unpredictable ways). If the coronavirus response puts us on a cooperative footing, all the better. Of course, that would be at the expense of currently unknown ultimate numbers of fatalities and sicknesses, as well as widespread fear and privation. The potential bits of silver I’ve mentioned are the linings of a cloud; but, as Monty Python can still remind us via YouTube, it’s always good to look on the bright side of life.
Por Richard Heinberg, publicado originalmente por Resilience.org. Traduzido por Renzo Taddei.
25 de março de 2020
No ano de 2019, o panorama geral para a humanidade era aproximadamente o seguinte. O Homo sapiens (nós), um mamífero bípede de cérebro grande, passou a época do Pleistoceno (de 2,5 milhões de anos atrás até 12.000 anos atrás) desenvolvendo sua habilidade de controlar o fogo, conversar, pintar imagens, tocar flautas ósseas e fazer ferramentas e roupas. A linguagem aumentou drasticamente nossa sociabilidade e nos ajudou a invadir e habitar todos os continentes, exceto a Antártica. Durante a época do Holoceno (os últimos 12.000 anos), começamos a viver em assentamentos permanentes, desenvolvemos a agricultura e construímos sociedades estatais com reis, escravidão, desigualdade econômica, divisão de trabalho em tempo integral, dinheiro, religiões e exércitos. A época do Antropoceno (um breve interlúdio, na verdade) surgiu há apenas alguns séculos, quando nós humanos começamos a usar combustíveis fósseis, o que nos capacitou dramaticamente a aumentar nossa população e nossas taxas de consumo per capita, mecanizar a produção e o transporte e basicamente dominar o planeta inteiro. A mecanização da agricultura, ao tornar redundante o campesinato, levou à urbanização em massa e rapidamente aumentou o tamanho da classe média. No entanto, o uso de combustíveis fósseis desestabilizou o clima global, além de aumentar enormemente os problemas existentes, como poluição, esgotamento de recursos e destruição de habitat para a maioria das criaturas selvagens. Além disso, nas últimas décadas, aprendemos a usar a dívida para transferir o consumo do futuro para o presente, com base no pressuposto arriscado de que a economia continuará a crescer para sempre, possibilitando às gerações futuras pagar pelo estilo de vida que desfrutamos agora.
Em suma, o quadro geral era de poder e perigo crescentes. De repente, o quadro mudou. Um padrão de crescimento econômico furioso, consistente ao longo de muitas décadas desde o início do Antropoceno (com interrupções ocasionais, consistindo principalmente na Grande Depressão e nas duas Guerras Mundiais), chocou-se com força contra a parede do (des)preparo pandêmico. Em um esforço para limitar a mortalidade pelo novo coronavírus, os governos de todo o mundo colocaram suas economias em um estado de hibernação, dizendo à maioria dos trabalhadores para ficar em casa e evitar o contato direto com os outros.
Como esse desenvolvimento está impactando as tendências que já estavam em andamento? As gerações futuras olharão para trás e verão a pandemia de coronavírus como algo que simplesmente passou, ou como um fenômeno que mudou o curso da história? Revisemos algumas das principais tendências que se desenvolveram durante o Antropoceno e exercitemos nossa capacidade de especulação bem informada sobre como elas podem ser afetadas pelo surto de COVID-19.
Mudança climática: Na China, o lockdown de trabalhadores e o fechamento de empresas levaram a uma redução drástica nas emissões de gases de efeito estufa. Nas próximas semanas, as emissões do mundo como um todo podem cair dez por cento ou mais. Nota para os guerreiros do clima: não comemorem de forma muito efusiva; ambientalista exultantes não serão bem vistos pelas pessoas que estão desempregadas por causa da pandemia.
A resposta do mundo ao coronavírus mina o argumento de que os governos não podem reduzir as emissões de carbono porque isso prejudicaria suas economias. Claramente, os líderes nacionais sentiram que a ameaça mais imediata (embora, no esquema mais amplo, menos significativa) da pandemia justificava o fechamento do comércio. Os ativistas climáticos sentem-se encorajados a defender o seguinte argumento: se o decrescimento econômico é o que é necessário para preservar uma biosfera habitável, os líderes mundiais podem e devem encontrar maneiras justas e humanas de reduzir o uso de energia, extração de recursos naturais, atividade industrial e lançamento de resíduos – todos eles elementos que contribuem para as mudanças climáticas.
No entanto, a pandemia não é uma boa notícia para a transição para as energias renováveis. As cadeias de suprimentos para empresas de energia solar e eólica foram interrompidas e a demanda por novas instalações foi reduzida. E com a perspectiva de petróleo e o gás superbaratos (veja “Esgotamento de recursos”, abaixo), é provável que as forças do mercado atrapalhem, em vez de ajudar tanto a indústria de energias renováveis quanto a transição para carros elétricos.
Desigualdade econômica: para os freelancers e para as pessoas que vivem de salário em salário (o que representa 74% dos americanos que são horistas), o bloqueio do coronavírus é uma catástrofe. A curto prazo, as desigualdades econômicas existentes resultarão em níveis altamente desiguais de sacrifício e sofrimento. Pode ser relativamente fácil para trabalhadores com baixos salários racional recursos e aguentar uma ou duas semanas em casa como férias forçadas, mas se dezenas de milhões de americanos sem poupança ficarem vários meses sem renda, as tensões sociais regionais podem chegar ao ponto de ruptura. Essa é uma das razões pelas quais os funcionários do governo estão falando sobre distribuição de dinheiro.
No longo prazo, os recentes níveis absurdos de desigualdade podem ser seriamente rediuzidos. Em seu livro The Great Leveler, o historiador Walter Scheidel argumenta que, no passado, a desigualdade econômica foi revertida de forma dramática pelo que ele chama de “Os Quatro Cavaleiros” – mobilização em massa para guerra, revolução, colapso estatal e epidemias. Atualmente, muitos governos estão realizando esforços de realocação econômica equivalentes, em escala, aos vistos nas guerras mundiais. Por exemplo, a Dinamarca está pagando, por um período de três meses, 75% dos salários (para salários de até 50 mil dólares por ano) para empresas que, de outra forma, teriam que demitir trabalhadores. Isso não apenas permite que os trabalhadores em quarentena sobrevivam, como também permaneçam na folha de pagamento e não precisem voltar ao mercado de trabalho.
Assim, a atual pandemia pode se qualificar como dois cavaleiros de Scheidel (mobilização em massa e epidemia). A classe dos investidores está testemunhando a destruição de capital em taxa e escala prodigiosas, enquanto os esforços dos governos para manter a civilidade e o bem-estar social podem implicar a criação de uma rede de segurança para os mais pobres. Obviamente, não é assim que os advogados da justiça social imaginaram controlar a desigualdade, mas o resultado pode acabar sendo equivalente a outro New Deal, e possivelmente até a um Green New Deal.
Perda de biodiversidade: A nova pandemia de coronavírus quase certamente começou nos mercados de animais selvagens em Wuhan, China. Como Carl Safina colocou em um artigo recente, “os seres humanos causaram a pandemia colocando os animais do mundo em um liquidificador cruel e bebendo-os como um drink”. Embora tenha havido outras epidemias zoonóticas nos últimos anos, incluindo o HIV, o vírus de Marburg, a SARS e a pandemia de “gripe suína” (H1N1) de 2009, o surto global de coronavírus pode proporcionar um momento de aprendizado, em que as organizações de conservação da vida selvagem podem pedir com êxito uma moratória internacional ao comércio ou venda de qualquer espécie animal não domesticada (os zoológicos sendo uma exceção fortemente regulamentada).
Caso contrário, não espere muita mudança na tendência geral de declínio no número de insetos, répteis, anfíbios e pássaros e mamíferos selvagens com os quais compartilhamos este pequeno planeta.
Superpopulação: Alguns indívíduos cínicos da geração Y chamam o novo coronavírus de “Removedor de Boomers”, devido à sua tendência de atacar os idosos com maior virulência. Como a humanidade recentemente adicionou 80 milhões de novos membros por ano (nascimentos menos mortes), uma exclusão do crescimento líquido de um ano na população é possível no pior dos cenários. No entanto, o potencial para uma moderação de curto prazo de nosso padrão geral de expansão demográfica pode ser pelo menos parcialmente compensado pelos resultados, a partir de nove meses a partir de agora, de centenas de milhões de pessoas em idade reprodutiva em todo o mundo que ficam em casa por semanas com pouco o que fazer. Para nações ricas com níveis decrescentes de fertilidade, uma ameaça muito maior à estabilidade da população humana provavelmente continuará sendo representada pelo acúmulo de substâncias químicas no ambiente que causam desregulação endócrina. Para os países pobres com altas tendências de crescimento populacional, oportunidades iguais de educação para todos, independentemente do sexo, ajudarão substancialmente a reduzir as taxas de crescimento.
Esgotamento de recursos: com a produção industrial em queda, a demanda e, portanto, os preços da maioria das mercadorias estão caindo. A commodity mais economicamente crucial do mundo, o petróleo, viu seu preço cair de US$ 50 por barril para perto de US$ 20 (no momento em que este artigo foi escrito); alguns analistas estão prevendo preços em um dígito. Com a queda do uso de petróleo, a capacidade de armazenamento de excedente de petróleo acabará, e os produtores não terão escolha a não ser abandonar alguns poços. As companhias de petróleo provavelmente serão socorridas, mas não serão lucrativas nas condições atuais. A perspectiva de aumentar as taxas mundiais de extração de petróleo até níveis recentes parece fraca. É provável, então, que o momento tão antecipado do pico da produção mundial de petróleo já tenha ocorrido, com pouco alarde, em novembro de 2018.
Obviamente, a queda nos mercados de petróleo é resultado de um desastre econômico, e não de políticas sólidas de conservação de recursos. Portanto, a adaptação por parte da indústria e da sociedade como um todo será caótica. As implicações internacionais são difíceis de prever: várias nações importantes do Oriente Médio verão suas economias destruídas pelos baixos preços do petróleo, e as grandes potências (especificamente China e Rússia) podem tentar aproveitar o momento buscando realinhar alianças na região.
Poluição: Marshall Burke, da Universidade de Stanford, escreveu recentemente que “as reduções na poluição do ar na China causadas por essa perturbação econômica provavelmente salvaram 20 vezes mais vidas na China do que foram perdidas devido à infecção pelo vírus naquele país”. Taxas reduzidas de atividade fabril e de consumo devem ajudar a reduzir a poluição geral, mas é claro que esse é o efeito colateral da crise, não o resultado de uma política sólida. Portanto, sem intervenções em políticas ambientais, não há razão para esperar que os benefícios da redução da poluição sejam sustentados. Apenas um exemplo de como alguns benefícios temporários podem ser equilibrados por novos danos: o uso de plásticos descartáveis provavelmente aumentará durante a resposta à pandemia.
Dívida global explosiva: a economia mundial está novamente em um momento deflacionário, como em 1932 e 2008. Para os bancos centrais e governos, todos os esforços fiscais serão voltados para reinflacionar uma economia que está murchando. Há um risco de que os investidores percebam que, em um mundo sem crescimento, seus instrumentos financeiros são inerentemente inúteis, forçando não apenas um colapso do valor de mercado das ações, mas um repúdio às próprias regras do jogo. No entanto, como a epidemia de coronavírus acabará por retroceder, o resultado mais provável é um período de inadimplência e falências, mitigadas por níveis heróicos de compras de títulos do Fed e ajudas dos governos (para as indústrias de petróleo e companhias aéreas, por exemplo) e déficit de gastos. Eventualmente, se a impressão de moeda crescer de forma exponencial, a hiperinflação é uma possibilidade, mas não tão cedo. Ponto central: o sistema financeiro foi desestabilizado e, como a indústria do petróleo, pode nunca voltar ao “normal”.
* * *
Voltemos à questão colocada acima: a humanidade voltará a olhar para a pandemia de coronavírus como um evento sem maior importância ou como uma transformação profunda? A resposta provável depende, em parte, de quanto tempo dura a pandemia, e isso, por sua vez, dependerá em grande parte da rapidez com que os testes se tornarem amplamente disponíveis e tratamentos e vacinas forem encontrados. Os documentos do governo dos EUA marcados como “impróprios para divulgação pública” sugerem escassez significativa não apenas de equipamentos médicos, mas também de bens em geral nos próximos 18 meses para governo, indústria e cidadãos, se as soluções não forem rapidamente encontradas.
O nível de mudança sistêmica também depende do grau de desaceleração do emprego e do PIB. Fred Bullard, presidente do Fed de St. Louis, afirmou que a taxa de desemprego nos EUA pode atingir 30% no segundo trimestre, devido a paralisações para combater o coronavírus, e que o PIB pode cair 50%. Isso seria uma carnificina econômica muito além da escala da Grande Depressão (a taxa de desemprego nos Estados Unidos em 1933 era de 25%; seu PIB caiu cerca de 15%). Se a economia global cair tanto e permanecer paralisada mesmo por algumas semanas, o coronavírus poderá ser chamado de “o grande divisor de águas”.
Mas uma mudança em que direção? As possibilidades distópicas vêm à mente com muita facilidade. No entanto, em conversas, alguns dos meus colegas que trabalham em think tanks sugeriram que a pandemia poderia se transformar em uma crise de tamanho suficiente para desorganizar a ordem global na medida certa e de tal maneira que promovesse respostas que induzissem pelo menos algumas sociedades à trajetória de cooperação, redistribuição e decrescimento.
Primeiro, os governos costumam lidar com a escassez (prevista nos documentos oficiais citado acima) por meio da estratégia testada e comprovada do racionamento de recursos. Como Stan Cox detalha em seu livro indispensável Any Way You Slice It: The Past, Present, and Future of Rationing, o racionamento nem sempre funciona bem; mas quando isso acontece, os resultados podem ser admiráveis. Durante as duas guerras mundiais, os americanos participaram entusiasticamente de programas de racionamento de alimentos, pneus, roupas e muito mais. A Grã-Bretanha continuou seus programas de racionamento bem após o final da Segunda Guerra Mundial, e pesquisas mostraram que, durante o período de racionamento, os britânicos eram geralmente mais bem alimentados e saudáveis do que antes ou depois. Na maioria dos cenários imaginários de degradação econômica deliberada, os programas de racionamento de energia e bens são os mais prováveis.
Cox conclui que os programas de racionamento tendem a ser mais bem-sucedidos quando as pessoas estão unidas contra um inimigo comum e quando se acredita que a escassez seja temporária. Apesar dos esforços do presidente Trump em chamá-lo de “vírus chinês”, o SARS-Cov-2 não tem nacionalidade inerente, nem é democrata ou republicano. É de fato um inimigo comum, e as pessoas tendem a se tornar mais cooperativas quando confrontadas com uma ameaça coletiva. Além disso, os epidemiologistas concordam que a ameaça terá um ponto final, mesmo que não saibamos exatamente quando será. Portanto, existem condições para o sucesso do racionamento, e ele poderia ajudar a promover atitudes mais comunitárias e cooperativas em geral.
Além disso, como discutido acima, a pandemia tem potencial para a redução significativa das desigualdades econômicas. Historicamente, nem todos os momentos de nivelamento econômico promoveram a cooperação: quando gerados pelo colapso do Estado ou por uma revolução, o nivelamento econômico foi acompanhado por sofrimento generalizado e por conflitos sangrentos. No entanto, durante os grandes momentos de nivelamento do século XX – a Depressão e as duas Guerras Mundiais – os americanos conseguiram se unir ao redor do sentimento de sacrifício compartilhado.
A longo prazo, ainda enfrentamos os desafios das mudanças climáticas, esgotamento de recursos, superpopulação, poluição e perda de biodiversidade. Embora a pandemia possa ter impactos positivos secundários ou menores sobre esses problemas, ela não os resolverá. Esforços coletivos significativos e sustentados ainda serão necessários para transformar sistemas energéticos, economias e estilos de vida (embora a pandemia possa transformar economias e estilos de vida de maneiras imprevisíveis). Se a resposta do coronavírus nos colocar em uma base cooperativa, tanto melhor. Obviamente, isso seria às custas de montantes desconhecidos de mortes, bem como do medo e da privação generalizados. Os elementos positivos que são sólidos como uma nuvem; mas, como Monty Python nos lembra pelo YouTube, é sempre bom olhar para o lado positivo da vida.
Summary of the article: Strong coronavirus measures today should only last a few weeks, there shouldn’t be a big peak of infections afterwards, and it can all be done for a reasonable cost to society, saving millions of lives along the way. If we don’t take these measures, tens of millions will be infected, many will die, along with anybody else that requires intensive care, because the healthcare system will have collapsed.
Within a week, countries around the world have gone from: “This coronavirus thing is not a big deal” to declaring the state of emergency. Yet many countries are still not doing much. Why?
Every country is asking the same question: How should we respond? The answer is not obvious to them.
Some countries, like France, Spain or Philippines, have since ordered heavy lockdowns. Others, like the US, UK, or Switzerland, have dragged their feet, hesitantly venturing into social distancing measures.
Here’s what we’re going to cover today, again with lots of charts, data and models with plenty of sources:
What’s the current situation?
What options do we have?
What’s the one thing that matters now: Time
What does a good coronavirus strategy look like?
How should we think about the economic and social impacts?
When you’re done reading the article, this is what you’ll take away:
Our healthcare system is already collapsing. Countries have two options: either they fight it hard now, or they will suffer a massive epidemic. If they choose the epidemic, hundreds of thousands will die. In some countries, millions. And that might not even eliminate further waves of infections. If we fight hard now, we will curb the deaths. We will relieve our healthcare system. We will prepare better. We will learn. The world has never learned as fast about anything, ever. And we need it, because we know so little about this virus. All of this will achieve something critical: Buy Us Time.
If we choose to fight hard, the fight will be sudden, then gradual. We will be locked in for weeks, not months. Then, we will get more and more freedoms back. It might not be back to normal immediately. But it will be close, and eventually back to normal. And we can do all that while considering the rest of the economy too.
Ok, let’s do this.
1. What’s the situation?
Last week, I showed this curve:
It showed coronavirus cases across the world outside of China. We could only discern Italy, Iran and South Korea. So I had to zoom in on the bottom right corner to see the emerging countries. My entire point is that they would soon be joining these 3 cases.
Let’s see what has happened since.
As predicted, the number of cases has exploded in dozens of countries. Here, I was forced to show only countries with over 1,000 cases. A few things to note:
Spain, Germany, France and the US all have more cases than Italy when it ordered the lockdown
An additional 16 countries have more cases today than Hubei when it went under lockdown: Japan, Malaysia, Canada, Portugal, Australia, Czechia, Brazil and Qatar have more than Hubei but below 1,000 cases. Switzerland, Sweden, Norway, Austria, Belgium, Netherlands and Denmark all have above 1,000 cases.
Do you notice something weird about this list of countries? Outside of China and Iran, which have suffered massive, undeniable outbreaks, and Brazil and Malaysia, every single country in this list is among the wealthiest in the world.
Do you think this virus targets rich countries? Or is it more likely that rich countries are better able to identify the virus?
It’s unlikely that poorer countries aren’t touched. Warm and humid weather probablyhelps, but doesn’t prevent an outbreak by itself — otherwise Singapore, Malaysia or Brazil wouldn’t be suffering outbreaks.
The most likely interpretations are that the coronavirus either took longer to reach these countries because they’re less connected, or it’s already there but these countries haven’t been able to invest enough on testing to know.
Either way, if this is true, it means that most countries won’t escape the coronavirus. It’s a matter of time before they see outbreaks and need to take measures.
What measures can different countries take?
2. What Are Our Options?
Since the article last week, the conversation has changed and many countries have taken measures. Here are some of the most illustrative examples:
Measures in Spain and France
In one extreme, we have Spain and France. This is the timeline of measures for Spain:
On Thursday, 3/12, the President dismissed suggestions that the Spanish authorities had been underestimating the health threat. On Friday, they declared the State of Emergency. On Saturday, measures were taken:
People can’t leave home except for key reasons: groceries, work, pharmacy, hospital, bank or insurance company (extreme justification)
Specific ban on taking kids out for a walk or seeing friends or family (except to take care of people who need help, but with hygiene and physical distance measures)
All bars and restaurants closed. Only take-home acceptable.
All entertainment closed: sports, movies, museums, municipal celebrations…
Weddings can’t have guests. Funerals can’t have more than a handful of people.
Mass transit remains open
On Monday, land borders were shut.
Some people see this as a great list of measures. Others put their hands up in the air and cry of despair. This difference is what this article will try to reconcile.
France’s timeline of measures is similar, except they took more time to apply them, and they are more aggressive now. For example, rent, taxes and utilities are suspended for small businesses.
Measures in the US and UK
The US and UK, like countries such as Switzerland, have dragged their feet in implementing measures. Here’s the timeline for the US:
Wednesday 3/11: travel ban.
Friday: National Emergency declared. No social distancing measures
Monday: the government urges the public to avoid restaurants or bars and attend events with more than 10 people. No social distancing measure is actually enforceable. It’s just a suggestion.
Lots of states and cities are taking the initiative and mandating much stricter measures.
The UK has seen a similar set of measures: lots of recommendations, but very few mandates.
These two groups of countries illustrate the two extreme approaches to fight the coronavirus: mitigation and suppression. Let’s understand what they mean.
Option 1: Do Nothing
Before we do that, let’s see what doing nothing would entail for a country like the US:
This fantastic epidemic calculator can help you understand what will happen under different scenarios. I’ve pasted below the graph the key factors that determine the behavior of the virus. Note that infected, in pink, peak in the tens of millions at a certain date. Most variables have been kept from the default. The only material changes are R from 2.2 to 2.4 (corresponds better to currently available information. See at the bottom of the epidemic calculator), fatality rate (4% due to healthcare system collapse. See details below or in the previous article), length of hospital stay (down from 20 to 10 days) and hospitalization rate (down from 20% to 14% based on severe and critical cases. Note the WHO calls out a 20% rate) based on our most recently available gathering of research. Note that these numbers don’t change results much. The only change that matters is the fatality rate.
If we do nothing: Everybody gets infected, the healthcare system gets overwhelmed, the mortality explodes, and ~10 million people die (blue bars). For the back-of-the-envelope numbers: if ~75% of Americans get infected and 4% die, that’s 10 million deaths, or around 25 times the number of US deaths in World War II.
You might wonder: “That sounds like a lot. I’ve heard much less than that!”
So what’s the catch? With all these numbers, it’s easy to get confused. But there’s only two numbers that matter: What share of people will catch the virus and fall sick, and what share of them will die. If only 25% are sick (because the others have the virus but don’t have symptoms so aren’t counted as cases), and the fatality rate is 0.6% instead of 4%, you end up with 500k deaths in the US.
If we don’t do anything, the number of deaths from the coronavirus will probably land between these two numbers. The chasm between these extremes is mostly driven by the fatality rate, so understanding it better is crucial. What really causes the coronavirus deaths?
How Should We Think about the Fatality Rate?
This is the same graph as before, but now looking at hospitalized people instead of infected and dead:
The light blue area is the number of people who would need to go to the hospital, and the darker blue represents those who need to go to the intensive care unit (ICU). You can see that number would peak at above 3 million.
Now compare that to the number of ICU beds we have in the US (50k today, we could double that repurposing other space). That’s the red dotted line.
No, that’s not an error.
That red dotted line is the capacity we have of ICU beds. Everyone above that line would be in critical condition but wouldn’t be able to access the care they need, and would likely die.
This is why people died in droves in Hubei and are now dying in droves in Italy and Iran. The Hubei fatality rate ended up better than it could have been because they built 2 hospitals nearly overnight. Italy and Iran can’t do the same; few, if any, other countries can. We’ll see what ends up happening there.
So why is the fatality rate close to 4%?
If 5% of your cases require intensive care and you can’t provide it, most of those people die. As simple as that.
These numbers only show people dying from coronavirus. But what happens if all your healthcare system is collapsed by coronavirus patients? Others also die from other ailments.
What happens if you have a heart attack but the ambulance takes 50 minutes to come instead of 8 (too many coronavirus cases) and once you arrive, there’s no ICU and no doctor available? You die.
There are 4 million admissions to the ICU in the US every year, and 500k (~13%) of them die. Without ICU beds, that share would likely go much closer to 80%. Even if only 50% died, in a year-long epidemic you go from 500k deaths a year to 2M, so you’re adding 1.5M deaths, just with collateral damage.
If the coronavirus is left to spread, the US healthcare system will collapse, and the deaths will be in the millions, maybe more than 10 million.
The same thinking is true for most countries. The number of ICU beds and ventilators and healthcare workers are usually similar to the US or lower in most countries. Unbridled coronavirus means healthcare system collapse, and that means mass death.
Unbridled coronavirus means healthcare systems collapse, and that means mass death.
By now, I hope it’s pretty clear we should act. The two options that we have are mitigation and suppression. Both of them propose to “flatten the curve”, but they go about it very differently.
Option 2: Mitigation Strategy
Mitigation goes like this: “It’s impossible to prevent the coronavirus now, so let’s just have it run its course, while trying to reduce the peak of infections. Let’s just flatten the curve a little bit to make it more manageable for the healthcare system.”
This chart appears in a very important paper published over the weekend from the Imperial College London. Apparently, it pushed the UK and US governments to change course.
It’s a very similar graph as the previous one. Not the same, but conceptually equivalent. Here, the “Do Nothing” situation is the black curve. Each one of the other curves are what would happen if we implemented tougher and tougher social distancing measures. The blue one shows the toughest social distancing measures: isolating infected people, quarantining people who might be infected, and secluding old people. This blue line is broadly the current UK coronavirus strategy, although for now they’re just suggesting it, not mandating it.
Here, again, the red line is the capacity for ICUs, this time in the UK. Again, that line is very close to the bottom. All that area of the curve on top of that red line represents coronavirus patients who would mostly die because of the lack of ICU resources.
Not only that, but by flattening the curve, the ICUs will collapse for months, increasing collateral damage.
You should be shocked. When you hear: “We’re going to do some mitigation” what they’re really saying is: “We will knowingly overwhelm the healthcare system, driving the fatality rate up by a factor of 10x at least.”
You would imagine this is bad enough. But we’re not done yet. Because one of the key assumptions of this strategy is what’s called “Herd Immunity”.
Herd Immunity and Virus Mutation
The idea is that all the people who are infected and then recover are now immune to the virus. This is at the core of this strategy: “Look, I know it’s going to be hard for some time, but once we’re done and a few million people die, the rest of us will be immune to it, so this virus will stop spreading and we’ll say goodbye to the coronavirus. Better do it at once and be done with it, because our alternative is to do social distancing for up to a year and risk having this peak happen later anyways.”
Except this assumes one thing: the virus doesn’t change too much. If it doesn’t change much, then lots of people do get immunity, and at some point the epidemic dies down
How likely is this virus to mutate? It seems it already has.
This graph represents the different mutations of the virus. You can see that the initial strains started in purple in China and then spread. Each time you see a branching on the left graph, that is a mutation leading to a slightly different variant of the virus.
This should not be surprising: RNA-based viruses like the coronavirus or the flu tend to mutate around 100 times faster than DNA-based ones—although the coronavirus mutates more slowly than influenza viruses.
Not only that, but the best way for this virus to mutate is to have millions of opportunities to do so, which is exactly what a mitigation strategy would provide: hundreds of millions of people infected.
That’s why you have to get a flu shot every year. Because there are so many flu strains, with new ones always evolving, the flu shot can never protect against all strains.
Put in another way: the mitigation strategy not only assumes millions of deaths for a country like the US or the UK. It also gambles on the fact that the virus won’t mutate too much — which we know it does. And it will give it the opportunity to mutate. So once we’re done with a few million deaths, we could be ready for a few million more — every year. This corona virus could become a recurring fact of life, like the flu, but many times deadlier.
The best way for this virus to mutate is to have millions of opportunities to do so, which is exactly what a mitigation strategy would provide.
So if neither doing nothing and mitigation will work, what’s the alternative? It’s called suppression.
Option 3: Suppression Strategy
The Mitigation Strategy doesn’t try to contain the epidemic, just flatten the curve a bit. Meanwhile, the Suppression Strategy tries to apply heavy measures to quickly get the epidemic under control. Specifically:
Go hard right now. Order heavy social distancing. Get this thing under control.
Then, release the measures, so that people can gradually get back their freedoms and something approaching normal social and economic life can resume.
What does that look like?
All the model parameters are the same, except that there is an intervention around now to reduce the transmission rate to R=0.62, and because the healthcare system isn’t collapsed, the fatality rate goes down to 0.6%. I defined “around now” as having ~32,000 cases when implementing the measures (3x the official number as of today, 3/19). Note that this is not too sensitive to the R chosen. An R of 0.98 for example shows 15,000 deaths. Five times more than with an R of 0.62, but still tens of thousands of deaths and not millions. It’s also not too sensitive to the fatality rate: if it’s 0.7% instead of 0.6%, the death toll goes from 15,000 to 17,000. It’s the combination of a higher R, a higher fatality rate, and a delay in taking measures that explodes the number of fatalities. That’s why we need to take measures to reduce R today. For clarification, the famous R0 is R at the beginning (R at time 0). It’s the transmission rate when nobody is immune yet and there are no measures against it taken. R is the overall transmission rate.
Under a suppression strategy, after the first wave is done, the death toll is in the thousands, and not in the millions.
Why? Because not only do we cut the exponential growth of cases. We also cut the fatality rate since the healthcare system is not completely overwhelmed. Here, I used a fatality rate of 0.9%, around what we’re seeing in South Korea today, which has been most effective at following Suppression Strategy.
Said like this, it sounds like a no-brainer. Everybody should follow the Suppression Strategy.
So why do some governments hesitate?
They fear three things:
This first lockdown will last for months, which seems unacceptable for many people.
A months-long lockdown would destroy the economy.
It wouldn’t even solve the problem, because we would be just postponing the epidemic: later on, once we release the social distancing measures, people will still get infected in the millions and die.
Here is how the Imperial College team modeled suppressions. The green and yellow lines are different scenarios of Suppression. You can see that doesn’t look good: We still get huge peaks, so why bother?
We’ll get to these questions in a moment, but there’s something more important before.
This is completely missing the point.
Presented like these, the two options of Mitigation and Suppression, side by side, don’t look very appealing. Either a lot of people die soon and we don’t hurt the economy today, or we hurt the economy today, just to postpone the deaths.
This ignores the value of time.
3. The Value of Time
In our previous post, we explained the value of time in saving lives. Every day, every hour we waited to take measures, this exponential threat continued spreading. We saw how a single day could reduce the total cases by 40% and the death toll by even more.
But time is even more valuable than that.
We’re about to face the biggest wave of pressure on the healthcare system ever seen in history. We are completely unprepared, facing an enemy we don’t know. That is not a good position for war.
What if you were about to face your worst enemy, of which you knew very little, and you had two options: Either you run towards it, or you escape to buy yourself a bit of time to prepare. Which one would you choose?
This is what we need to do today. The world has awakened. Every single day we delay the coronavirus, we can get better prepared. The next sections detail what that time would buy us:
Lower the Number of Cases
With effective suppression, the number of true cases would plummet overnight, as we saw in Hubei last week.
As of today, there are 0 daily new cases of coronavirus in the entire 60 million-big region of Hubei.
The diagnostics would keep going up for a couple of weeks, but then they would start going down. With fewer cases, the fatality rate starts dropping too. And the collateral damage is also reduced: fewer people would die from non-coronavirus-related causes because the healthcare system is simply overwhelmed.
Suppression would get us:
Fewer total cases of Coronavirus
Immediate relief for the healthcare system and the humans who run it
Reduction in fatality rate
Reduction in collateral damage
Ability for infected, isolated and quarantined healthcare workers to get better and back to work. In Italy, healthcare workers represent 8% of all contagions.
Understand the True Problem: Testing and Tracing
Right now, the UK and the US have no idea about their true cases. We don’t know how many there are. We just know the official number is not right, and the true one is in the tens of thousands of cases. This has happened because we’re not testing, and we’re not tracing.
With a few more weeks, we could get our testing situation in order, and start testing everybody. With that information, we would finally know the true extent of the problem, where we need to be more aggressive, and what communities are safe to be released from a lockdown.
We could also set up a tracing operation like the ones they have in China or other East Asia countries, where they can identify all the people that every sick person met, and can put them in quarantine. This would give us a ton of intelligence to release later on our social distancing measures: if we know where the virus is, we can target these places only. This is not rocket science: it’s the basics of how East Asia Countries have been able to control this outbreak without the kind of draconian social distancing that is increasingly essential in other countries.
The measures from this section (testing and tracing) single-handedly curbed the growth of the coronavirus in South Korea and got the epidemic under control, without a strong imposition of social distancing measures.
Build Up Capacity
The US (and presumably the UK) are about to go to war without armor.
We have masks for just two weeks, few personal protective equipments (“PPE”), not enough ventilators, not enough ICU beds, not enough ECMOs (blood oxygenation machines)… This is why the fatality rate would be so high in a mitigation strategy.
But if we buy ourselves some time, we can turn this around:
We have more time to buy equipment we will need for a future wave
We can quickly build up our production of masks, PPEs, ventilators, ECMOs, and any other critical device to reduce fatality rate.
Put in another way: we don’t need years to get our armor, we need weeks. Let’s do everything we can to get our production humming now. Countries are mobilized. People are being inventive, such as using 3D printing for ventilator parts. We can do it. We just need more time. Would you wait a few weeks to get yourself some armor before facing a mortal enemy?
This is not the only capacity we need. We will need health workers as soon as possible. Where will we get them? We need to train people to assist nurses, and we need to get medical workers out of retirement. Many countries have already started, but this takes time. We can do this in a few weeks, but not if everything collapses.
Lower Public Contagiousness
The public is scared. The coronavirus is new. There’s so much we don’t know how to do yet! People haven’t learned to stop hand-shaking. They still hug. They don’t open doors with their elbow. They don’t wash their hands after touching a door knob. They don’t disinfect tables before sitting.
Once we have enough masks, we can use them outside of the healthcare system too. Right now, it’s better to keep them for healthcare workers. But if they weren’t scarce, people should wear them in their daily lives, making it less likely that they infect other people when sick, and with proper training also reducing the likelihood that the wearers get infected. (In the meantime, wearing something is better than nothing.)
All of these are pretty cheap ways to reduce the transmission rate. The less this virus propagates, the fewer measures we’ll need in the future to contain it. But we need time to educate people on all these measures and equip them.
Understand the Virus
We know very very little about the virus. But every week, hundreds of new papers are coming.
The world is finally united against a common enemy. Researchers around the globe are mobilizing to understand this virus better.
How does the virus spread? How can contagion be slowed down? What is the share of asymptomatic carriers? Are they contagious? How much? What are good treatments? How long does it survive? On what surfaces? How do different social distancing measures impact the transmission rate? What’s their cost? What are tracing best practices? How reliable are our tests?
Clear answers to these questions will help make our response as targeted as possible while minimizing collateral economic and social damage. And they will come in weeks, not years.
Find Treatments
Not only that, but what if we found a treatment in the next few weeks? Any day we buy gets us closer to that. Right now, there are already several candidates, such as Favipiravir, Chloroquine, or Chloroquine combined with Azithromycin. What if it turned out that in two months we discovered a treatment for the coronavirus? How stupid would we look if we already had millions of deaths following a mitigation strategy?
Understand the Cost-Benefits
All of the factors above can help us save millions of lives. That should be enough. Unfortunately, politicians can’t only think about the lives of the infected. They must think about all the population, and heavy social distancing measures have an impact on others.
Right now we have no idea how different social distancing measures reduce transmission. We also have no clue what their economic and social costs are.
Isn’t it a bit difficult to decide what measures we need for the long term if we don’t know their cost or benefit?
A few weeks would give us enough time to start studying them, understand them, prioritize them, and decide which ones to follow.
Fewer cases, more understanding of the problem, building up assets, understanding the virus, understanding the cost-benefit of different measures, educating the public… These are some core tools to fight the virus, and we just need a few weeks to develop many of them. Wouldn’t it be dumb to commit to a strategy that throws us instead, unprepared, into the jaws of our enemy?
4. The Hammer and the Dance
Now we know that the Mitigation Strategy is probably a terrible choice, and that the Suppression Strategy has a massive short-term advantage.
But people have rightful concerns about this strategy:
How long will it actually last?
How expensive will it be?
Will there be a second peak as big as if we didn’t do anything?
Here, we’re going to look at what a true Suppression Strategy would look like. We can call it the Hammer and the Dance.
The Hammer
First, you act quickly and aggressively. For all the reasons we mentioned above, given the value of time, we want to quench this thing as soon as possible.
One of the most important questions is: How long will this last?
The fear that everybody has is that we will be locked inside our homes for months at a time, with the ensuing economic disaster and mental breakdowns. This idea was unfortunately entertained in the famous Imperial College paper:
Do you remember this chart? The light blue area that goes from end of March to end of August is the period that the paper recommends as the Hammer, the initial suppression that includes heavy social distancing.
If you’re a politician and you see that one option is to let hundreds of thousands or millions of people die with a mitigation strategy and the other is to stop the economy for five months before going through the same peak of cases and deaths, these don’t sound like compelling options.
But this doesn’t need to be so. This paper, driving policy today, has been brutally criticized for core flaws: They ignore contact tracing (at the core of policies in South Korea, China or Singapore among others) or travel restrictions (critical in China), ignore the impact of big crowds…
The time needed for the Hammer is weeks, not months.
This graph shows the new cases in the entire Hubei region (60 million people) every day since 1/23. Within 2 weeks, the country was starting to get back to work. Within ~5 weeks it was completely under control. And within 7 weeks the new diagnostics was just a trickle. Let’s remember this was the worst region in China.
Remember again that these are the orange bars. The grey bars, the true cases, had plummeted much earlier (see Chart 9).
The measures they took were pretty similar to the ones taken in Italy, Spain or France: isolations, quarantines, people had to stay at home unless there was an emergency or had to buy food, contact tracing, testing, more hospital beds, travel bans…
Details matter, however.
China’s measures were stronger. For example, people were limited to one person per household allowed to leave home every three days to buy food. Also, their enforcement was severe. It is likely that this severity stopped the epidemic faster.
In Italy, France and Spain, measures were not as drastic, and their implementation is not as tough. People still walk on the streets, many without masks. This is likely to result in a slower Hammer: more time to fully control the epidemic.
Some people interpret this as “Democracies will never be able to replicate this reduction in cases”. That’s wrong.
For several weeks, South Korea had the worst epidemic outside of China. Now, it’s largely under control. And they did it without asking people to stay home. They achieved it mostly with very aggressive testing, contact tracing, and enforced quarantines and isolations.
The following table gives a good sense of what measures different countries have followed, and how that has impacted them (this is a work-in-progress. Feedback welcome.)
This shows how countries who were prepared, with stronger epidemiological authority, education on hygiene and social distancing, and early detection and isolation, didn’t have to pay with heavier measures afterwards.
Conversely, countries like Italy, Spain or France weren’t doing these well, and had to then apply the Hammer with the hard measures at the bottom to catch up.
The lack of measures in the US and UK is in stark contrast, especially in the US. These countries are still not doing what allowed Singapore, South Korea or Taiwan to control the virus, despite their outbreaks growing exponentially. But it’s a matter of time. Either they have a massive epidemic, or they realize late their mistake, and have to overcompensate with a heavier Hammer. There is no escape from this.
But it’s doable. If an outbreak like South Korea’s can be controlled in weeks and without mandated social distancing, Western countries, which are already applying a heavy Hammer with strict social distancing measures, can definitely control the outbreak within weeks. It’s a matter of discipline, execution, and how much the population abides by the rules.
Once the Hammer is in place and the outbreak is controlled, the second phase begins: the Dance.
The Dance
If you hammer the coronavirus, within a few weeks you’ve controlled it and you’re in much better shape to address it. Now comes the longer-term effort to keep this virus contained until there’s a vaccine.
This is probably the single biggest, most important mistake people make when thinking about this stage: they think it will keep them home for months. This is not the case at all. In fact, it is likely that our lives will go back to close to normal.
In this video, the South Korea Foreign Minister explains how her country did it. It was pretty simple: efficient testing, efficient tracing, travel bans, efficient isolating and efficient quarantining.
Want to guess their measures? The same ones as in South Korea. In their case, they complemented with economic help to those in quarantine and travel bans and delays.
Is it too late for these countries and others? No. By applying the Hammer, they’re getting a new chance, a new shot at doing this right. The more they wait, the heavier and longer the hammer, but it can control the epidemics.
But what if all these measures aren’t enough?
The Dance of R
I call the months-long period between the Hammer and a vaccine or effective treatment the Dance because it won’t be a period during which measures are always the same harsh ones. Some regions will see outbreaks again, others won’t for long periods of time. Depending on how cases evolve, we will need to tighten up social distancing measures or we will be able to release them. That is the dance of R: a dance of measures between getting our lives back on track and spreading the disease, one of economy vs. healthcare.
How does this dance work?
It all turns around the R. If you remember, it’s the transmission rate. Early on in a standard, unprepared country, it’s somewhere between 2 and 3: During the few weeks that somebody is infected, they infect between 2 and 3 other people on average.
If R is above 1, infections grow exponentially into an epidemic. If it’s below 1, they die down.
During the Hammer, the goal is to get R as close to zero, as fast as possible, to quench the epidemic. In Wuhan, it is calculated that R was initially 3.9, and after the lockdown and centralized quarantine, it went down to 0.32.
But once you move into the Dance, you don’t need to do that anymore. You just need your R to stay below 1: a lot of the social distancing measures have true, hard costs on people. They might lose their job, their business, their healthy habits…
You can remain below R=1 with a few simple measures.
This is an approximation of how different types of patients respond to the virus, as well as their contagiousness. Nobody knows the true shape of this curve, but we’ve gathered data from different papers to approximate how it looks like.
Every day after they contract the virus, people have some contagion potential. Together, all these days of contagion add up to 2.5 contagions on average.
It is believed that there are some contagions already happening during the “no symptoms” phase. After that, as symptoms grow, usually people go to the doctor, get diagnosed, and their contagiousness diminishes.
For example, early on you have the virus but no symptoms, so you behave as normal. When you speak with people, you spread the virus. When you touch your nose and then open door knob, the next people to open the door and touch their nose get infected.
The more the virus is growing inside you, the more infectious you are. Then, once you start having symptoms, you might slowly stop going to work, stay in bed, wear a mask, or start going to the doctor. The bigger the symptoms, the more you distance yourself socially, reducing the spread of the virus.
Once you’re hospitalized, even if you are very contagious you don’t tend to spread the virus as much since you’re isolated.
This is where you can see the massive impact of policies like those of Singapore or South Korea:
If people are massively tested, they can be identified even before they have symptoms. Quarantined, they can’t spread anything.
If people are trained to identify their symptoms earlier, they reduce the number of days in blue, and hence their overall contagiousness
If people are isolated as soon as they have symptoms, the contagions from the orange phase disappear.
If people are educated about personal distance, mask-wearing, washing hands or disinfecting spaces, they spread less virus throughout the entire period.
Only when all these fail do we need heavier social distancing measures.
The ROI of Social Distancing
If with all these measures we’re still way above R=1, we need to reduce the average number of people that each person meets.
There are some very cheap ways to do that, like banning events with more than a certain number of people (eg, 50, 500), or asking people to work from home when they can.
Other are much, much more expensive economically, socially and ethically, such as closing schools and universities, asking everybody to stay home, or closing businesses.
This chart is made up because it doesn’t exist today. Nobody has done enough research about this or put together all these measures in a way that can compare them.
It’s unfortunate, because it’s the single most important chart that politicians would need to make decisions. It illustrates what is really going through their minds.
During the Hammer period, politicians want to lower R as much as possible, through measures that remain tolerable for the population. In Hubei, they went all the way to 0.32. We might not need that: maybe just to 0.5 or 0.6.
But during the Dance of the R period, they want to hover as close to 1 as possible, while staying below it over the long term term. That prevents a new outbreak, while eliminating the most drastic measures.
What this means is that, whether leaders realize it or not, what they’re doing is:
List all the measures they can take to reduce R
Get a sense of the benefit of applying them: the reduction in R
Get a sense of their cost: the economic, social, and ethical cost.
Stack-rank the initiatives based on their cost-benefit
Pick the ones that give the biggest R reduction up till 1, for the lowest cost.
This is for illustrative purposes only. All data is made up. However, as far as we were able to tell, this data doesn’t exist today. It needs to. For example, the list from the CDC is a great start, but it misses things like education measures, triggers, quantifications of costs and benefits, measure details, economic / social countermeasures…
Initially, their confidence on these numbers will be low. But that‘s still how they are thinking—and should be thinking about it.
What they need to do is formalize the process: Understand that this is a numbers game in which we need to learn as fast as possible where we are on R, the impact of every measure on reducing R, and their social and economic costs.
Only then will they be able to make a rational decision on what measures they should take.
Conclusion: Buy Us Time
The coronavirus is still spreading nearly everywhere. 152 countries have cases. We are against the clock. But we don’t need to be: there’s a clear way we can be thinking about this.
Some countries, especially those that haven’t been hit heavily yet by the coronavirus, might be wondering: Is this going to happen to me? The answer is: It probably already has. You just haven’t noticed. When it really hits, your healthcare system will be in even worse shape than in wealthy countries where the healthcare systems are strong. Better safe than sorry, you should consider taking action now.
For the countries where the coronavirus is already here, the options are clear.
On one side, countries can go the mitigation route: create a massive epidemic, overwhelm the healthcare system, drive the death of millions of people, and release new mutations of this virus in the wild.
On the other, countries can fight. They can lock down for a few weeks to buy us time, create an educated action plan, and control this virus until we have a vaccine.
Governments around the world today, including some such as the US, the UK or Switzerland have so far chosen the mitigation path.
That means they’re giving up without a fight. They see other countries having successfully fought this, but they say: “We can’t do that!”
What if Churchill had said the same thing? “Nazis are already everywhere in Europe. We can’t fight them. Let’s just give up.” This is what many governments around the world are doing today. They’re not giving you a chance to fight this. You have to demand it.
Share the Word
Unfortunately, millions of lives are still at stake. Share this article—or any similar one—if you think it can change people’s opinion. Leaders need to understand this to avert a catastrophe. The moment to act is now.
If you are an expert in the field and want to criticize or endorse the article or some of its parts, feel free to leave a private note here or contextually and I will respond or address.
If you want to translate this article, do it on a Medium post and leave me a private note here with your link. Here are the translations currently available:
This article has been the result of a herculean effort by a group of normal citizens working around the clock to find all the relevant research available to structure it into one piece, in case it can help others process all the information that is out there about the coronavirus.
Special thanks to Dr. Carl Juneau (epidemiologist and translator of the French version), Dr. Brandon Fainstad, Pierre Djian, Jorge Peñalva, John Hsu, Genevieve Gee, Elena Baillie, Chris Martinez, Yasemin Denari, Christine Gibson, Matt Bell, Dan Walsh, Jessica Thompson, Karim Ravji, Annie Hazlehurst, and Aishwarya Khanduja. This has been a team effort.
Thank you also to Berin Szoka, Shishir Mehrotra, QVentus, Illumina, Josephine Gavignet, Mike Kidd, and Nils Barth for your advice. Thank you to my company, Course Hero, for giving me the time and freedom to focus on this.
2 MSc in Engineering. Stanford MBA. Ex-Consultant. Creator of viral applications with >20M users. Currently leading a billion-dollar business @ Course Hero
A Itália de onde escrevo, um dos países mais vivazes e alegres do mundo, é hoje apenas um deserto. Cada um dos seus 60 milhões de habitantes acha que é imortal, que o vírus não o tocará, que irá matar não ele mas alguma outra pessoa. Porém, no silêncio do seu coração, cada um sabe que essa ilusão é pueril e que essa pandemia misteriosa, abstrata e tangível ao mesmo tempo, escolhe suas vítimas ao acaso, como numa roleta russa.
Em algum tempo vamos saber se o vírus pode ser debelado ou se nos matará em massa, assim como fez no século passado a famosa gripe espanhola, que matou 1 milhão de pessoas por semana durante 25 semanas seguidas.
Moro há 50 anos no centro de Roma, na rua mais movimentada da cidade, que leva da praça Veneza à Basílica de São Pedro.
Normalmente, essa rua está 24 horas por dia entupida de trânsito, de turistas e peregrinos. Há duas semanas, está muda e deserta. Só de vez em quando ouve-se o grito de uma sirene de ambulância e algum sem-teto passa. A cidade inteira está fantasmagórica como a Los Angeles de “Blade Runner”. Aqui, porém, desapareceram até os replicantes extraterrestres.
Fechados os lugares públicos, as escolas, as fábricas, as lojas, as estações, os portos e os aeroportos, a Itália é agora um país separado do resto da Europa e do mundo. Cada cidade está parada, cada família trancafiada em casa. Quem sai à revelia dos pouquíssimos motivos permitidos é interceptado imediatamente pelas rondas policiais que aplicam penas bastante severas.
Os gregos antigos consideravam que, quando algo é indispensável e todavia impossível, a situação é trágica. Foram necessários 50 dias, milhares de doentes e mortos para que os italianos entendessem que a situação é, enfim, irremediavelmente trágica.
O que significa uma pandemia como essa para Roma, para a Itália, para a humanidade como um todo? Como ela age nas mentes e nos corações de todos nós que, armados com tecnologias poderosas e inteligência artificial, até poucas semanas atrás nos sentíamos os senhores do céu e da terra?
Subitamente nos descobrimos frágeis pigmeus diante da onipotência imaterial de um vírus que, por vias misteriosas, escapou de um morcego chinês para vir matar homens e mulheres em nossas cidades.
A sujeição a um vírus desconhecido, para o qual não há nem cura nem vacina, transformou a Itália numa enorme caserna blindada e os 60 milhões de italianos noutros tantos dóceis soldadinhos empenhados num gigantesco exercício militar no qual estão obrigados a aprender a verdade que antes ignoravam obstinadamente. O que não quer dizer que irão apreendê-la.
Numa Europa onde, até ontem, era permitida a livre circulação de pessoas, mercadorias e dinheiro, agora cada país, em vez de abraçar uma colaboração ainda mais solidária com os demais, tranca suas próprias fronteiras, iludindo-se de forma cínica e infantil que seja possível deter o vírus com barreiras aduaneiras.
Contudo, hoje, mais do que nunca, os soberanismos parecem tentativas fantasiosas contra a globalização. Hoje, mais do que nunca, a difusão da pandemia e sua rápida volta ao mundo demonstraram que deter a globalização é como se opor à força de gravidade. Nosso planeta já é aquela “aldeia global” da qual falava McLuhan, unida por infortúnios e pela vontade de viver, precisando de uma direção unitária, capaz de coordenar a ação sinérgica de todos os povos que desejam se salvar. Nessa aldeia global, nenhum homem, nenhum país é uma ilha.
Talvez tenhamos aprendido que o caso agora é de vida ou morte e que ninguém pode enfrentar sozinho um vírus tão ardiloso e potente. Por isso, são necessários recursos, inteligências, competências, ações e instituições coletivas. Coordenação e coesão geral. É necessária uma cabine de comando, um governo competente que tenha autoridade, uma equipe formada por um vértice político de grande inteligência e apoiada pelos máximos representantes das ciências médicas, da economia, da sociologia, da psicologia social e da comunicação.
Talvez tenhamos aprendido que os fatos e os dados devem prevalecer sobre as opiniões, a competência reconhecida deva prevalecer sobre o simples bom senso, a prudência e a gradualidade das intervenções devem prevalecer às tomadas de decisões arrogantes e à improvisação imprudente. Por outro lado, é necessário tolerar os erros de quem possui a responsabilidade terrível de tomar decisões, líder que deve ser generosamente amparado para que sejam melhoradas.
Talvez tenhamos aprendido que, perante um vírus desconhecido, assim como diante de um problema complexo, as decisões sobre a pandemia não apenas devem ser tomadas pelas pessoas competentes mas também ser comunicadas de forma unívoca, com autoridade, prontamente, de forma abrangente e clara. Todo o alarmismo, todo o exagero, toda a subestimação é terrível porque confunde as ideias e nos faz perder um tempo precioso. Carência e excesso de informações são parâmetros nocivos. Talk shows superficiais e fake news delirantes levam ao cinismo e à desumanização.
Talvez tenhamos aprendido que, nos países civilizados, o bem-estar é uma conquista irrenunciável. Por sorte e pela sabedoria dos nossos pais, a Constituição italiana de 1948 considera a saúde como um direito fundamental de cada ser humano. Já a reforma sanitária de 1978 instituiu um serviço nacional universal que considera a saúde não como meramente a ausência de doença, mas como o bem-estar físico, psíquico e social completo.
Graças a esse regime de saúde, todos os residentes (e também os turistas) fruem dos cuidados médicos sem qualquer custo. Isso nos possibilitou descobrir e curar prontamente os contágios e reduzir o número de mortes.
No país mais rico e mais poderoso do mundo, os EUA, onde o bem-estar é estupidamente mortificado, os suspeitos de Covid-19 precisam desembolsar o equivalente a 1.200 euros pelo teste. O vírus corona, ao se difundir, causaria uma verdadeira hecatombe entre 90 milhões de estadunidenses que, desprovidos de seguro-saúde, seriam cinicamente rejeitados pelos hospitais.
A propaganda neoliberal, que se alastrou sob a bandeira insana de Reagan e Thatcher, desacreditou tudo o que é público em favor do setor privado. Porém, pelo contrário, nessas semanas trágicas, a reação eficiente dos hospitais e dos funcionários públicos diante do surgimento da pandemia nos ensinou que a nossa saúde pública, da mesma forma que outras funções públicas, dispõe, muito mais do que o setor privado, de pessoas preparadas profissionalmente, motivadas e generosas até o heroísmo.
Toda noite, às 18h, todas as janelas da Itália se escancaram e cada um canta ou toca o hino nacional para agradecer aos médicos e a todos os profissionais da saúde.
A pandemia está nos ensinando que o pensamento de Keynes permanece precioso. Em 1980, o prêmio Nobel Robert Lucas Jr. observou: “Não é possível encontrar nenhum bom economista com menos de 40 anos que se diga ‘keynesiano’. Nas universidades, as teorias keynesianas não são levadas a sério e provocam sorrisinhos de superioridade”.
Hoje, essa crise histórica, com seus mortos e com suas tragédias, se porum lado nos leva à recessão, por outro nos lembra que, para evitar uma crise irreparável, em vez de políticas de austeridade, é preferível dar lugar aos investimentos públicos maciços e “open-ended”, ainda que isso leve ao déficit público.
Talvez tenhamos aprendido tudo isso e várias outras coisas com aquilo que ocorreu fora do recinto doméstico, isto é, entre o governo e todo o povo do país. Entretanto, hoje, a nossa vida está segregada entre as paredes domésticas. Todos estão restritos entre as quatro paredes da própria casa: não só as famílias que vivem em harmonia e acordo, mas também os solitários, os casais em crise e os núcleos familiares em que o diálogo entre pais e filhos há muito tempo andava claudicante.
A sociedade industrial nos habituara a separar o local de trabalho do local de vida, nos fazendo passar a maior parte do nosso tempo com chefes e colegas nas empresas: os que a sociologia chama de grupos “secundários”, frios, formais, nos quais as relações são quase exclusivamente profissionais. Uma parte mínima do nosso tempo nos via reunidos em família ou com os amigos, ou seja, com grupos “primários”, calorosos, informais, envolventes.
De repente, o descanso compulsório em casa nos obrigou de forma inédita ao isolamento total, a uma convivência forçada que para alguns parece agradável e tranquilizadora, mas que para outros é invasiva e até opressora. Os mais sortudos conseguem transformar o ócio depressivo em ócio criativo, conjugando a leitura, o estudo, o lúdico com a parcela de trabalho que é possível desempenhar em regime de “smart working”.
Sabíamos teoricamente que essa modalidade de trabalho à distância permite aos trabalhadores uma preciosa economia de tempo, dinheiro, stress e alienação; e às empresas, evita os microconflitos, despesas na manutenção do local de trabalho e promove incremento da eficiência, recuperando de 15 a 20% da produtividade; à coletividade, evita a poluição, o entupimento de trânsito e despesas de manutenção das estradas.
Agora que 10 milhões de italianos, forçados pelo vírus, rapidamente adotaram o teletrabalho, minimizando seu sentimento de inutilidade e os danos à economia nacional, nos perguntamos por que as empresas não haviam adotado antes uma forma de organização tão eficaz e enxuta. A resposta está naquilo que os antropólogos definem como “cultural gap” —lacuna cultural— das empresas, dos sindicatos, dos chefes.
O tempo livre que, até um mês atrás, nos parecia um luxo raro, hoje abunda. O espaço, que nas cidades vazias se dilatou, por sua vez falta nas casas. Por isso, estamos apreciando a ajuda que nos chega da internet, graças à qual, mesmo permanecendo forçosamente distantes, é possível nos reunirmos virtualmente, nos informarmos, nos confrontarmos, nos encorajarmos.
Nessa reclusão, os jovens têm a maior vantagem, graças à sua facilidade com os computadores, enquanto os velhos têm mais vantagem por serem mais independentes, mais acostumados a estar em casa, fazendo pequenos trabalhos e jogos sedentários, contentando-se com a televisão.
Em todos se insinua o medo de que, mais cedo ou mais tarde, possa terminar o abastecimento dos mantimentos. O colapso da economia torna-se cada vez mais inevitável, já que tanto a produção como o consumo encontram-se bloqueados.
Há alguns anos, Kennet Building, um dos pais da teoria geral dos sistemas, comentando a sociedade opulenta, afirmou: “Quem acredita na possibilidade do crescimento infinito num mundo finito ou é louco ou é economista”. E Serge Latouche acrescentou: “O drama é que agora somos todos mais ou menos economistas. Aonde estamos nos encaminhando? Diretamente contra um muro. Estamos a bordo de um bólido sem piloto, sem marcha a ré e sem freios que irá se chocar contra os limites do planeta”. Latouche propõe abandonar a sociedade de consumo com um decrescimento planificado, progressivo e sereno.
A marcha a ré e os freios que a cultura neoliberal se recusou obstinadamente a usar agora foram desencadeados: não graças a uma revolução violenta, mas sim a um vírus invisível que um morcego soprou sobre a sociedade opulenta, obrigando-a a se repensar.
“A Peste” (1947), obra-prima profética de Albert Camus, talvez possa nos ajudar nesse repensar. Naquele romance, a ciência era protagonista, ou seja, o médico Bernardo Rieux, ocupado até o fim, como médico e como homem, de socorrer os contagiados, enquanto “o cheiro de morte emburrecia todos os que não matava”.
Hoje, nós também, como o nosso tão humano irmão Rieux, estamos presos num limbo entre o pesar e a esperança, no qual temos que aprender que “a peste pode vir e ir embora sem que o coração do homem seja modificado”; que “o bacilo da peste não morre nem desaparece nunca, que pode permanecer adormecido por décadas nos móveis e nas roupas, que espera pacientemente nos quartos, nas adegas, nas malas, nos lenços e nos papéis, que talvez chegue o dia em que, infortúnio ou lição aos homens, a peste acordará seus ratos para mandá-los morrer numa cidade feliz”.
Domenico De Masi, sociólogo italiano, é autor dos livros “Ócio Criativo” e “O Futuro do Trabalho”.
Thomas Friedman, um dos colunistas mais influentes do mundo, ouviu três médicos e escreveu o artigo mais contundente até agora sobre o risco do lockdown global se estender por muito tempo.
No texto, publicado hoje à tarde no The New York Times, Friedman nota que os políticos estão tendo que tomar “decisões enormes de vida ou morte, enquanto atravessam uma neblina com informação imperfeita e todo mundo no banco de trás gritando com eles. Eles estão fazendo o melhor que podem.”
Mas com o desemprego se alastrando pelo mundo tão rápido quanto o vírus, “alguns especialistas estão começando a questionar: ‘Espera um minuto! O que estamos fazendo com nós mesmos? Com nossa economia? Com a próxima geração? Será que essa cura — mesmo que por um período curto — será pior que a doença?’”
Friedman diz que as lideranças políticas estão ouvindo o conselho de epidemiologistas sérios e especialistas em saúde pública. Ainda assim, ele diz que o mundo tem que ter cuidado com o “pensamento de grupo” e que até “pequenas escolhas erradas podem ter grandes consequências.”
Para ele, a questão é como podemos ser mais cirúrgicos na resposta ao vírus de forma a manter a letalidade baixa e ao mesmo tempo permitir que as pessoas voltem ao trabalho o mais cedo possível e com segurança.
Friedman diz que “se a minha caixa de email for alguma indicação, uma reação mais inteligente está começando a brotar.”
Ele cita um artigo publicado semana passada pelo Dr. John P. A. Ioannidis, um epidemiologista e co-diretor do Centro de Inovação em Meta-Pesquisa de Stanford. No artigo, Ioannidis diz que a comunidade científica ainda não sabe exatamente qual é a taxa de mortalidade do coronavírus. Segundo ele, “as evidências disponíveis hoje indicam que a letalidade pode ser de 1% ou ainda menor.”
“Se essa for a taxa verdadeira, paralisar o mundo todo com implicações financeiras e sociais potencialmente tremendas pode ser totalmente irracional. É como um elefante sendo atacado por um gato doméstico. Frustrado e tentando fugir do gato, o elefante acidentalmente pula do penhasco e morre.”
Friedman também cita o Dr. Steven Woolf, diretor emérito do Centro Sobre a Sociedade e Saúde da Universidade da Virgínia, para quem o lockdown “pode ser necessário para conter a transmissão comunitária, mas pode prejudicar a saúde de outras formas, custando vidas.”
“Imagine um paciente com dor no peito ou sofrendo um derrame — casos em que a rapidez de resposta é essencial para salvar vidas — hesitando em chamar o serviço de emergência por medo de pegar coronavírus. Ou um paciente de câncer tendo que adiar sua quimioterapia porque a clínica está fechada.”
Friedman complementa: “Imagine o estresse e a doença mental que virá — já está vindo — de termos fechado a economia, gerando desemprego em massa.”
Woolf, o médico da Virgínia, afirma no artigo que a renda é uma das variáveis mais fortes a afetar a saúde e a longevidade. “Os pobres, que já sofrem há gerações com taxas de mortalidade mais altas, serão os mais prejudicados e provavelmente os que receberão menos ajuda. São as camareiras dos hotéis fechados e as famílias sem opções quando o transporte público fecha.”
Há outro caminho?, pergunta Friedman.
Para ele, a melhor ideia até agora veio do Dr. David Katz, diretor do Centro de Prevenção e Pesquisa da Universidade de Yale e um especialista em saúde pública e medicina preventiva.
Num artigo publicado sexta-feira no The New York Times, o Dr. Katz diz que há três objetivos neste momento: salvar tantas vidas quanto possível, garantindo que o sistema de saúde não entre em colapso, “mas também garantir que no processo de atingir os dois primeiros objetivos não destruamos nossa economia e, como resultado disso, ainda mais vidas.”
Como fazer isso?
Katz diz que o mundo tem que pivotar da estratégia de “interdição horizontal” que estamos empregando agora — restringindo o movimento e o comércio de toda a população, sem considerar a variância no risco de infecção severa — para uma estratégia mais “cirúrgica”, ou de “interdição vertical”.
“A abordagem cirúrgica e vertical focaria em proteger e isolar os que correm maior risco de morrer ou sofrer danos de longo prazo — isto é, os idosos, pessoas com doenças crônicas e com baixa imunidade — e tratar o resto da sociedade basicamente da mesma forma que sempre lidamos com ameaças mais familiares como a gripe.”
Katz sugere que o isolamento atual dure duas semanas, em vez de um período indefinido. Para os infectados, os sintomas aparecerão nesse período. “Aqueles que tiverem uma infecção sintomática devem se auto-isolar em seguida, com ou sem testes, que é exatamente o que fazemos com a gripe. Quem não estiver sintomático e fizer parte da população de baixo risco deveria voltar ao trabalho ou a escola depois daquelas duas semanas.”
“O efeito rejuvenescedor na alma humana e na economia — de saber que existe luz no fim do túnel — é difícil de superestimar. O risco não será zero, mas o risco de acontecer algo ruim com qualquer um de nós em qualquer dia da nossa vida nunca é zero.”
Países asiáticos estão lidando melhor com essa crise do que o Ocidente. Enquanto lá se trabalha com dados e máscaras, aqui se chega tarde e fecham fronteiras
Um oficial de polícia vigia diante de um cartaz dia 23 de janeiro em Pequim.Kevin Frayer/Getty Images
O coronavírus está colocando nosso sistema à prova. Ao que parece a Ásia controla melhor a epidemia do que a Europa. Em Hong Kong, Taiwan e Singapura há poucos infectados. Em Taiwan foram registrados 108 casos e 193 em Hong Kong. Na Alemanha, pelo contrário, após um período muito mais breve já existem 19.000 casos confirmados, e na Espanha 19.980 (dados de 20 de março). A Coreia do Sul já superou a pior fase, da mesma forma que o Japão. Até a China, o país de origem da pandemia, já está com ela bem controlada. Mas Taiwan e a Coreia não decretaram a proibição de sair de casa e as lojas e restaurantes não fecharam. Enquanto isso começou um êxodo de asiáticos que saem da Europa. Chineses e coreanos querem regressar aos seus países, porque lá se sentem mais seguros. Os preços dos voos multiplicaram. Já quase não é possível conseguir passagens aéreas para a China e a Coreia.
A Europa está fracassando. Os números de infectados aumentam exponencialmente. Parece que a Europa não pode controlar a pandemia. Na Itália morrem diariamente centenas de pessoas. Retiram os respiradores dos pacientes idosos para ajudar os jovens. Mas também vale observar ações inúteis. Os fechamentos de fronteiras são evidentemente uma expressão desesperada de soberania. Nós nos sentimos de volta à época da soberania. O soberano é quem decide sobre o estado de exceção. É o soberano que fecha fronteiras. Mas isso é uma vã tentativa de soberania que não serve para nada. Seria muito mais útil cooperar intensamente dentro da Eurozona do que fechar fronteiras alucinadamente. Ao mesmo tempo a Europa também decretou a proibição da entrada a estrangeiros: um ato totalmente absurdo levando em consideração o fato de que a Europa é justamente o local ao qual ninguém quer ir. No máximo, seria mais sensato decretar a proibição de saídas de europeus, para proteger o mundo da Europa. Depois de tudo, a Europa é nesse momento o epicentro da pandemia.
As vantagens da Ásia
Em comparação com a Europa, quais vantagens o sistema da Ásia oferece que são eficientes para combater a pandemia? Estados asiáticos como o Japão, Coreia, China, Hong Kong, Taiwan e Singapura têm uma mentalidade autoritária, que vem de sua tradição cultural (confucionismo). As pessoas são menos relutantes e mais obedientes do que na Europa. Também confiam mais no Estado. E não somente na China, como também na Europa e no Japão a vida cotidiana está organizada muito mais rigidamente do que na Europa. Principalmente para enfrentar o vírus os asiáticos apostam fortemente na vigilância digital. Suspeitam que obig data pode ter um enorme potencial para se defender da pandemia. Poderíamos dizer que na Ásia as epidemias não são combatidas somente pelos virologistas e epidemiologistas, e sim principalmente pelos especialistas em informática e macrodados. Uma mudança de paradigma da qual a Europa ainda não se inteirou. Os apologistas da vigilância digital proclamariam que o big data salva vidas humanas.
A consciência crítica diante da vigilância digital é praticamente inexistente na Ásia. Já quase não se fala de proteção de dados, incluindo Estados liberais como o Japão e a Coreia. Ninguém se irrita pelo frenesi das autoridades em recopilar dados. Enquanto isso a China introduziu um sistema de crédito social inimaginável aos europeus, que permitem uma valorização e avaliação exaustiva das pessoas. Cada um deve ser avaliado em consequência de sua conduta social. Na China não há nenhum momento da vida cotidiana que não esteja submetido à observação. Cada clique, cada compra, cada contato, cada atividade nas redes sociais são controlados. Quem atravessa no sinal vermelho, quem tem contato com críticos do regime e quem coloca comentários críticos nas redes sociais perde pontos. A vida, então, pode chegar a se tornar muito perigosa. Pelo contrário, quem compra pela Internet alimentos saudáveis e lê jornais que apoiam o regime ganha pontos. Quem tem pontuação suficiente obtém um visto de viagem e créditos baratos. Pelo contrário, quem cai abaixo de um determinado número de pontos pode perder seu trabalho. Na China essa vigilância social é possível porque ocorre uma irrestrita troca de dados entre os fornecedores da Internet e de telefonia celular e as autoridades. Praticamente não existe a proteção de dados. No vocabulário dos chineses não há o termo “esfera privada”.
Na China existem 200 milhões de câmeras de vigilância, muitas delas com uma técnica muito eficiente de reconhecimento facial. Captam até mesmo as pintas no rosto. Não é possível escapar da câmera de vigilância. Essas câmeras dotadas de inteligência artificial podem observar e avaliar qualquer um nos espaços públicos, nas lojas, nas ruas, nas estações e nos aeroportos.
Toda a infraestrutura para a vigilância digital se mostrou agora ser extremamente eficaz para conter a epidemia. Quando alguém sai da estação de Pequim é captado automaticamente por uma câmera que mede sua temperatura corporal. Se a temperatura é preocupante todas as pessoas que estavam sentadas no mesmo vagão recebem uma notificação em seus celulares. Não é por acaso que o sistema sabe quem estava sentado em qual local no trem. As redes sociais contam que estão usando até drones para controlar as quarentenas. Se alguém rompe clandestinamente a quarentena um drone se dirige voando em sua direção e ordena que regresse à sua casa. Talvez até lhe dê uma multa e a deixe cair voando, quem sabe. Uma situação que para os europeus seria distópica, mas que, pelo visto, não tem resistência na China.
Na China e em outros Estados asiáticos como a Coreia do Sul, Hong Kong, Singapura, Taiwan e Japão não existe uma consciência crítica diante da vigilância digital e o big data. A digitalização os embriaga diretamente. Isso obedece também a um motivo cultural. Na Ásia impera o coletivismo. Não há um individualismo acentuado. O individualismo não é a mesma coisa que o egoísmo, que evidentemente também está muito propagado na Ásia.
Ao que parece o big data é mais eficaz para combater o vírus do que os absurdos fechamentos de fronteiras que estão sendo feitos nesses momentos na Europa. Graças à proteção de dados, entretanto, não é possível na Europa um combate digital do vírus comparável ao asiático. Os fornecedores chineses de telefonia celular e de Internet compartilham os dados sensíveis de seus clientes com os serviços de segurança e com os ministérios de saúde. O Estado sabe, portanto, onde estou, com quem me encontro, o que faço, o que procuro, em que penso, o que como, o que compro, aonde me dirijo. É possível que no futuro o Estado controle também a temperatura corporal, o peso, o nível de açúcar no sangue etc. Uma biopolítica digital que acompanha a psicopolítica digital que controla ativamente as pessoas.
É possível que no futuro o Estado controle também a temperatura corporal, o peso, o nível de açúcar no sangue
Em Wuhan se formaram milhares de equipes de pesquisa digitais que procuram possíveis infectados baseando-se somente em dados técnicos. Tendo como base, unicamente, análises de macrodados averiguam os que são potenciais infectados, os que precisam continuar sendo observados e eventualmente isolados em quarentena. O futuro também está na digitalização no que se refere à pandemia. Pela epidemia talvez devêssemos redefinir até mesmo a soberania. É soberano quem dispõe de dados. Quando a Europa proclama o estado de alarme e fecha fronteiras continua aferrada a velhos modelos de soberania.
Não somente na China, como também em outros países asiáticos a vigilância digital é profundamente utilizada para conter a epidemia. Em Taiwan o Estado envia simultaneamente a todos um SMS para localizar as pessoas que tiveram contato com infectados e para informar sobre os lugares e edifícios em que existiram pessoas contaminadas. Já em uma fase muito inicial, Taiwan utilizou uma conexão de diversos dados para localizar possíveis infectados em função das viagens que fizeram. Na Coreia quem se aproxima de um edifício em que um infectado esteve recebe através do “Corona-app” um sinal de alarme. Todos os lugares em que infectados estiveram estão registrados no aplicativo. Não são levadas muito em consideração a proteção de dados e a esfera privada. Em todos os edifícios da Coreia foram instaladas câmeras de vigilância em cada andar, em cada escritório e em cada loja. É praticamente impossível se mover em espaços públicos sem ser filmado por uma câmera de vídeo. Com os dados do telefone celular e do material filmado por vídeo é possível criar o perfil de movimento completo de um infectado. São publicados os movimentos de todos os infectados. Casos amorosos secretos podem ser revelados. Nos escritórios do Ministério da Saúde coreano existem pessoas chamadas “tracker” que dia e noite não fazem outra coisa a não ser olhar o material filmado por vídeo para completar o perfil do movimento dos infectados e localizar as pessoas que tiveram contato com eles.
Chineses, todos de máscara, fazem fila no ponto de ônibus em Pequim, em 20 de março.Kevin Frayer / Getty Images
Uma diferença chamativa entre a Ásia e a Europa são principalmente as máscaras protetoras. Na Coreia quase não existe quem ande por aí sem máscaras respiratórias especiais capazes de filtrar o ar de vírus. Não são as habituais máscaras cirúrgicas, e sim máscaras protetoras especiais com filtros, que também são utilizadas pelos médicos que tratam os infectados. Durante as últimas semanas, o tema prioritário na Coreia era o fornecimento de máscaras à população. Diante das farmácias enormes filas se formaram. Os políticos eram avaliados em função da rapidez com que eram fornecidas a toda a população. Foram construídas a toda pressa novas máquinas para sua fabricação. Por enquanto parece que o fornecimento funciona bem. Há até mesmo um aplicativo que informa em qual farmácia próxima ainda se pode conseguir máscaras. Acho que as máscaras protetoras fornecidas na Ásia a toda a população contribuíram decisivamente para conter a epidemia.
Os coreanos usam máscaras protetoras antivírus até mesmo nos locais de trabalho. Até os políticos fazem suas aparições públicas somente com máscaras protetoras. O presidente coreano também a usa para dar o exemplo, incluindo em suas entrevistas coletivas. Na Coreia quem não a usa é repreendido. Na Europa, pelo contrário, frequentemente se diz que não servem para muita coisa, o que é um absurdo. Por que então os médicos usam as máscaras protetoras? Mas é preciso trocar de máscara frequentemente, porque quando umedecem perdem sua função filtradora. Os coreanos, entretanto, já desenvolveram uma “máscara ao coronavírus” feita de nanofiltros que podem ser lavados. O que se diz é que podem proteger as pessoas do vírus durante um mês. Na verdade, é uma solução muito boa enquanto não existem vacinas e medicamentos.
Está surgindo uma sociedade de duas classes. Quem tem carro próprio se expõe a menos riscos
Na Europa, pelo contrário, até mesmo os médicos precisam viajar à Rússia para consegui-las. Macron mandou confiscar máscaras para distribui-las entre os funcionários da área de saúde. Mas o que acabaram recebendo foram máscaras normais sem filtro com a indicação de que bastariam para proteger do coronavírus, o que é uma mentira. A Europa está fracassando. De que adianta fechar lojas e restaurantes se as pessoas continuam se aglomerando no metrô e no ônibus durante as horas de pico? Como guardar a distância necessária assim? Até nos supermercados é quase impossível. Em uma situação como essa, as máscaras protetoras realmente salvariam vidas humanas. Está surgindo uma sociedade de duas classes. Quem tem carro próprio se expõe a menos riscos. As máscaras normais também seriam de muita utilidade se os infectados as usassem, porque dessa maneira não propagariam o vírus.
Nos países europeus quase ninguém usa máscara. Há alguns que as usam, mas são asiáticos. Meus conterrâneos residentes na Europa se queixam de que são olhados com estranheza quando as usam. Por trás disso há uma diferença cultural. Na Europa impera um individualismo que traz atrelado o costume de andar com o rosto descoberto. Os únicos que estão mascarados são os criminosos. Mas agora, vendo imagens da Coreia, me acostumei tanto a ver pessoas mascaradas que o rosto descoberto de meus concidadãos europeus me parece quase obsceno. Eu também gostaria de usar máscara protetora, mas aqui já não existem.
No passado, a fabricação de máscara, da mesma forma que tantos outros produtos, foi externalizada à China. Por isso agora não se conseguem máscaras na Europa. Os Estados asiáticos estão tentando prover toda a população com máscaras protetoras. Na China, quando também começaram a escassear, fábricas chegaram a ser reequipadas para produzir máscaras. Na Europa nem mesmo os funcionários da área de saúde as conseguem. Enquanto as pessoas continuarem se aglomerando nos ônibus e metrôs para ir ao trabalho sem máscaras protetoras, a proibição de sair de casa logicamente não adiantará muito. Como é possível guardar a distância necessária nos ônibus e no metrô nos horários de pico? E uma lição que deveríamos tirar da pandemia deveria ser a conveniência de voltar a trazer à Europa a produção de determinados produtos, como máscaras protetoras, remédios e produtos farmacêuticos.
O presidente da Coreia do Su, terceiro na imagem, em 25 de fevereiro.South Korean Presidential Blue House/Getty Images / South Korean Presidential Blue H
Apesar de todo o risco, que não deve ser minimizado, o pânico desatado pela pandemia de coronavírus é desproporcional. Nem mesmo a “gripe espanhola”, que foi muito mais letal, teve efeitos tão devastadores sobre a economia. A que isso se deve na realidade? Por que o mundo reage com um pânico tão desmesurado a um vírus? Emmanuel Macron fala até de guerra e do inimigo invisível que precisamos derrotar. Estamos diante de um retorno do inimigo? A gripe espanhola se desencadeou em plena Primeira Guerra Mundial. Naquele momento todo o mundo estava cercado de inimigos. Ninguém teria associado a epidemia com uma guerra e um inimigo. Mas hoje vivemos em uma sociedade totalmente diferente.
Na verdade, vivemos durante muito tempo sem inimigos. A Guerra Fria terminou há muito tempo. Ultimamente até o terrorismo islâmico parecia ter se deslocado a áreas distantes. Há exatamente dez anos afirmei em meu ensaio Sociedade do Cansaço a tese de que vivemos em uma época em que o paradigma imunológico perdeu sua vigência, baseada na negatividade do inimigo. Como nos tempos da Guerra Fria, a sociedade organizada imunologicamente se caracteriza por viver cercada de fronteiras e de cercas, que impedem a circulação acelerada de mercadorias e de capital. A globalização suprime todos esses limites imunitários para dar caminho livre ao capital. Até mesmo a promiscuidade e a permissividade generalizadas, que hoje se propagam por todos os âmbitos vitais, eliminam a negatividade do desconhecido e do inimigo. Os perigos não espreitam hoje da negatividade do inimigo, e sim do excesso de positividade, que se expressa como excesso de rendimento, excesso de produção e excesso de comunicação. A negatividade do inimigo não tem lugar em nossa sociedade ilimitadamente permissiva. A repressão aos cuidados de outros abre espaço à depressão, a exploração por outros abre espaço à autoexploração voluntária e à auto-otimização. Na sociedade do rendimento se guerreia sobretudo contra si mesmo.
Limites imunológicos e fechamento de fronteiras
Pois bem, em meio a essa sociedade tão enfraquecida imunologicamente pelo capitalismo global o vírus irrompe de supetão. Em pânico, voltamos a erguer limites imunológicos e fechar fronteiras. O inimigo voltou. Já não guerreamos contra nós mesmos. E sim contra o inimigo invisível que vem de fora. O pânico desmedido causado pelo vírus é uma reação imunitária social, e até global, ao novo inimigo. A reação imunitária é tão violenta porque vivemos durante muito tempo em uma sociedade sem inimigos, em uma sociedade da positividade, e agora o vírus é visto como um terror permanente.
Mas há outro motivo para o tremendo pânico. Novamente tem a ver com a digitalização. A digitalização elimina a realidade, a realidade é experimentada graças à resistência que oferece, e que também pode ser dolorosa. A digitalização, toda a cultura do “like”, suprime a negatividade da resistência. E na época pós-fática das fake news e dos deepfakes surge uma apatia à realidade. Dessa forma, aqui é um vírus real e não um vírus de computador, e que causa uma comoção. A realidade, a resistência, volta a se fazer notar no formato de um vírus inimigo. A violenta e exagerada reação de pânico ao vírus se explica em função dessa comoção pela realidade.
Espero que após a comoção causada por esse vírus não chegue à Europa um regime policial digital como o chinês.
A reação de pânico dos mercados financeiros à epidemia é, além disso, a expressão daquele pânico que já é inerente a eles. As convulsões extremas na economia mundial fazem com que essa seja muito vulnerável. Apesar da curva constantemente crescente do índice das Bolsas, a arriscada política monetária dos bancos emissores gerou nos últimos anos um pânico reprimido que estava aguardando a explosão. Provavelmente o vírus não é mais do que a gota que transbordou o copo. O que se reflete no pânico do mercado financeiro não é tanto o medo ao vírus quanto o medo a si mesmo. O crash poderia ter ocorrido também sem o vírus. Talvez o vírus seja somente o prelúdio de um crash muito maior.
Žižek afirma que o vírus deu um golpe mortal no capitalismo, e evoca um comunismo obscuro. Acredita até mesmo que o vírus poderia derrubar o regime chinês. Žižek se engana. Nada disso acontecerá. A China poderá agora vender seu Estado policial digital como um modelo de sucesso contra a pandemia. A China exibirá a superioridade de seu sistema ainda mais orgulhosamente. E após a pandemia, o capitalismo continuará com ainda mais pujança. E os turistas continuarão pisoteando o planeta. O vírus não pode substituir a razão. É possível que chegue até ao Ocidente o Estado policial digital ao estilo chinês. Com já disse Naomi Klein, a comoção é um momento propício que permite estabelecer um novo sistema de Governo. Também a instauração do neoliberalismo veio precedida frequentemente de crises que causaram comoções. É o que aconteceu na Coreia e na Grécia. Espero que após a comoção causada por esse vírus não chegue à Europa um regime policial digital como o chinês. Se isso ocorrer, como teme Giorgio Agamben, o estado de exceção passaria a ser a situação normal. O vírus, então, teria conseguido o que nem mesmo o terrorismo islâmico conseguiu totalmente.
O vírus não vencerá o capitalismo. A revolução viral não chegará a ocorrer. Nenhum vírus é capaz de fazer a revolução. O vírus nos isola e individualiza. Não gera nenhum sentimento coletivo forte. De alguma maneira, cada um se preocupa somente por sua própria sobrevivência. A solidariedade que consiste em guardar distâncias mútuas não é uma solidariedade que permite sonhar com uma sociedade diferente, mais pacífica, mais justa. Não podemos deixar a revolução nas mãos do vírus. Precisamos acreditar que após o vírus virá uma revolução humana. Somos NÓS, PESSOAS dotadas de RAZÃO, que precisamos repensar e restringir radicalmente o capitalismo destrutivo, e nossa ilimitada e destrutiva mobilidade, para nos salvar, para salvar o clima e nosso belo planeta.
Byung-Chul Han é um filósofo e ensaísta sul-coreano que dá aulas na Universidade de Artes de Berlim. Autor, entre outras obras, de ‘Sociedade do Cansaço’, publicou há um ano ‘Loa a la tierra’, na editora Herder.
In early February, I was working from home when I received a message informing me—and all the other professors at my university in China—that courses would be taught online because of the novel coronavirus. I was already feeling anxious about the mounting epidemic, and my university had locked its doors a few days earlier. Then, when I realized I’d have to teach students online, my anxiety level grew. I didn’t have any experience with online teaching platforms. I was also skeptical about how effective they’d be. “How will I gauge the students’ reactions to my lectures through a computer screen?” I wondered. “Will they learn anything?”
I live in Xuzhou, China—roughly 500 kilometers from Wuhan, the epicenter of the COVID-19 pandemic. Unlike Wuhan, my city isn’t on lockdown, but residents have been discouraged from going outside and many businesses and institutions are closed. I’ve spent most of the past 2 months at home, along with my wife and daughter, fearful of the future and wondering when life will get back to normal.
Thankfully, none of my family members, friends, or colleagues have tested positive for the novel coronavirus. Working from home is also possible for me because my research doesn’t involve lab work. But the spread of the virus and the rapidly rising death toll have weighed heavily on my mind. I’ve found it difficult to sleep. I’ve also had trouble focusing on work. One day early in the outbreak, I sat down at my computer intending to write a grant proposal. But all I could do was stare at the screen.
Years ago, I’d heard that Taoism philosophies were helpful for finding internal peace. So, I decided to listen to a few recordings. One instructed listeners to “govern [yourself] by doing nothing that goes against nature.” That resonated with me because I realized that I’d been trying to push my anxieties aside and force myself to concentrate on work—an approach that wasn’t working because it didn’t feel natural. From then on, I told myself that it was OK to feel anxious, even if it impeded my work. That helped to lessen my internal struggles.
Over the past 2 months, I’ve also learned how to teach courses online, and I have found unexpected joy in that process—even though I struggled at first. There were multiple online teaching platforms to choose from, and I didn’t know which one was best or how to use it. I opted for a platform that had a large server, thinking that it would cope better with heavy usage. My university provided some helpful guidance, and I also learned through trial and error.
I’ve spent most of the past 2 months at home … wondering when life will get back to normal.
My first lecture was especially difficult because I couldn’t see the students’ faces. I was accustomed to lecturing in front of an audience. Online, I felt like I was speaking at my students but not getting anything in return. I communicated with a few of them afterward to get their feedback and they agreed with me, saying that I needed to find a way to make my lectures more interactive. So, I started to encourage my students to leave questions for me in the platform’s comment section during my lectures.
Almost immediately, my students started peppering me with questions. I was surprised by the level of engagement. In a normal classroom setting, they are afraid to raise their hands; most wait until after the lecture is over to approach me and ask a question. But online, students were more comfortable sharing their questions in front of the entire class. That was a great outcome because if one student has a question, it’s likely that another student has the same question and would benefit from hearing the answer. I’ve also been pleased to see from the homework assignments that they are following my teaching well.
China was the first country to close its universities, but over the past month, universities in Italy, the United States, and elsewhere have made similar moves. I hope that my story can provide inspiration for academics who are fearful of what’s to come. It’s OK to feel anxious. But I’d also recommend staying open to change. You never know what you’ll learn.
There is a post circulating on Facebook that tells the following story: someone once asked the famous American anthropologist Margaret Mead what she considered the first evidence of human civilization. This was a heated debate in the mid-20th century in anthropology. Some authors said that the mark of the rise of civilization was the appearance of symbolic language (the ability to use metaphors, for example). Others said that the starting point was the emergence of the perception that some forms of behavior – such as incest – were unacceptable. Others, the invention of hunting tools. Still others, the creation of religious artifacts. Margaret Mead’s response was surprising: she said that the beginning of humanity was represented in a femur, found in an archaeological site dated 15,000 years ago. This bone had the mark of a fracture that had been healed (this story is narrated in the book The Best Care Possible: A Physician’s Quest to Transform Care Through the End of Life, Avery, 2012).
Mead’s explanation was as follows: no animal, in wild conditions, is able to survive with a fractured femur bone. Such an animal would be killed by another animal, or by the likely infection, before the bone could be repaired. In this way, the existence of a cured 15,000-year-old femur means that the individual to whom the bone belonged was helped by her peers, who cared for, protected, and provided her food for a long period of time, so that calcification of the bone was possible. Mead’s argument was, therefore, that the hallmark that defines human civilization is care for those who are sick or in a situation of vulnerability. To be human is to empathize with others.
It happens, however, that the journey of Western civilization – the most materially rich and powerful in the entire history of mankind – ended up producing, from the 19th century on, ways of life guided by individualism and hedonism (which is the idea that the purpose of human existence is to enjoy life, to have pleasure). Individualism and hedonism together produce selfish ways of understanding the world and life.
In the midst of the COVID-19 crisis, we see the Western world torn between selfish tendencies and the ability to empathize with those at risk. Selfish tendencies are visible when, for example, someone runs to the supermarket and buys all available bottles of alcohol gel, before others do it; or when the (usually healthy) young person thinks that, because she has a very high chance of recovery if infected, she does not have to worry so much about contracting the virus. Empathetic behavior is visible when someone offers to shop for the old couple who live in the condo, so that they do not need to leave home; or when the young person, who is generally healthy, stays at home when she realizes that she has the symptoms of the virus, so that medical attention and test kits for detecting the disease are used in those who are really in serious condition. Or even when someone realizes that many children in public schools need the food they receive there, and if they stay at home they will go hungry, and organize food collection and distribution for the families of such children.
Historically speaking, major epidemics have tended to turn the scales towards empathy (even though most people remain in a state of selfish panic). An article published in 2018 in the British newspaper The Guardian (https://bit.ly/39Y7L2p) described how the Spanish flu that killed more than 10 million people in 1918 was important in creating the welfare state in Sweden, and resulted in the fact that the country, one of the richest on the planet, has very low social inequality. The high mortality of the Spanish flu has disorganized society in such a way that injustices and inequalities that existed but were invisible came to the fore.
We can say that the epidemiological crisis can be understood, among many other more dramatic things, as a great sociological experiment. In other words, it is possible to observe things and behaviors that, in more “normal” situations, would not be visible. In this experiment, one could observe how this clash between individualistic selfishness and empathic behavior is unfolding in each location. Is there a turn towards empathy, or what characterizes most collective behavior is individualistic selfishness? What could be done so empathetic attitudes are promoted and amplified? And will people who feel more stimulated to be supportive and behave empathically continue to behave this way after the end of the crisis? In other words, will the epidemic produce real changes in society, as occurred in Sweden in 1918?
Another interesting thing that may help us think about the current crisis in different keys is that epidemics have important roles in the formation of contemporary civilization. Yuval Harari mentions that in chapter 5 (“The biggest fraud in history”) of his book Sapiens. Epidemics started to be part of human life at the time when plants and animals were domesticated, and most human groups started to live on the same land, practicing agriculture. Cities emerged, throughout history, without sanitary infrastructure, and this favored microorganisms that lived more or less in balance with the local ecology to start causing epidemics. From the invention of agriculture in the Middle East to the invasion of the Americas by Europeans, 10,000 years have passed. In these 10,000 years, epidemics of all types have overwhelmed the populations of Eurasia. What is the result of this? Natural selection: the European human being of the 15th century had immunity to a large number of microorganisms to which the indigenous populations of the Americas were not immune. This is one of the reasons (not the only one) why it was Europe that invaded the Americas, and not the Americas that invaded Europe. More than 90% of the entire indigenous population of the Americas died in the next 150 years, almost all due to epidemics brought by Europeans. There are authors who suggest that the carnage that victimized the original peoples was so intense that, when the forests grew on the rubble of decimated civilizations, they sequestered so much carbon from the atmosphere that it caused the planet to cool down (an event that became known as the small medieval ice age – see https://bit.ly/38TeoBC).
The interesting and delicate point here is the idea that epidemics can have other effects on populations besides simply causing a part of them to die. In fact, this is a poorly understood question of Darwin’s natural selection: the “advance” of a species, through adaptation to an ecosystem, depends on the death of a large number of individuals. Harari puts the question sharply in his book: evolution works for the species, not the individual. Of course, almost all of humanity’s efforts since it emerged have focused on disabling the mechanisms of natural selection. If we go back to our 15,000 year old ancestor, with a broken femur, whose colleague decided that, instead of letting her friend die and keep her food, she would donate her energy, time and resources (food, water, fire) so that the companion could recover, we will see that, at that very moment, humanity began to walk away from pure and simple natural selection, towards empathy. In fact, Darwin himself stated that empathy is a human quality that maximizes the survival of the species (today we know that many animals also experience feelings of empathy).
There are many interesting things to be discussed here. One is that, even if things are to be understood scientifically, one cannot approach the world from the point of view of the navel of humans concerned only with themselves.
Everyone is making the necessary arrangements for the difficult period that has started. One suggestion is that, in the list of things to be provided, between alcohol gel and toilet paper, one should insert something that, it seems to me, is extremely important, but few people have thought about it: it is time to resolve that fight that made relatives break up and stop talking to each other; it’s time to put pride aside and forgive father, mother, grandmother, grandfather, sister, brother, son, daughter, friends, neighbors, and whoever else, of whom we parted, it doesn’t matter the cause of the issue.
I don’t know if people realized what is coming. I’ll put it in numbers, and you do your math. Today I have 2600 friendships on Facebook. If the medical authorities’ projections are correct, 80% will be contaminated: 2080 friendships. If we repeat the history of Italy, about 8% will die: 166 friendships. Perhaps I have an effective personal relationship with about 1/3 of this group: 55 people. Add to that that most people over 60 that I know don’t have a Facebook account. Roughly estimating, there may be another 100 people. Chinese data suggest that for the 60 to 69 age group, the average mortality is 4.6%; 70 to 79, 9.8%, 80 and above, 18%. Estimating an average of 10%, of the 100 people I mentioned, probably 10 will die. Adding to the 55 I mentioned above, the result is 65.
The question is: am I prepared for 65 people in my affective circle to die in the next two months?
It is not about the number, the percentages. There is a much smaller group of people with whom I am viscerally connected, and where someone will certainly die.
Unfortunately our world has spent the last century and a half preaching productivism and meritocracy, transforming our perception of the body and life so that we now see them as productive resources. The West and its satellites (like Brazil) have become more affluent, and at the same time immensely less able to make sense of the experience of death. Look inside universities and see where there is something that prepares someone for death. Perhaps the only thing to be found is, in anthropology, the information that a great number of non-Western(ized) peoples on the planet have philosophies, ethics and pedagogies for death. They are less affluent, but their cultural context gives them tools so that they, if they know how to use them well, have a good death. The very strangeness caused by the expression “good death” shows us how unprepared we are for what is coming.
There is no time for great philosophical-existential revolutions now. But there is time for the individual to pick up the phone, call the father, mother, son, etc. with whom she or he no longer speaks or for whom she or he feeds rotten emotions, and resolve the issue. And the resolution is not to revive the fight, but to forgive.
We all have to do this, wholesale, before it’s too late. We may not know how to die, but at least we can give each other the chance to die in peace.
This molecule has been used for different purposed against several conditions hepatatis A and B, also all kinds of leukemia, dengue, explained the professor in an exclusive interview with teleSUR. | Photo: teleSUR
Published 17 March 2020
For 40 years, Cuba has been using a molecule named Interferon Alpha 2B , which has successfully been used to combat the new Coonavirus in China and elsewhere.
“The world has an opportunity to understand that health is not a commercial asset but a basic right,” Cuban doctor Luis Herrera, the creator of the Interferon Alfa 2-B medication, one of the most successful medications in the fight against COVID-19 told teleSUR Tuesday.
Interferon has been known for more than 40 years: first, it was produced from original sources in local sites, then nationally and later in the United States and even Finland.
“At the beginning of the 80s, an important professor from Houston came to Cuba and advised our President Fidel Castro than the Interferon we had here was a very interesting molecule for a different purpose,” Herrera told teleSUR.
“Then a group of people went to Finland to get training in the production of interferon,” while people were also producing Interferon from recombined sources using genetic engineering.
The first one was Beta Interferon in Japan, and the second one was the family of Alpha Interferon by Genetec in California, according to the Cuban doctor.
“One year later in Cuba, we cloned different genes of Interferon from local sites, and we started to produce Interferon in 1981 and 1982, which we used in the outbreak of dengue fever, and we presented the results in the United States in California.”
One of the ways the virus can multiply inside the cells is by decreasing the levels of Interferon naturally produced in human cells. The molecule thus, through a different metabolic way, can create conditions to limit the replication of the virus.
During the MERS-CoV epidemic three years ago – another type of coronavirus – people realized that Interferon was decreased during the replication of the virus, highlighted Herrera.
In China, practically a few weeks after the beginning of the outbreak, people started to use Interferon in a way to avoid complications in people infected with the virus. According to Herrera, this molecule has “some side effects but not too critical.”
“The main idea of Interferon is just to avoid complications,” he told teleSUR. “Young people and people with a good immuno-response perhaps don’t need the medicine or people who won’t have complications and respond to the virus-like any other flu, but old people or people susceptible to have a bad immuno-response will have better chances of avoiding complications by using Interferon.”
He concluded that Cuba must participate in this solidarity movement with other nations, just “the same way other countries have had solidarity with Cuba, especially with Latin American and African countries.”
“We have more physicians working abroad than practically any other country in the world, not because we are exporting anything but simply because we want to participate in building a world with better health conditions and living conditions.”
As of March 15¹, Korea has 8162 infections, but only 75 deaths, a death rate of 0.91%. By comparison, Italy has 24,747 infections and 1809 deaths, a death rate of 7.3%.
The WHO is distributing inadequate Coronavirus treatment guidelines for worldwide use, which Italy is following.
There is no specific treatment for the disease caused by a new coronavirus.. Treatment is based on the patient’s symptoms and supportive care can be very effective. Specific therapies and vaccines are being studied.
However, both Korea and China have been treating infections with drugs known as Chloroquine (long known to treat malaria) or Kaletra (used for the treatment of HIV/AIDS, contains lopinavir/ritonavir ).
The New York Times ran a major story of two 29 year old female Wuhan medical professionals, one who died, and one who lived. The one who lived was treated with Kaletra. The one who died was not treated with either chloroquine or Kaletra.
The New York Post has a similar story of a New Jersey healthcare worker who was on the verge of dying. He was only saved because Chinese family members reached out to doctors in Wuhan who told them to begin immediate treatment with either chloroquine or Kaletra.
He said “Fortunately I have the resources and knowledge about it. I would be dead and gone already. Most medical providers here don’t know about it. Medical providers need to communicate with Chinese medical teams.”
In the (now removed / archive) WHO public guidelines for coronavirus treatment published 13 March 2020, there is no mention of either chloroquine or Kaletra.
Instead the WHO guidelines state:
“There is no current evidence to recommend any specific anti-COVID-19 treatment for patients with confirmed COVID-19”
We find the same from the CDC in the USA. In the official CDC clinical guidance (archive) published on March 7, 2020 Chloroquine is only mentioned in an unrelated footnote and Kaletra is not mentioned at all. The CDC states:
“There are currently no antiviral drugs licensed by the U.S. Food and Drug Administration (FDA) to treat patients with COVID-19.”
Since three major countries (Italy, USA, Australia) appear to be following incorrect WHO treatment guidelines, it likely means that this is a problem in most other countries as well.
Why aren’t our usual medical channels getting this information themselves?
This is a problem from the top down. Western healthcare has already become very complex and government employees are risk averse. They are not used to situations where critical drug treatments need to be made available within a few weeks. China made it a national priority to solve the problem, so normal drug market approvals were waived. WHO was also very delayed² in declaring a pandemic. WHO also didn’t do a good job on the ebola outbreak.
In addition, WHO has been reported to spend³ more than $200M/year on travel expenses, more than it spends on fighting many major problems.
If Italy had the same treatment success rate as Korea, with only 0.91% of people dying instead of 7.3%, then there would be 227 deaths in Italy instead of 1809. 1582 more people would be alive now.
How many people will be dead when the next exponential waves of the virus hit worldwide?
In fact all these deaths aren’t the real problem
The real problem from this pandemic is that because the virus is so infectious, even though it is fairly mild for most people, a large number become severely ill and require hospitalization. This large number of severely ill people overwhelms the entire hospital system. The population is then forced into quarantine to slow down the rate of infections, which can lead to a total breakdown of society.
Using these treatment options, the majority of people will be kept out of hospital entirely. Both the Koreans and Chinese guidelines make it clear that people should be treated very early if the infection progresses beyond a mild case.
This is likely the reason the medical system in Italy is currently overwhelmed.
The most important thing you can do is make your local healthcare system and government aware of this problem. If you’re successful, you’ll save lives.
What if you get sick?
Korea is one of the countries with the most experience with the virus and their treatment has proven results.
If you get sick I suggest you closely study the official Korean medical guidelines (archive) and find a doctor that will treat you according to those guidelines. Don’t self-treat, as these are powerful drugs that have side effects and interactions with other drugs. You could easily overdose and die. Many people died of aspirin overdose during the 1918 Spanish Flu pandemic⁴. Only in an emergency would I use this information to treat myself (and I certainly would if I had no other choice).
In addition, it appears we now have 3 additional treatment options, giving us a total of 5 treatment choices depending on individual tolerances and availability.
You don’t need to get these drugs yourself. Chloroquine is readily available to your doctor and it is an inexpensive, off patent drug that has been used clinically since 1947. It can be easily produced in massive quantities even if there are temporary shortages⁵.
About me
I used to work in Silicon Valley tech. I’m now interested in using Chinese philosophy to find truth in complex situations. I lived at Wudang Mountain, Hubei Province, China from 2014 to 2016. I did this research because my mother is in a high risk category in Australia.
Many of you will already be familiar with the FLICC graphic which shows the 5 main characterstics of (climate) science denial, namely fake experts, logical fallacies, impossible expectations, cherry picking and conspiracy theories. It was first introduced when our MOOC “Denial101x – Making sense of climate science denial” launched in April 2015.
In the five (!) years since, John Cook and colleagues have been busy refining and enlarging this fallacy taxonomy as explained in a series of three new videos for Denial101x. Here is the first of them:
We recently received an email from a current Denial101x student suggesting to make the fallacy icons available as emojis to have them readily available when responding to comments on social media. While this might not be quite as easy as it sounds (anybody know?), it gave us another idea: make the current set of fallacy icons available on Wikimedia commons! So, this is what we did! The significantly larger taxonomy makes for a good entry point:
The individual icons can be found on the page listing all of our uploaded files (which we plan to add to soon with more fallacy icons as well as other graphics from our large collection – please feel free to help us decide which ones to upload by posting a comment!).
And to state the obvious: these fallacies not only plague climate science but also many other scientific discussions. It for example didn’t take long for them to appear with the ongoing COVID-19 pandemic as John Cook noted in a recent tweet sharing the taxonomy graphic:
“Seeing the same fallacies & science denial techniques proliferate with coronavirus as they do with climate science denial inspired me to post the latest version of the FLICC taxonomy, documenting many of the techniques found in science misinformation.“
The individual icons will therefore hopefully come in handy to call-out fallacies regardless of the topics they show up with!
Editor’s note: We are not a virus, unless we act like one. Read: Basic Goodness. ~ Waylon, ed.
Renowned Indian spiritual teacher, Preethaji, spoke of the coronavirus a few weeks back.
What she said in her Facebook video might not be what we want to hear, but it’s absolutely what we need to understand.
For millions of years, every single species has had its role in the universe. However, we are the species who has done the most damage on Earth and, unfortunately, continues to do so. Preethaji eloquently explains how we kill other species for pleasure and superiority rather than survival.
Throughout all our undesirable actions, we forget the consequence. But it would seem that nature’s living intelligence does not. Perhaps, as Preethaji puts it, the coronavirus—like many natural disasters and diseases—is eliminating what doesn’t support the whole.
The death toll from the coronavirus is increasing by the day. It’s sad to see how many families and nations are affected by this tragedy. Nevertheless, in order to live a brighter future on earth, we must examine our contribution to life’s continuity.
Ask yourself today:
How are my actions affecting me and others?
Do I understand that I’m part of the whole and not a separate entity?
What can I do to create a more awakened and conscious future?”
~
It’s time to change our toxic habits and patterns. May this virus outbreak help us forge a healthier lifestyle and an awakened state of mind.
A woman wears a face mask amid coronavirus fears in Iraq. Getty Images
After years of urging its terrorists to attack major European cities, ISIS is now telling them to steer clear due to the coronavirus.
Any sick jihadists already in Europe, however, should stay there — presumably to sicken infidels, according to a “sharia” directive printed in the group’s al-Naba newsletter, the Sunday Times of London reported.
The “healthy should not enter the land of the epidemic and the afflicted should not exit from it,” the newsletter advised.
The newsletter instructs jihadists that the “plague” is a “torment sent by God on whomsoever He wills.”
Iraq, where most of the surviving fragments of the group remain, had 110 reported coronavirus cases on Sunday morning, 10 of them fatal, according to Johns Hopkins University, which is tracking the contagion.
A epidemia do coronavírus no mundo está evidenciando as desigualdades sociais, apesar de aparentemente o vírus contaminar todos e, neste primeiro momento, pessoas das classes média e alta que viajaram para o exterior. De fato, o que salta aos olhos neste momento da epidemia é o fato dela ter tomado uma dimensão na cobertura jornalística muito maior que outras epidemias que ainda hoje vitimam mais pessoas, como a dengue e o sarampo.
À primeira vista, isto ocorre justamente por uma questão de classe: como o epicentro atual do coronavírus é a Europa e não o continente africano ou latino-americano, a visibilidade desta epidemia é muito maior. Uma lógica que também esteve presente quando a mídia hegemônica em todo o mundo, inclusive o Brasil, mobilizou os sentimentos de consternação no ataque do grupo terrorista Exército Islâmico à Paris em 2015. O grupo Boko Haram praticou ataques terroristas até mais violentos em 2019 na Nigéria sem a mesma repercussão.
Mas o classismo e o racismo também estão neste caso do coronavírus. E é importante este alerta porque há ideias entre algumas pessoas da periferia de que se trata de “doença de gente rica” e, portanto, não deveria ser objeto de preocupação da população da quebrada. Se não ficarmos atentos, pode-se em pouco tempo haver um deslocamento do epicentro da doença para a periferia e, por conta disto, sem a visibilidade que ela tem agora.
Uma análise de algumas medidas de contenção do vírus: a ordem é sair pouco de casa, procurar trabalhar em “home-office”, transferir as atividades didáticas de escolas e universidades para a modalidade online, suspender viagens internacionais, entre outros. Note-se que os atores atingidos por estas medidas protetivas são aqueles que não estão na maior parte do trabalho precarizado e informal. Se nas universidades as aulas foram suspensas e algumas adotaram o sistema de ensino à distância, como ficam os funcionários operacionais terceirizados? Evidente que eles continuarão trabalhando.
Há o caso relatado pelo colunista Lauro Jardim, do Globo, do empresário e sua esposa que contraíram o vírus em uma viagem, se colocaram em quarentena no apartamento deles porém obrigaram a empregada doméstica a continuar indo trabalhar desconsiderando o alto risco dela se contaminar.
Com isto, em um primeiro momento, observa-se que tais medidas, ao mesmo tempo que visam proteger um determinado segmento da sociedade, deixam o outro completamente desprotegido. Estes trabalhadores operacionais e precarizados se deslocam para suas casas de transporte coletivo, um ambiente potencialmente explosivo para uma contaminação massiva.
Esta situação se agrava por dois motivos conjunturais: o primeiro é a desregulamentação do trabalho imposta pela direita em todo o mundo e aplicada no Brasil com maior intensidade no ano passado. A lógica desta proposta é: o ganho depende de quanto trabalha e não de quanto é necessário para sobreviver. Empregadas domésticas, faxineiras, trabalhadores de aplicativos, ambulantes, flanelinhas, motoboys, cicloboys, entre outros teriam que optar entre ficar sem dinheiro ou sair as ruas em busca de trabalho. Ainda que estes trabalhadores contraiam o vírus e fiquem doentes, a tendência é que eles continuem trabalhando pois no mercado informal não tem nenhum tipo de proteção. Imagine este cenário de pessoas com o COVID-19 nas ruas entregando comida, dirigindo Uber, motos, vendendo coisas nas ruas, limpando casas… Imaginem estas pessoas andando nos trens, ônibus, metros lotados. O vírus vai para a periferia, mas volta com tudo pois estas pessoas atendem justamente estes que se julgariam protegidos. O risco é intensificar comportamentos de cunho fascista, racista, xenofóbico.
O segundo motivo é o desmonte do sistema público de saúde que está enfraquecido para o enfrentamento massivo desta epidemia. Este é o momento que mais se precisa do SUS e todo o seu arcabouço de atendimento, prevenção, medicina da família, entre outros. E da estrutura dos laboratórios públicos de pesquisa das universidades e institutos como o Fiocruz, Manguinhos, FURP e das universidades públicas.
Só para lembrar: 47,3% dos trabalhadores negros estão no mercado informal, 80% dos usuários do SUS se declaram negros. Em outras palavras, estamos falando de situações que atingem a população negra na sua maioria.
Daí que é o momento ímpar para se retomar a pactuação político-social da Constituinte de 1988 e barrar as mudanças de cunho neoliberal que tem sido feitas desde o golpe de 2016. É necessário revogar a emenda constitucional do teto de gastos, fortalecer o SUS e os laboratórios públicos e centrar a política de Estado não no “equilíbrio fiscal para obter a confiança dos mercados”, mas na capacidade de atendimento social massivo para garantir o bem-estar de todos os cidadãos.
*Este artigo não reflete, necessariamente, a opinião da Fórum
O perigo que a atual epidemia do COVID-19 representa para as populações pobres de todo o mundo vem sendo quase completamente ignorado pelos jornalistas e governos do ocidente.
O coronavírus1 é o velho filme que temos assistido repetidas vezes desde que o livro Zona Quente, de Richard Preston, nos introduziu em 1995 ao demônio exterminador nascido em uma misteriosa caverna de morcegos na África Central e conhecido como Ebola. Aquele foi apenas o primeiro de toda uma sucessão de novas doenças irrompendo no “campo virgem” (esse é o termo adequado) dos sistemas imunes inexperientes da humanidade. Depois do vírus da Ebola, logo se seguiu a influenza aviária, que os humanos pegaram em 1997, e a SARS, que surgiu no final de 2002. Em ambos os casos, a doença surgiu primeiro em Guangzhou, o polo manufatureiro mundial.
Hollywood, é claro, abraçou com tudo esses surtos e produziu uma série de filmes para nos provocar e amedrontar – Contágio (2001), dirigido por Steven Soderbergh, se destaca pela precisão científica e pela sua espantosa antecipação do caos atual.) Além dos filmes e dos inúmeros romances lúgubres, centenas de livros de milhares de artigos científicos responderam a cada surto, muitos deles sublinhando o estado deplorável da prevenção e preparação emergencial global de se detectar e reagir a tais doenças novas.
Caos numérico
Assim, o coronavírus atravessa nossa porta da frente como um monstro já familiar. Sequenciar seu genoma (aliás muito semelhante ao de sua irmã, a amplamente estudada SARS) foi moleza. Ainda nos faltam, no entanto, os pedaços mais vitais de informação. À medida que os pesquisadores trabalham noite e dia para conseguir caracterizar o surto, eles enfrentam três enormes desafios. Em primeiro lugar, a continuada escassez de kits para diagnóstico da infecção viral, especialmente nos Estados Unidos e na África, tem impedido a projeção de estimativas precisas de parâmetros-chave, tais como a taxa de reprodução, o tamanho da população infectada e a quantidade de infecções de caráter benigno. O resultado vem sendo um completo caos numérico.
Alguns países, contudo, dispõem de dados mais confiáveis a respeito do impacto do vírus em certos grupos. E as informações são muito assustadoras. A Itália, por exemplo, registra uma espantosa taxa de mortalidade de 23% entre as pessoas maiores de 65 anos de idade; na Inglaterra, a cifra atualmente se encontra no patamar dos 18% para esse grupo. A “gripe corona” que Trump menospreza representa um perigo sem precedentes para populações geriátricas, com um potencial saldo de mortalidade na casa dos milhões.
Em segundo lugar, assim como as influenzas sazonais, o vírus está sofrendo mutações à medida que atravessa populações dotadas de diferentes composições etárias e condições de saúde. A variedade que os estadunidenses têm mais probabilidade de acabar pegando já é ligeiramente diferente daquela identificada no surto original em Wuhan. As futuras mutações do vírus podem tanto ser benignas quanto alterar a distribuição de virulência, que atualmente cresce vertiginosamente a partir dos cinquenta anos de idade A “gripe corona” de Trump representa no mínimo um perigo mortal ao quarto dos estadunidenses que são de idade, possuem sistemas imunes fracos ou problemas respiratórios crônicos.
Em terceiro lugar, mesmo se o vírus permanecer estável e sofrer poucas mutações, é possível que seu impacto sobre coortes etários mais jovens difira radicalmente em países pobres e entre grupos de alta pobreza. Considere a experiência global da gripe espanhola de 1918-19, que, estima-se, matou cerca de 1-2% da humanidade. Nos Estados Unidos e na Europa Ocidental, o vírus original do H1N1 teve maior índice de letalidade em jovens adultos, e a explicação que geralmente se dá para tanto é que seus sistemas imunes relativamente mais fortes acabavam reagindo com demasiada intensidade à infecção e atacarem células pulmonares, o que acarretava uma pneumonia viral e um choque séptico. Mais recentemente, contudo, alguns epidemiologistas levantaram a hipótese de que adultos mais velhos podem ter adquirido “memória imune” por conta de um surto anterior ocorrido na década de 1890s que teria os protegido. De todo modo, é sabido que o vírus original da H1N1 encontrou um nicho privilegiado em acampamentos do exército e em trincheiras de batalha, onde ele ceifou a vida de dezenas de milhares de jovens soldados. Esse tornou-se um fator importantíssimo na batalha entre os impérios. Chegou-se a atribuir o colapso da grande ofensiva alemã na primavera de 1918, e portanto o resultado da guerra, ao fato de que os Aliados, em contraste com seu inimigo, tinham condições de reabastecer seus exércitos doentes com tropas estadunidenses recém-chegadas.
Já a gripe espanhola em países mais pobres teve um perfil diferente. Raramente se leva em conta que 60% da mortalidade global (e isso representa ao menos 20 milhões de mortes) ocorreu em Punjabi, Pompéia, e em outras partes da Índia Ocidental onde exportações de grão para a Inglaterra e práticas brutais de requisição coincidiram com uma seca generalizada. As escassezes alimentares que resultaram disso levaram milhões de pobres à beira da fome. Essas populações tornaram-se vítimas de uma sinistra sinergia entre subnutrição, que suprimia sua resposta imune à infecção, e surtos desenfreados de pneumonias virais e bacterianas. Em outro caso semelhante, o Irã sob ocupação inglesa, tendo passado por muitos anos de seca, cólera e escassez alimentar, além de um surto generalizado de malária, precondicionou a morte de, estima-se, um quinto da população.
Essa história – especialmente as consequências desconhecidas das interações com subnutrição e infecções existentes – deveria nos alertar que o COVID-19 pode tomar um caminho diferente e mais letal nas favelas densas e insalubres da África e do Sul Asiático. Com casos agora sendo reportados em Lagos, Kigali, Addis Ababa e Kinshasa, ninguém sabe (e nem saberá por um bom tempo por conta da ausência de testes para diagnóstico) de que forma ele pode entrar em sinergia com as condições locais de saúde e as doenças da região. O perigo desse fenômeno para as populações pobres de todo o mundo vem sendo quase completamente ignorado por jornalistas e governos ocidentais. O único artigo publicado que li nesse sentido argumenta que por conta do fato da população urbana da África ser a mais jovem do mundo, a pandemia deve produzir lá apenas um impacto ameno. À luz da experiência de 1918, essa não passa de uma extrapolação tola. Assim como a suposição de que a pandemia, assim como a gripe sazonal, irá recuar diante de climas mais quentes. (Tom Hanks acabou de pegar o vírus na Austrália, onde ainda é verão.)
Um Katrina médico
É possível que daqui a um ano vejamos com admiração o sucesso da China em conter a pandemia, e que fiquemos horrorizados com o fracasso dos EUA. (Estou aqui fazendo a suposição heróica de que a declaração da China de que a taxa de transmissão está diminuindo rapidamente é mais ou menos precisa.) A incapacidade de nossas instituições de manter fechada a Caixa de Pandora, é claro, não é surpresa para ninguém. Desde o ano 2000 temos repetidamente visto colapsos na linha de frente do atendimento de saúde.
Tanto temporada de gripe de 2009 quanto a de 2018, por exemplo, sobrecarregaram hospitais em todo o país, expondo a chocante escassez de leitos hospitalares depois de vinte anos de cortes na capacidade de internação movidos pela maximização dos lucros (a versão do setor hospitalar para a gestão de inventário just-in-time). A crise remonta à ofensiva corporativa que levou Reagan ao poder e converteu lideranças do Partido Democrata em seus porta-vozes neoliberais. De acordo com A Associação Hospitalar Estadunidense, o número de leitos hospitalares sofreu um espantoso declínio de 39% entre 1981 e 1999. O objetivo era elevar os lucros através de um aumento no “censo” (calculado a partir do número de leitos ocupados). Mas o objetivo da gerência de uma taxa de ocupação de 90% significava que os hospitais não tinham mais a capacidade de absorver um influxo de pacientes em situações de epidemia e de emergência médica.
Hospitais privados e de caridade fechando as portas e carências de enfermagem, igualmente provocados pela lógica de mercado, devastaram os serviços de saúde em comunidades mais pobres e em áreas rurais, transferindo o fardo para hospitais públicos subfinanciados e instalações médicas do Departamento de Assuntos de Veteranos dos EUA. Se as condições do atendimento emergencial em tais instituições já são incapazes de dar conta de infecções sazonais, como esperar que elas deem conta de uma iminente sobrecarga de casos críticos?
No novo século, a medicina emergencial continuou a sofrer reduções no setor privado por conta do imperativo de se preservar o “valor dos acionistas”, buscando o aumento de dividendos e lucros de curto prazo, e no setor público por meio de austeridade fiscal e reduções nos orçamentos estaduais e federias de prevenção e preparação emergencial. O resultado disso é que há apenas 45.000 leitos de UTI disponíveis para lidar com a avalanche projetada de casos graves e críticos de coronavírus. (Em comparação, os sul coreanos dispõem de três vezes mais leitos por milhar do que os estadunidenses.) De acordo com uma investigação feita pela USA Today “apenas oito estados teriam leitos hospitalares suficientes para tratar os 1 milhão de americanos de sessenta ou mais anos de idade que podem adoecer de COVID-19”.
Ao mesmo tempo, os Republicanos vem rechaçando todos os esforços de reconstruir as redes de segurança destruídas pelos cortes orçamentários da recessão de 2008. Os departamentos municipais e estaduais de saúde – a primeira (e vital) linha de defesa – dispõem hoje de equipes 25% menores do que crise financeira doze anos atrás. Além disso, ao longo da última década o orçamento dos Centros de Controle e Prevenção de Doenças caiu 10% em termos reais. Desde a coroação de Trump as insuficiências fiscais só se exacerbaram. O New York Times recentemente noticiou que “21% dos departamentos municipais de saúde registraram reduções nos seus orçamentos para o ano fiscal referente a 2017.” Trump também fechou o escritório de pandemia da Casa Branca, uma diretoria instituída pelo Obama depois do surto de Ebola em 2014 para garantir uma resposta nacional rápida e bem-coordenada para novas epidemias.
Estamos nas fases iniciais de um Katrina médico. Ao desinvestirmos em prevenção e preparação emergencial médica no exato momento em que todas as avaliações de peritos recomendam uma expansão generalizada dessas capacidades, nos encontramos em uma situação em que nos faltam tanto suprimentos elementares quanto funcionários públicos de saúde e leitos emergenciais. As reservas nacionais e regionais de mantimentos hospitalares vêm sendo armazenadas em condições muito inferiores às orientações epidemiológicas. Por isso, a débacle de kits para testes de diagnóstico coincidiu com uma escassez crítica de equipamentos protetivos básicos para trabalhadores de saúde.
As enfermeiras militantes, nossa reserva nacional de consciência social, estão garantindo que todos nós compreendamos os graves perigos provocados pelo armazenamento inadequado de mantimentos protetivos essenciais tais como máscaras faciais N95. Elas também nos lembram que os hospitais tornaram-se ambientes ideais para micro-organismos super-resistentes a antibióticos, tais como o C. Difficile, que podem tornar-se seríssimos agentes mortais secundários em alas hospitalares superlotadas. Ainda mais vulneráveis porque invisíveis são as centenas de milhares de trabalhadoras de lares de repouso e as equipes de enfermagem domiciliar, operando em condições de sub-remuneração e sobrecarga de trabalho.
A divisão de classes
O surto expôs instantaneamente a marcada divisão de classes no atendimento de saúde, que a Nossa Revolução colocou na agenda nacional. Em suma: quem dispõe de um bom plano de saúde e também tem condições de trabalhar ou lecionar de casa está confortavelmente isolado, contanto que siga com prudência as diretrizes de segurança. Funcionários públicos e outros grupos de trabalhadores sindicalizados que gozam de uma cobertura decente terão de fazer escolhas difíceis, optando entre renda e proteção. Enquanto isso, milhões de trabalhadores de baixa renda do setor de serviços, trabalhadores agrícolas, desempregados e sem teto estão sendo atirados aos lobos.
Mesmo se Washington eventualmente der conta de resolver o fiasco dos testes e fornecer um número adequado de kits para diagnóstico, aqueles que não dispõem de plano de saúde ainda terão de pagar médicos ou hospitais para que estes apliquem os testes. As contas médicas familiares gerais vão disparar, ao mesmo tempo em que milhões de trabalhadores estão perdendo seus empregos e os planos de saúde fornecidos pelos empregadores. Poderia haver defesa mais forte e mais urgente da proposta de se estender o Medicare para todos?
Mas, como todos sabemos, cobertura universal em qualquer sentido minimamente eficaz requer provisão universal de ausências remuneradas por motivo de saúde. Quarenta e cinco por cento da força de trabalho atualmente tem esse direito negado: essas pessoas são portanto virtualmente compelidos a transmitirem a infecção ou abrirem mão da renda mensal. Da mesma forma, quatorze estados governados pelo Partido Republicano se recusaram a implementar a Affordable Care Act3, que expande o Medicaid aos trabalhadores pobres. É por isso que um em cada quarto texanos, por exemplo, não dispõe de cobertura e só pode contar com a sala emergencial do hospital municipal se precisar se tratar.
As contradições mortais dos planos privados de saúde em uma era de pragas são talvez mais visíveis no setor de enfermagem domiciliar e cuidado assistido, que administra 2,5 milhões de estadunidenses de idade – muitos deles dependentes de Medicare. A situação há muito constitui um escândalo nacional. Trata-se de um setor altamente competitivo, capitalizado em salários baixos, falta de pessoal e cortes ilegais de custos. De acordo com o New York Times, 380.000 pacientes de casas de repouso morrem a cada ano por conta da negligência dessas instalações diante de procedimentos básicos de controle de infecções. Muitas dessas casas de repouso – particularmente em estados do Sul do país – calculam ser mais barato arcar com as multas por violações sanitárias do que contratar funcionários adicionais e treiná-los adequadamente.
Não é de surpreender que o primeiro epicentro de transmissão comunitária foi o Life Care Center, uma casa de repouso em Kirkland, situada nos subúrbios de Seattle. Conversei com Jim Straub, um velho amigo que é líder sindical nas casas de repouso da região de Seattle e está atualmente escrevendo um artigo a respeito do tema para o The Nation. Ele caracterizou a instalação como “sendo uma das piores equipadas em de quadro de funcionários em todo o Estado” e descreveu a totalidade do sistema de casas de repouso de Washington como “o mais subfinanciado do país – um oásis absurdo de sofrimento de austeridade em um mar de dinheiro da indústria de tecnologia de ponta.”
Além disso, ele assinalou ainda que os oficiais de saúde pública estavam ignorando o fator crucial que explica a rápida taxa de transmissão da doença do Life Care Center para dez outras casas de repouso nas proximidades: “trabalhadores de casas de repouso situadas no mercado imobiliário mais caro dos Estados Unidos via de regra trabalham em mais de um emprego, geralmente atendendo em múltiplas casas de repouso.” Ele diz que as autoridades foram incapazes de descobrir os nomes e as localizações desses segundos empregos e assim perderam todo e qualquer controle sobre a disseminação do COVID-19. E até agora ninguém está propondo compensar a remuneração de trabalhadores expostos para que eles permaneçam em casa.
Agora, como nos alerta o exemplo de Seattle, mais dezenas, talvez centenas, de casas de repouso em todo o país deverão se tornar pontos de foco do coronavírus e seus funcionários, muitos deles recebendo o salário mínimo, optarão racionalmente por permanecer em casa a fim de protegerem suas famílias. Numa situação dessas, o sistema poderia entrar em colapso – e ninguém há de esperar que a Guarda Nacional venha cuidar da reposição dos coletores de urina.
Solidariedade internacional
A cada passo de seu avanço mortal, a pandemia promove uma defesa de uma política de cobertura universal e ausência remunerada no trabalho. Enquanto Biden se concentra em arranhar a popularidade de Trump, os progressistas precisam se unir, como propõe Bernie, para vencer a convenção com sua pauta de Medicare para Todos. Juntos, os delegados de Bernie Sanders e Elizabeth Warren têm um papel a desempenhar no Fiserv Forum em Milwaukee em meados de julho2, mas o resto de nós possui uma tarefa igualmente importante nas ruas, começando agora com lutas contra despejos, demissões e empregadores que se recusam a compensar trabalhadores ausentes (Está com medo de contágio? Permaneça a dois metros de distância do próximo manifestante e você ainda garante uma imagem mais poderosa para a TV. Mas precisamos reivindicar as ruas.)
Como sabemos, a cobertura universal é apenas um primeiro passo. É desapontador, para dizer o mínimo, que nos debates das primárias do Partido Democrata nem Sanders nem Warren chamaram atenção para como as grandes corporações farmacêuticas [Big Pharma] abriram mão de investir em pesquisa e desenvolvimento de novos antibióticos e antivirais. Das dezoito maiores empresas farmacêuticas, quinze abandonaram totalmente o campo. Medicamentos cardíacos, tranquilizadores viciantes e tratamentos para impotência masculina são alguns dos produtos mais lucrativos do setor, e não a defesa contra infecções hospitalares, doenças emergentes e doenças letais tradicionais dos trópicos, como a malária. A vacina universal para a influenza – isto é, uma vacina voltada para as partes imutáveis das proteínas de superfície do vírus – já é uma possibilidade há décadas, mas não é lucrativa o suficiente para ser considerada prioridade.
À medida que a revolução dos antibióticos retrocede, velhas doenças deverão reaparecer ao lado de novas infecções e os hospitais se converterão em ossuários. Até mesmo alguém como Trump pode esbravejar oportunisticamente contra os custos absurdos dos medicamentos de prescrição. O que precisamos, no entanto, é de uma visão mais audaciosa voltada para quebrar os monopólios farmacêuticos e fornecer ao público uma produção de medicamentos vitais. (As coisas já foram assim um dia: durante a Segunda Guerra Mundial, o exército convocou Jonas Salk e outros pesquisadores para desenvolverem a primeira vacina de gripe.) Como escrevi quinze anos atrás em meu livro O monstro bate à nossa porta: a ameaça global da gripe aviária:
“O acesso a medicamentos vitais, incluindo vacinas, antibióticos e antivirais, deveria ser um direito humano, universalmente disponível a preço zero. Se os mercados não tiverem condições de fornecer incentivos para produzir tais drogas de maneira barata, então os governos e as organizações sem fins lucrativos deveriam assumir a responsabilidade por sua manufatura e distribuição. A sobrevivência dos pobres deve sempre ser prioridade sobre os lucros do grande complexo farmacêutico [Big Pharma].”4
A atual pandemia expande o argumento: a organização capitalista agora parece estar biologicamente insustentável na ausência de uma infraestrutura verdadeiramente internacional de saúde pública. Mas tal infraestrutura jamais existirá enquanto movimentos de pessoas não quebrarem o poder das grandes corporações farmacêuticas e de um sistema de atendimento à saúde organizado em função do lucro.
Isso exige um projeto socialista independente para a sobrevivência humana, que vai além de um Segundo New Deal. Desde a época do movimento Occupy, os progressistas vem colocado a luta contra a desigualdade econômica e de renda na ordem do dia, um grande feito. Mas agora os socialistas precisam dar o próximo passo e, tendo as indústrias farmacêutica e de saúde como alvos imediatos, lutarem pela propriedade social e a democratização do poder econômico.
Mas precisamos ter uma avaliação honesta de nossas fraquezas políticas e morais. Por mais que tenho visto com entusiasmo a evolução à esquerda de uma nova geração e o retorno da palavra “socialismo” ao discurso político, há um elemento perturbador de solipsismo nacional no movimento progressista que é simétrico ao novo nacionalismo de direita. Tendemos a falar apenas da classe trabalhadora estadunidense e da história radical dos Estados Unidos (talvez nos esquecendo que Eugene V. Debs era um internacionalista até o último fio de cabelo). Às vezes isso passa perto de uma versão de esquerda do bordão “América em Primeiro Lugar”.
Diante dessa pandemia, os socialistas devem aproveitar toda ocasião para lembrar os outros da urgência da solidariedade internacional. Concretamente, precisamos mobilizar nossos amigos progressistas e seus ídolos políticos a fim de reivindicar um aumento massivo na produção de kits para diagnóstico, equipamentos de segurança e medicamentos vitais para serem distribuídos gratuitamente a países pobres. Cabe a nós garantir que o Medicare para Todos torne-se uma tanto uma política externa quanto uma política doméstica nos EUA.
* Texto enviado pelo autor diretamente para o Blog da Boitempo. A tradução é de Artur Renzo.
NOTAS
1 Tem havido muita confusão a respeito da terminologia científica: o Comitê Internacional de Taxonomia de Vírus denominou o vírus de SARS-CoV-2. COVID-19 refere-se ao surto. (Nota do autor). 2O autor refere-se aqui à Convenção Nacional Democrata de 2020, que definirá o candidato que o Partido escolherá para enfrentar Donald Trump nas eleições presidenciais deste ano. A disputa, como se sabe, atualmente entre Joe Biden e Bernie Sanders, e o apoio da base da candidata progressista Elizabeth Warren é um fator crucial para a vitória do Sanders. (Nota da tradução.) 3 O “Patient Protection and Affordable Care Act” é a “Lei Federal de Proteção e Cuidado ao Paciente”, apelidada de “Obamacare”, sancionada pelo presidente estadunidense em março de 2010. (N. T.) 4 Edição brasileira: O monstro bate à nossa porta: a ameaça global da gripe aviária (São Paulo, Record, 2006). (N. T.)
***
Mike Davis nasceu na cidade de Fontana, Califórnia, em 1946. Abandonou os estudos precocemente, aos dezesseis anos, por conta de uma grave doença do pai. Trabalhou como açougueiro, motorista de caminhão e militou no Partido Comunista da Califórnia meridional antes de retornar à sala de aula. Aos 28 anos, ingressou na Universidade da Califórnia de Los Angeles (Ucla) para estudar economia e história. Atualmente, mora em San Diego, é um distinguished professor no departamento de Creative Writing na Universidade da Califórnia, em Riverside, e integra o conselho editorial da New Left Review. Autor de vários livros, entre eles Planeta favela, Apologia dos bárbaros e Cidade de quartzo. O autor também colabora com o livro de intervenção Cidades rebeldes: passe livre e as manifestações que tomaram as ruas do Brasil.
Coronavirus victims in Italy will be denied access to intensive care if they are aged 80 or more or in poor health should pressure on beds increase, a document prepared by a crisis management unit in Turin proposes.
Some patients denied intensive care will in effect be left to die, doctors fear.
The unit has drawn up a protocol, seen by The Telegraph, that will determine which patients receive treatment in intensive care and which do not if there are insufficient spaces. Intensive care capacity is running short in Italy as the coronavirus continues to spread.
The document, produced by the civil protection deparment of the Piedmont region, one of those hardest hit, says: “The criteria for access to intensive therapy in cases of emergency must include age of less than 80 or a score on the Charlson comorbidity Index [which indicates how many other medical conditions the patient has] of less than 5.”
The ability of the patient to recover from resuscitation will also be considered.
One doctor said: “[Who lives and who dies] is decided by age and by the [patient’s] health conditions. This is how it is in a war.”
The document says: “The growth of the current epidemic makes it likely that a point of imbalance between the clinical needs of patients with COVID-19 and the effective availability of intensive resources will be reached.
“Should it become impossible to provide all patients with intensive care services, it will be necessary to apply criteria for access to intensive treatment, which depends on the limited resources available.”
It adds: “The criteria set out guidelines if the situation becomes of such an exceptional nature as to make the therapeutic choices on the individual case dependent on the availability of resources, forcing [hospitals] to focus on those cases in which the cost/benefit ratio is more favorable for clinical treatment.”
Luigi Icardi, a councilor for health in Piedmont, said: “I never wanted to see such a moment. It [the document] will be binding and will establish in the event of saturation of the wards a precedence code for access to intensive care, based on certain parameters such as potential survival.”
The document is already complete and only approval from a technical-scientific committee is needed before it is sent to hospitals. The criteria are expected to apply throughout Italy, government sources said.
Italy has 5,090 intensive care beds, which for the moment exceeds the number of patients who need them. It is also working to create new bed capacity in private clinics, nursing homes and even in tents. However, the country also needs also doctors and nurses – the government wants to hire them – and equipment.
Lombardy remains the most critical region. However, the situation is also serious in neighboring Piedmont. Here, in just one day, 180 new cases were recorded, while deaths numbered 27. The trend suggests that the situation is not about to improve.
Roberto Testi, president of the coranavirus technical-scientific committee for Piedmont, told The Telegraph: “Here in Piedmont we aim to delay as long as possible the use of these criteria. At the moment there are still intensive care places available and we are working to create more.
“We want to arrive as late as possible at the point where we have to decide who lives and who dies. The criteria relate only to access to intensive care – those who do not get access to intensive care will still receive all the treatment possible. In medicine we sometimes have to make difficult choices but it’s important to have a system about how to make them.”
In the span of just a few weeks, the coronavirus has completely changed life as we know it, while also exposing the vast array of contradictions firmly entrenched within capitalist society. America has been laid bare as to what it always has been, a settler-colonial project that is the sole property of those who own it, as John Jay, one of the ‘Foun ding Fathers’ once argued. In the face of this disaster, Trump has predictably doubled down on painting the pandemic with a xenophobic brush as his supporters use it as yet another excuse to push half-baked conspiracy theories in order to defend the dumpster fire that is his administration. Meanwhile, outside of the gaze of neoliberal TV pundits who now pander to studios with empty audiences, across the so-called United States, autonomous groups are mobilizing to provide mutual aid to their neighbors and those hit the hardest by the exploding virus.
From Pandemic to Class War
For millions of poor and working people, life in this country is going to change – and change very quickly. Already, many companies are starting to lay off workers as the economy slows and things begin to shut down. Low wage workers, many already living just on the edge of eviction and homelessness, now find themselves with even less money coming in and with young children, recently forced out of school, to watch and feed.
In many ways, the coronavirus has accelerated all of the trajectories of modern capitalism that have hurdled us towards our current position: rapidly gentrifying cities, automation and the gig economy displacing workers into precarious forms of employment, the rising cost of living, and lack of access to affordable healthcare, education, and daycare for children. To make matters worse, soon the US will be rocked by a flood of very sick people attempting to access a broken health care system that is unprepared to handle a wide-scale pandemic.
In this moment, everyday people have to seize the initiative and get organized; before a new normal takes hold and the State can re-solidify its authority. The Trump administration will try and do this through blunt violence and police orders, as already the national guard is streaming into various cities. Democrats and the neoliberal media on the other hand will push for the country to “come together” behind Joe Biden – assuming that the November 2020 elections even are held.
If poor and working people see within the coronavirus not only a pandemic that will possibly leave in its wake a massive death count, but also the very real crisis that is modern industrial capitalism, then we must mobilize for our own interests, push back, and actually fight. This means demanding not only bread and butter: free housing, access to food, an end to evictions, and clean water: but also building new human relationships, new forms of actual life. This means creating ways of meeting our needs, making decisions, and organizing ourselves and solving problems outside of the State structure and the capitalist system.
Towards this end, we are encouraged by the explosion of grassroots and autonomous mutual aid projects that are springing up across the US. Not since the early stages of the Occupy Movement have we seen this growth of spontaneous mobilization in the face of a crisis. These efforts must continue to organize themselves, grow, network, and deepen their connections within working-class and poor neighborhoods.
What follows is both a collection of resources and links, as well as a list of active mutual aid projects that are currently mobilizing in the face of the coronavirus. We are also including a short reading list, and information on how to participate in phone-zap campaigns in support of prisoners and migrant detainees.
To have your group or mutual aid project listed, email us at: info[at] itsgoingdown [dot]org
Tacoma Mutual Aid Collective: Tacoma Mutual Aid Collective works in solidarity with Tacoma communities to support resource, knowledge, and skill sharing across our neighborhoods. Currently organizing free food programs for kids hit by school closures and beyond. Support via PayPal. Grocery program sign-up form.
Olympia Mutual Aid: We are coordinating food and supply drop offs to people’s front doors. Please use this form if you would like to help make deliveries. Facebook.
Common Stash: Mutual Aid in So-Called Olympia: We are not afraid of sickness—many of us are already sick, and those of us who are not yet sick will one day become unwell. But we are afraid of not getting cared for, of not getting what we need and of those we love not getting what they need, so we are coming together, collecting and redistributing herbal remedies, over the counter cough medication, and other supplies to our friends and neighbors. Instagram.
Oregon:
Portland-area COVID-19 “Offer Support”: We are an all-volunteer grassroots group operating in the territories of the many tribes who have made their homes near the confluence of the Willamette and Columbia Rivers, including Multnomah, Wasco, Cowlitz, Kathlamet, Clackamas, Bands of Chinook, Tualatin, Kalapuya, Molalla. Instagram and Facebook.
South Willamette Valley Mutual Aid Network: As things get harder, we show up for our neighbors. We advocate collective liberation through class solidarity, disability justice, anti-racism, abolition, and horizontal mutual aid as we reside on stolen Kalapuya land. We are trying to build a network of many neighborhood pods across Lane County. Instagram. Facebook.
Bay Area & Northern California
California:
West Oakland Punks With Lunch: Oakland based nonprofit, non religious, DIY organization that hands out lunches, harm reduction supplies, and more to our neighbors in West Oakland. Works largely with houseless community. Instagram.
South Bay Area Mutual Aid: We are coordinating food and supply drop offs to people’s front doors during the COVID-19 quarantine.
SF Bay Area: The idea behind this is to crowd source some mutual aid for folks in the SF Bay Area, who are affected by Covid-19 or the current situation.
East Bay Disabled Folks: Are you a disabled person (especially prioritizing BIPOC) in the East Bay needing extra support re COVID19?
Monterey Peninsula Aid: Please fill out this form if you live on the Monterey Peninsula and have specific needs due to the Coronavirus pandemic. Also use this form to indicate that you can help provide for the needs of other people.
Mutual Aid Los Angeles Fundraiser: Mutual Aid Action Los Angeles (M.A.A.L.A.) would like your support to continue our work and keep growing. We are committed to providing a wide range of services and support to anyone who comes through our doors and beyond. We practice Mutual Aid to live our solidarity.
Los Angeles Mutual Aid Fund: Providing mutual aid to communities in need of supplies such as drinks, food, sanitary products, clothing, and other things needed. We feel it’s up to us to provide for our communities and we must come together in solidarity in times of crisis. Any amount of donations will help and we thank you for your support!
Mutual Aid San Diego: We will be sharing this list with trusted groups doing mutual aid in San Diego, county-wide, who are organizing mutual aid. We will not use or share the info you provide for any other purpose.
Nevada:
Las Vegas Mutual Aid: Please fill out this form if you are in the Las Vegas area and are interested in offering support to people impacted by COVID-19 *OR* are requesting support for yourself/a family member.
Albuquerque Mutual Aid: In Response to COVID-19, we’re organizing mutual aid to respond to those that are often not included in conversations about public health.
Santa Fe Mutual Aid: Times seem really wild and unpredictable right now and we can isolate and hoard or possibly find a way to stay in community and help each other out. Safe distancing is important, but so is solidarity.
Arizona:
Tucson Mutual Aid: We are coordinating food and supply drop offs to people’s front doors. Please use this form if you would like to help make deliveries. Thank you!! This is a live document that will continue to change and update as we move forward.
Central
Nebraska:
Lincoln/Omaha Mutual Aid: This group is intended to be a forum for people to request and offer help specific to needs related to the COVID-19 pandemic in our area.
Montana:
Bozeman Solidarity: The volunteer will drop off the items outside of the residence, in an effort to reduce exposure.
Missoula Mutual Aid: In Missoula, we have created a COVID19 Community Organizing group, which aims to organize material support. Immediately we are providing grocery and supply deliveries. We are preparing to expand this to running errands, dog walking, childcare, caregiving, and mental/emotional support among people impacted by the pandemic. Donate here.
Colorado:
Front Range Mutual Aid: Front Range Mutual Aid Network is setting up a distribution network to get supplies to people who need them during the COVID-19 crisis.
Northern Colorado Mutual Aid and Defense: Northern Colorado Community Mutual Aid and Defense is organizing a supplies distribution service and will get your overstock to people who need it in the Greeley/Evans area. Facebook. Donate here.
Aurora Mutual Aid: A group of out of work librarians have come together to create an emergency supply kit distribution group for the elderly or families with children out of school. We have created kits that include: pasta, rice, sauce, seasonings, canned tuna, canned chicken, canned veggies, fruit cups, cookies, oatmeal, handsoap, bar soap, and toilet paper. We are targeting the North Aurora community which is our own community and are hoping to start distributing starting this morning. What we aim to do is we have set up a hotline number for those in need to call and we will drop off supply kits at the door step so they don’t have to leave the house. Call: 720-477-0406. Email: AllHandsOnDeckAurora@gmail.com
Denver Service Worker Solidarity: Many of us can not afford to miss a single shift, much less a month and a half of shifts. We need to demand an immediate moratorium on rent collection and evictions, city wide. Alone we are weak, but together we can stand strong and assure that we all make it through this difficult time, together. More details will follow, but it is important that we get our network started IMMEDIATELY. Please share this post far and wide. Bartenders, Servers, Chefs, everyone in this industry: Y’all are some of the baddest motherfuckers in the world. Let’s go!
Aid Network of Denton County: Aid Network of Denton is a coalition of organizations and individuals seeking to provide community support in the face of the COVID-19 crisis. Donate here.
Mutual Aid Central Ohio: We are building a network of people who can support their neighbors through mutual aid in Central Ohio. Facebook.
Mutual Aid Dayton/Miami Valley: We are building a network of people who can support their neighbors through mutual aid in Dayton and the Miami Valley. Facebook.
Mutual Aid Southeast Ohio: We are building a network of people who can support their neighbors through mutual aid in Southeast Ohio. Facebook.
Illinois:
Chicago Mutual Aid Volunteers: This list is being compiled to share with groups that are doing mutual aid work around COVID-19 in Chicago.
Brave Space Alliance: Brave Space Alliance will be operating a crisis food pantry for queer and trans folks on the south side of Chicago during the pandemic.
Rockford Mutual Aid Volunteers: This is for members of the Rockford community to offer skills, resources, supplies, space and time to community members who are affected by COVID – 19 and those most vulnerable among us. Facebook.
Indiana:
Bloomington Mutual Aid: Are you homebound and in need of help getting access to groceries and other supplies? For your friends and neighbors who are homebound and quarantined, are you willing to help make grocery deliveries and supply runs? Spreadsheet.
Michigan:
Kalamazoo: This list is being compiled by Kzoo Covid-19 Mutual Aid to share with groups that are doing mutual aid work around COVID-19 in Kalamazoo.
Grand Rapids Mutual Aid: Grand Rapids Area Mutual Aid Network is a hub for folks to share resources to keep each other safe and healthy. Facebook.
Huron Valley Mutual Aid: This group is for the purposes of sharing resources, needs, and info about mutual aid work that people are doing at this time.
The Mutual Aid Network of Ypsilanti: We believe that as a community we are stronger when we work together to help each other out. Our purpose is to help facilitate as much cooperation and aid as possible. Particularly focusing on the most impacted and marginalized members of our community.
Minnesota:
Twin Cities Queer and Trans Mutual Aid: The idea behind this is to crowd source some mutual aid for queer/trans/nonbinary folks in the Twin Cities area, who are affected by Covid-19 or the current situation.
Twin Cities Mutual Aid: Add yourself to a list of people willing to help each other in case of quarantine or self isolation during the COVID-19 pandemic. This information will be used to reach out of interested individuals willing to provide assistance if needed.
Madison Mutual Aid: We are using the model of mutual aid practices- basically that we can help each other in times of crisis. Facebook.
Missouri:
St. Louis Mutual Aid: Communities are safer and stronger when its members check in on one another and pitch in in whatever ways they can. This concept is called mutual aid.
First Aid Collective of Knoxville: We are an autonomous first-aid/wound collective based in Knoxville, TN. Our practices mainly focus around harm reduction, but we also supply street medicing for actions and practice mutual aid. Instagram.
North Carolina:
Chapel Hill Food Not Bombs: Offering to-go food on Saturdays at Nightlight in Chapel Hill. 430-530pm. Along with hygiene products, cleaning supplies, harm reduction. Offering delivery & drive up service. Everything is free. No questions asked. Email: foodnotbombs919@gmail.com. Instagram.
Mutual Aid Carrboro: In the coming weeks, potentially millions of workers will be sent home without pay. For the most precarious, that could mean evictions, utility shut-offs, missed payments, and other economic catastrophes. That’s why Mutual Aid Carrboro is partnering with NC Piedmont DSA to create the COVID-19 Mutual Aid Relief Fund. Donate here.
Surry County Mutual Aid Network: Our goal is to help get needed supplies to people to help prevent the spread of Covid-19 into Surry County NC.
Asheville Survival Program: In any kind of crisis we are always strongest when we work together. We can overcome our fears and the urge to isolate and hoard, to instead be part of a meaningful community wide response. Information sharing is a critical first step, from there we can work together as neighbors and friends to ensure everyone has what we need.
Atlanta:
Food 4 Life: In response to the COVID-19 pandemic crisis, we are operating a grocery delivery program in Atlanta, Georgia to ensure that those impacted by the virus will not be forced to choose between decent food and their health. Food is a human right, we must help each other! Donate here. Website.
Atlanta Mutual Aid: Students at Emory, Morehouse, Spelman, and Georgia State are facing removal and even eviction from their dorms in the response to the COVID-19 outbreak. Many students, such as international, LGBTQIA+, and out-of-state students do not have an immediate place to move to or store their belongings. Tens of thousands of students are being displaced and are in immediate need of resources and support.
Washington DC:
Takoma DC Community Care and Mutual Aid: Times that are potentially scary require us to better support one another. In the same way that we bring casseroles to grieving families and baby clothes to celebrate newborns, we can come together as a community to help each other through this difficult time.
Birmingham Mutual Aid: In these fast moving and uncertain times, it’s important to show up for each other and remember that we are not alone. Mutual aid is a powerful way to build strong connections – we all have something to offer and we all have something we need.
Kentucky:
Lexington Mutual Aid: We are building a network of people who can support their neighbors through mutual aid in Lexington, Kentucky.
Louisville Mutual Aid: We are building a network of people who can support their neighbors through mutual aid in Louisville, Kentucky.
Kentucky Mutual Aid: With the current uncertainty, it’s important that no one falls through the cracks. Facebook.
Youth Mutual Aid Fund: For young folks in Kentucky and Appalachia experiencing income loss or food and housing insecurity due to COVID-19. We’re also providing social events and general trainings to keep folks busy via video and phone calls and are available to chat with folks who are looking for social connection and need help finding resources. In the next few weeks, we’ll be expanding to ensure young folks get fair treatment from universities. Donate here.
Arkansas:
Mutual Aid Northwest Arkansas: We are building a network of folks who can support their neighbors through mutual aid in Northwest Arkansas.
Free Store Pantry in Fayetteville, Arkansas: A working food bank at 647 W. Dickson St. in Fayetteville AR. as the ongoing COVID-19 crisis continues. All donations will be to help those who do not have the means or access to food.
New Orleans Mutual Aid: As the city and country shuts down over the coming days and weeks, it is crucial that we build robust mutual aid networks that can support the elderly, the immunocompromised and the vast group of hospitality workers who have no safety net. Instagram.
Bvlbancha Collective: If you are local to the Bvlbancha area and you or a neighbor could benefit from fresh garden herbs, or plant medicines, pls contact us through email or the contact us portion of our page!!! We have herbs for immune-boosting, respiratory health, lymphatic support & working with fevers. Fresh & dried herbs for teas & steams, syrups, & some tinctures on hand. We also have a limited supply of stress relief herbs/elixirs. And more brewing right now. Plus, everything in stock from our website. No one will be declined due to lack of funds as long as we have supplies on hand. We are happy to do porch/mailbox drops as time allows. Also, we have homemade hand sanitizer! Pls, don’t hesitate to reach out! We’re in this together!
Florida:
Tampa Mutual Aid: In response to the COVID-19 epidemic, Tampa Dream Defenders and Mutual Aid Disaster Relief are partnering to support the most vulnerable in our community.
Northeast
Maryland:
Mutual Aid and Emergency Relief Fund: Food, Clothing & Resistance Collective – Maroon Movement is doing a mutual aid & emergency relief fundraising drive, and pop-up distributions, for anyone who may need some “extra assistance” to stock up food, toiletries and medical supplies in Baltimore during this still very early stage of an emerging pandemic (Covid-19), in the middle of another pandemic (Influenza). Twitter.
Pitt Mutual Aid: We‘re a team of student leaders dedicated to providing up-to-date information and resources for the COVID-19 pandemic. Check out our resource guide here.
Neighbors Helping Neighbors: We are simply neighbors helping neighbors. The aid provided comes from community support and solidarity thus we cannot guarantee to meet each request but we will be trying our best to do so . We are not funded, we are not a government or medical agency, we are simply neighbors connecting neighbors to neighbors who can help (and we happen to be organizers). Facebook.
Mutual Aid Medford and Somerville: In these fast moving and uncertain times, it’s important that we show up for each other and remember that we are not alone. Facebook.
Charles River Mutual Aid: We will be pooling funds in a Mutual Aid Fund to purchase food, medical supplies, and other necessities, and organizing to provide these resources to the community.
Tufts Mutual Aid: Tufts is closing due to COVID-19, and are compiling resources for students who need it. Fill out the form if you have resources to give, and reach out to those who have resources you need!
Solidarity Supply Distro: Solidarity Supply Distro is a coalition of leftist and anti-capitalist organizers in Boston who are building community resilience to the COVID-19 pandemic. Donate here. Facebook.
Rhode Island:
Providence Mutual Aid: Project LETS is working to support the Providence, RI community during times of increased fear, isolation, and need.
Mutual Aid Jamaica Plain & Roxbury Network: Mutual aid is a powerful way to build strong connections – we all have something to offer and we all have something we need.
New Jersey:
Central New Jersey: This form originally was asking for volunteers too, but we have enough for now! We’ll ask for more as requests come in.
North New Jersey Mutual Aid: This group is for the purposes of sharing resources, needs, and info about mutual aid work that people are doing at this time. Facebook.
New York:
Friends of Westcott Mutual Aid Group: Many of us in Westcott (Syracuse, NY) are looking for ways to help those in our neighborhood who may be affected by Covid-19. Some people in our community may have health risks. Others may be financially affected due to social distancing. This includes employees at the several businesses in our neighborhood that rely on people going out to eat and drink.
NYC United Against the Coronavirus: Massive collection of mutual aid projects and resources throughout the New York area. Includes many localized mutual aid groups.
NYC Mutual Aid Network: Mutual aid is a powerful way to build strong connections – we all have something to offer and we all have something we need.
Vermont:
Mutual Aid Hubs in Vermont: These Mutual Aid links each consist of a spreadsheet with multiple tabs for different categories of need (food, transportation, housing, emotional support, etc) and are specific to different regions of Vermont.
Durante a 22ª Conferência Estadual Espírita, neste domingo, 15, em Curitiba (PR),. Bezerra de Menezes proferiu linda mensagem espiritual de fé e força neste momento que a Terra enfrenta o Coronovírus através de psicofonia pela mediunidade de Divaldo Franco.
Ele reforça a necessidade de aprendizado e amor ao próximo neste momento de mudanças e reflexões no mundo, com ações em escalas planetárias para combater do Coronavírus.
‘Nunca houve tão bela e nobre consciência’, diz em psicofonia Bezerra de Menezes, que afirma que esse momento consequentemente será compreendido pelos nossos corações.
Confira abaixo a íntegra da psicofonia de Bezerra de Menezes:
Bezerra de Menezes observa, também, a necessidade de precaução, obedecendo as leis vigentes de contenção da pandemia. E lembra que Jesus precisa de todos nós neste momento, unindos através do ‘amor responsável’.
Amor que doa sem receber
Através da psicofonia, Dr. Bezerra de Menezes lembra de como devemos amar, nos doando, sem desejar receber nada em troca.
‘Os céus enviam seus embaixadores para quem o intercâmbio se faça com mais facilidade. Tenha cuidado para que suas ondas mentais sincronizem as mentes que administram as vidas’, ressalta, para evitarmos a agonia.
Mudança de padrão de pensamento
Em outras palavras, alerta para a mudança de padrão de pensamento e energético que precisamos desempenhar para auxiliar os trabalhadores encarnados e desencarnados no combate ao Coronavírus.
Exemplo: dedicar no final de suas preces diárias energias para toda a humanidade. Portanto, busque a serenidade, encarando esse momento como aprendizado e cura.
A medical official outside an emergency tent installed for patients infected by COVID-19 in Poland- Credit Sky News
Covid-19 is a flu-like illness (symptoms include fever, cough, and breathing problems) caused by a corona virus (SARS CoV-2). Like Ebola, the virus causing Covid-19 circulates within populations of bats and crossed over to humans via the bush meat trade. The first human cases were identified in China in December 2019, and the infection has now (March 2020) reached more than 100 countries.
The disease is now recognised by the World Health Organization as a pandemic. Up to 80 percent of the population of some countries might eventually become infected. Most cases will be mild, and recovery spontaneous. About 5 percent of cases will be life-threatening. Death rates appear to be around 1-2 percent. The elderly are most at risk.[1]
Currently, attention is focused on reducing the rate at which Covid-19 spreads. One aim is to delay the peak of infection beyond the winter flu period in the northern hemisphere, when medical help is stretched. Slowing the epidemic also allows more time for preparation of health systems to cope with large numbers, and for work on vaccine development.
Predictably, some politicians have demanded border closures against immigrants and refugees, even though spread is associated with tourism and normal business travel. Africans internationally stigmatised by Ebola might feel aggrieved that cases of Covid-19 have been introduced from Europe and Asia. But in a globally connected and inter-dependent world blaming and stigmatising helps no one. It is better to share ideas about what can be done to protect.
This is where Africa’s experience of Ebola has something to offer. Communities experiencing Ebola in West Africa in 2014-15 rapidly learnt from scratch how to cope with a deadly new infection, and this provides the rest of the world with important information on strategies to address novel disease threats more generally.
Like Ebola, Covid-19 is a family disease, in the sense that many infections occur in the home. Restrictions on travel can slow the spread of the disease, but it also helps if individuals and families understand infection pathways and implement domestic precautions. This is something in which West Africans confronted by Ebola have had much experience.
The name for Ebola in Mende, one of the main languages of Sierra Leone, the worst affected country in 2014-15, was bonda wote, literally ‘family turn round’. In other words, it was clearly recognised that this was a disease requiring families to change behaviour in major ways, especially in how they cared for the sick.
Covid-19 will require similar changes at the family level, especially in terms of how the elderly are protected. The buzz words for epidemic responders include self-isolation and social distancing, but the details of how to implement these vague concepts have been left to local social imagination.
Answers are required for both the uninfected elderly, and for others who are sick.
Should grandpa be packed off to a shed in the garden away from the family for his own protection? What happens when grandma gets lonely and wants to see the grandchildren? Who does the shopping? How does the daily-paid worker ‘self-isolate’ when there is no sick pay? Who collects the children from school when a single mum is sick?
Much depends on actual family arrangements and housing stock. So African solutions for Ebola will not work directly in other parts of the world. But it is important to know that under the challenge of Ebola local people showed much inventiveness in devising solutions to such problems.
Evidence shows that ways can be found to reduce family risks of infection, even with a disease 30 times more deadly than Covid-19.[2]For Ebola, these ranged from the elbow knock that replaced shaking of hands as a public greeting, to the appointment of a single carer in the household to look after the sick while waiting for help, to the carefully choreographed ‘safe and respectful’ funerals that allowed some element of local ritual back into the burial process, a major source of infection.
Every encouragement should be given to this local adaptive creativity, and the authorities should listen carefully to information from below about what would help to make a difference.
However, Covid-19 is not Ebola, and differences have to be taken into account. Some of the major questions about how the disease spreads are as yet unknown, and citizens and households need to be listening for this information as it becomes available and helped to adapt to its implications in real time.
This implies having very good means of two-way communication. In Sierra Leone a telephone helpline, ‘117’, played an important part in arranging emergency Ebola response, but it was much poorer at harvesting feedback from communities about what could be done better.
It seems that the lesson has not been learnt with Covid-19. In Britain, the National Health Service helpline, ‘111’ has now been ‘stood down’ for Covid-19 enquiries relating to domestic testing, since the epidemic is deemed to have passed into a new phase. How then are the authorities to have a conversation with families about the resources most needed for adaptation at household level?
Case-handling is a second area of difference. Ebola does not spread easily. The virologist Peter Piot put it well when he stated that he would have no problem sitting next to someone with Ebola provided they were not vomiting over him. Infection spreads only through contact with body fluids. Covid-19, however, spreads through the air, as well as via bodily contact, and case numbers will be much higher.
With Ebola in West Africa the number of cases turning up at specialist Ebola care facilities at the height of the epidemic numbered in tens or hundreds per week. With Covid-19 the numbers of cases requiring intensive care at the peak of the epidemic may amount to hundreds of thousands.
Even if stretched out over several months infection on this scale implies a large extra demand for medical care.
Ebola taught that epidemics cause deaths from other diseases through their impact on health systems. In all there were about 12,000 Ebola deaths in Upper West Africa (Guinea, Liberia, Sierra Leone) in 2014-15 but many additional fatalities resulted from, for example, closure of facilities such as maternity clinics.
So contingency planning is required. A key challenge for Covid-19 is how health system care should best be organized, without severely disrupting other forms of health provision.
For Ebola, the first response was to build large field hospitals (Ebola Treatment Centres).[3]These were seen as the safest option. But they were shunned by families, because so few patients came out alive. They were also often in the wrong place (built behind, not ahead, of the epidemic).
Information started to filter through that some communities were taking their own steps to reduce infection and bury the dead. This raised the question whether there was more scope for community care.
Family do-it-yourself responses proved controversial. International responders were adamant that there would be nothing resembling home care; it was too dangerous. Local communities were equally adamant that there would have to be some form of home care; they could not stand by and watch family members die, when an ambulance to take a patient to an ETC might take days to arrive over bad or non-existent roads.
Families saw it as their duty to be involved in care of the sick. So, they repeatedly asked what to do while waiting for help to arrive. Could they not prepare food for the sick? Could they not be trained to safely bury the dead?
No, they were told. Ebola required specialist management.
Communities answered back. They pointed to areas at the outset of the epidemic, where the epidemic was rolled back with only local resources. In Kailahun District, for example, an intense initial outbreak was reduced to a trickle of cases by local responders organizing quarantine and burial with improvised resources. That cases then declined without outside help implied either that the disease burnt out more readily than anticipated, or that local improvisation worked better than expected. There is evidence to support both interpretations.[4]
Experts knew that Ebola control required prompt diagnosis, before the ‘wet’ symptoms of the disease became apparent. Something had to be done to speed up the presentation of cases. The answer was to build much smaller community care centres (CCC) close to where active transmission was taking place.[5]This also changed the relationship between families and Ebola responders from fear to active cooperation.
Staff of CCC were for the most part local volunteers – trained nurses who had not been absorbed on to the payroll of the Ministry of Health, or villagers willing to take on high-risk chores for a decent wage. The fact that staffing was local meant patients saw familiar faces, and this built trust. CCC also normalized Ebola by bringing treatment within a framework of general medical assistance.
As a result, patients were presented more promptly than was the case with the distant ETC. Ebola (indistinguishable from malaria or typhoid in its early phase) was more rapidly identified and isolated. One study estimates that CCC contributed up to one third of the infection control ending the epidemic in Sierra Leone.[6]
This example of responders modifying their approach to infection control better to accommodate family requirements may hold lessons for Covid-19.
Specifically, cases may have to be kept out of main hospitals as much as possible, Thus, there may be a need for field treatment facilities not dissimilar to CCC, as a half-way house between home isolation and intensive care. In effect these facilities would isolate and triage the most vulnerable cases, as was the case with Ebola CCC.
There is also a possibility that any such facilities might be run up by military personnel[7]and staffed by medically trained ‘volunteers’ (retired doctors and nurses), as in Sierra Leone.
Interesting to note, the chief medical advisor for England was previously one of the proponents of the introduction of CCC in Sierra Leone, and we may be about to see some lessons directly transferred.[8]
Quarantine for Ebola in Sierra Leone is also an issue from which Covid-19 responders might wish to draw lessons. Much of it was organised and imposed by the state, and was at times heavy-handed. But communities also organised their own quarantine. They understood that self-isolation was in their own interest, and this sometimes worked surprisingly effectively.
Use was made of an approach used during the civil war of 1991-2002 of mobilising community youth to identify infiltrators. Visitors who might have been carrying the virus were turned away. But in other cases the approach was more focused on sequestering those who were well. Rural families sometimes decamped from villages with outbreaks to settle down for a few weeks in their farms, where sleeping quarters were sometimes built for the purpose.
In this respect, Sierra Leonean rural communities showed a clear appreciation of the fact that there were two distinct kinds of quarantine – self-isolation and protective sequestration. Both kinds are being used as part of the response to Covid-19, but at times without adequate discussion of how the two types differ and have different social motivations – self-protection and altruism towards neighbours. It is not wise to talk about self-isolation for the sick and the elderly in the same breath. The different motivations need to be more clearly explained.
In conclusion, it is also important to say something about what Africa can learn from its own experience of Ebola. The point made above should be reiterated – about the differences as well as similarities between Covid-19 and Ebola.
Prompt case finding, contact tracing and quarantine are being applied to Covid-19 as they were for Ebola.[9]Good hygiene practices, such as hand washing, also remain applicable. African countries with experience of Ebola know how to do these things, and this will be helpful in dealing with early cases.
However, African countries also have to be prepared to learn to adapt to the specific features of this new disease as more data emerge. This will pose more of a challenge, since this will require rapid knowledge-based domestic adaptation to new information on how Covid-19 spreads (perhaps most notably, why it affects the old more than the young, and how older people might be best protected from its effects).
The main lesson for both Africa and other parts of the world from Ebola for Covid-19, however, is that shared learning between communities and medical professionals is a key aspect of human adaptive response to emergent diseases. In any disease in which community mobilization is an important aspect families need to think like epidemiologists, but equally epidemiologists need to think like families.
Paul Richards’ Ebola book front cover, part of the African Arguments book series
References:
[1]Xu, J., Zhao, S., Teng T., Abdalla, A.E., Zhu, W., Xie, L., Wang, Y., Guo, X. (2020) ‘Systematic comparison of two animal-to-human transmitted human coronaviruses: SARS-CoV-2 and SARS-CoV’, Viruses 12, 244.
[2]Richards, P. (2016) Ebola: How a People’s Science Helped End an Epidemic, London: Zed Books.
[3]Richards, P., Mokuwa, E., Welmers, P., Maat, H., Beisel, U. (2019) ‘Trust, and distrust, of Ebola Treatment Centers: a case-study from Sierra Leone’, PLoS ONE14(12): e0224511. https://doi.org/10.1371/journal.pone.0224511.
[4]Glynn, Judith R. et al. (2017) ‘Asymptomatic infection and unrecognised Ebola virus disease in Ebola-affected households in Sierra Leone: a cross-sectional study using a new non-invasive assay for antibodies to Ebola virus’,Lancet Infectious Diseases17(6), 645-653. On local case finding, quarantine and burial procedures see Richards (2016) op. cit.
[5]Mokuwa, E.Y., Maat, H. (2020) ‘Rural populations exposed to Ebola Virus Disease respond positively to localised case handling: evidence from Sierra Leone’, PLoS Negl Trop Dis 14(1): e0007666. https://doi.org/10.1371/journal.pntd.0007666.
[6]Pronyk, P., Rogers, B., Lee, S., Bhatnagar, A., Wolman, Y., Monasch, R., Hipgrave, D., Salama, P., Kucharski, A., Chopra, M., and on behalf of the UNICEF Sierra Leone Ebola Response Team, (2016) ‘The effect of community-based prevention and care on Ebola transmission in Sierra Leone’,American Journal of Public Health 106, 727–32, https://doi.org/10.2105/AJPH.2015.303020.
[7]Aaaron Walawalkar and Jamie Grierson, The Guardian,8 March 2020, 14.12 GMT.
[8]Whitty, C.J.M., Farrar, J., Ferguson, N., Edmunds, W.J., Piot, P., Leach, M., Davies, S.C. (2014) ‘Tough choices to reduce Ebola transmission’, Nature515, 13 November, 192–4; see also Ian Sample and Lisa O’Carroll ‘Prof Chris Whitty – the expert we need in the coronavirus crisis’, Guardian,4 March 2020.
On July 8, 1853, Commodore Matthew Perry of the U.S. Navy sailed into Tokyo Bay with two steamships and two sailing vessels under his command. He landed a squadron of heavily armed sailors and marines; he moved one of the ships ostentatiously up the harbor, so that more people could see it. He delivered a letter from President Millard Fillmore demanding that the Japanese open up their ports to American trade. As they left, Perry’s fleets fired their guns into the ether. In the port, people were terrified: “It sounded like distant thunder,” a contemporary diarist wrote at the time, “and the mountains echoed back the noise of the shots. This was so formidable that the people in Edo [modern Tokyo] were fearful.”
This is the story of an unnatural disaster.
But the noise was not the only thing that frightened the Japanese. The Perry expedition famously convinced them that their political system was incapable of coping with new kinds of threats. Secure in their island homeland, the rulers of Japan had been convinced for decades of their cultural superiority. Japan was unique, special, the homeland of the gods. “Japan’s position, at the vertex of the earth, makes it the standard for the nations of the world,” the nationalist thinker Aizawa Seishisai wrote nearly three decades before Perry’s arrival. But the steamships and the guns changed all that. Suddenly, the Japanese realized that their culture, their political system, and their technology were out of date. Their samurai-warrior leaders and honor culture were not able to compete in a world dominated by science.
The coronavirus pandemic is in its early days. But the scale and force of the economic and medical crisis that is about to hit the United States may turn out to be as formidable as Perry’s famous voyage was. Two weeks ago—it already seems like an infinity—I was in Italy, writing about the first signs of the virus. Epidemics, I wrote, “have a way of revealing underlying truths about the societies they impact.” This one has already done so, and with terrifying speed. What it reveals about the United States—not just this administration, but also our health-care system, our bureaucracy, our political system itself—should make Americans as fearful as the Japanese who heard the “distant thunder” of Perry’s guns.
Not everybody has yet realized this, and indeed, it will take some time, just as it has taken time for the nature of the virus to sink in. At the moment, many Americans are still convinced that, even in this crisis, our society is more capable than others. Quite a lot was written about the terrifying and reckless behavior of the authorities in Wuhan, China, who initially threatened doctors who began posting information about the new virus, forcing them into silence.
On the very day that one of those doctors, Li Wenliang, contracted the virus, the Wuhan Municipal Health Commission issued a statement declaring,“So far no infection [has been] found among medical staff, no proof of human-to-human transmission.” Only three weeks after the initial reports were posted did authorities begin to take the spread of the disease seriously, confirming that human-to-human transmission had in fact occurred. And only three days later did the lockdown of the city, and eventually the entire province, actually begin.
This story has been told repeatedly—and correctly—as an illustration of what’s wrong with the Chinese system: The secrecy and mania for control inside the Communist Party lost the government many days during which it could have put a better plan into place. But many of those recounting China’s missteps have become just a little bit too smug.
The United States also had an early warning of the new virus—but it, too, suppressed that information. In late January, just as instances of COVID-19, the disease caused by the coronavirus, began to appear in the United States, an infectious-disease specialist in Seattle, Helen Y. Chu, realized that she had a way to monitor its presence. She had been collecting nasal swabs from people in and around Seattle as part of a flu study, and proposed checking them for the new virus. State and federal officials rejected that idea, citing privacy concerns and throwing up bureaucratic obstacles related to lab licenses.
Finally, at the end of February, Chu could stand the intransigence no longer. Her lab performed some tests and found the coronavirus in a local teenager who had not traveled overseas. That meant the disease was already spreading in the Seattle region among people who had never been abroad. If Chu had found this information a month earlier, lives might have been saved and the spread of the disease might have slowed—but even after the urgency of her work became evident, her lab was told to stop testing.
Chu was not threatened by the government, like Li had been in Wuhan. But she was just as effectively silenced by a rule-bound bureaucracy that was insufficiently worried about the pandemic—and by officials at the Food and Drug Administration and the Centers for Disease Control and Prevention who may even have felt political pressure not to take this disease as seriously as they should.
For Chu was not alone. We all now know that COVID-19 diagnostic tests are in scarce supply. South Korea, which has had exactly the same amount of time as the U.S. to prepare, is capable of administering 10,000 tests every day. The United States, with a population more than six times larger, had only tested about 10,000 people in total as of Friday. Vietnam, a poor country, has tested more people than the United States. During congressional testimony on Thursday, Anthony Fauci, the most distinguished infectious-disease doctor in the nation, described the American testing system as “failing.” “The idea of anybody getting [tested] easily the way people in other countries are doing it? We’re not set up for that,” he said. “Do I think we should be? Yes, but we’re not.”
And why not? Once again, no officials from the Chinese Communist Party instructed anyone in the United States not to carry out testing. Nobody prevented American public officials from ordering the immediate production of a massive number of tests. Nevertheless, they did not. We don’t know all the details yet, but one element of the situation cannot be denied: The president himself did not want the disease talked of too widely, did not want knowledge of it to spread, and, above all, did not want the numbers of those infected to appear too high. He said so himself, while explaining why he didn’t want a cruise ship full of infected Americans to dock in California. “I like the numbers being where they are,” he said. “I don’t need to have the numbers double because of one ship that wasn’t our fault.”
Donald Trump, just like the officials in Wuhan, was concerned about the numbers—the optics of how a pandemic looks. And everybody around him knew it. There are some indications that Alex Azar, the former pharmaceutical-industry executive and lobbyist who heads the Department of Health and Human Services, was not keen on telling the president things he did not want to hear. Here is how Dan Diamond, a Politico reporter who writes about health policy, delicately described the problem in a radio interview: “My understanding is [that Azar] did not push to do aggressive additional testing in recent weeks, and that’s partly because more testing might have led to more cases being discovered of coronavirus outbreak, and the president had made clear—the lower the numbers on coronavirus, the better for the president, the better for his potential reelection this fall.”
Once again: Nobody threatened Azar. But fear of offending the president may have led him to hesitate to push for aggressive testing nevertheless.
Without the threats and violence of the Chinese system, in other words, we have the same results: scientists not allowed to do their job; public-health officials not pushing for aggressive testing; preparedness delayed, all because too many people feared that it might damage the political prospects of the leader. I am not writing this in order to praise Chinese communism—far from it. I am writing this so that Americans understand that our government is producing some of the same outcomes as Chinese communism. This means that our political system is in far, far worse shape than we have hitherto understood.
What if it turns out, as it almost certainly will, that other nations are far better than we are at coping with this kind of catastrophe? Look at Singapore, which immediately created an app that could physically track everyone who was quarantined, and that energetically tracked down all the contacts of everyone identified to have the disease. Look at South Korea, with its proven testing ability. Look at Germany, where Chancellor Angela Merkel managed to speak honestly and openly about the disease—she predicted that 70 percent of Germans would get it—and yet did not crash the markets.
The United States, long accustomed to thinking of itself as the best, most efficient, and most technologically advanced society in the world, is about to be proved an unclothed emperor. When human life is in peril, we are not as good as Singapore, as South Korea, as Germany. And the problem is not that we are behind technologically, as the Japanese were in 1853. The problem is that American bureaucracies, and the antiquated, hidebound, unloved federal government of which they are part, are no longer up to the job of coping with the kinds of challenges that face us in the 21st century. Global pandemics, cyberwarfare, information warfare—these are threats that require highly motivated, highly educated bureaucrats; a national health-care system that covers the entire population; public schools that train students to think both deeply and flexibly; and much more.
The failures of the moment can be partly ascribed to the loyalty culture that Trump himself has spent three years building in Washington. Only two weeks ago, he named his 29-year-old former bodyguard, a man who was previously fired from the White House for financial shenanigans, to head up a new personnel-vetting team. Its role is to ensure that only people certifiably loyal are allowed to work for the president. Trump also fired, ostentatiously, the officials who testified honestly during the impeachment hearings, an action that sends a signal to others about the danger of truth-telling.
These are only the most recent manifestations of an autocratic style that has been described, over and over again, by many people. And now we see why, exactly, that style is so dangerous, and why previous American presidents, of both political parties, have operated much differently. Within a loyalty cult, no one will tell the president that starting widespread emergency testing would be prudent, because anyone who does is at risk of losing the president’s favor, even of being fired. Not that it matters, because Trump has very few truth-tellers around him anymore. The kinds of people who would dare make the president angry have left the upper ranks of the Cabinet and the bureaucracy already.
But some of what we are seeing is unrelated to Trump. American dysfunction is also the result of our bifurcated health-care system, which is both the best in the world and the worst in the world, and is simply not geared up for any kind of collective national response. The present crisis is the result of decades of underinvestment in civil service, of undervaluing bureaucracy in public health and other areas, and, above all, of underrating the value of long-term planning.
Back from 2001 to 2003, I wrote multiple editorials for The Washington Post about biological warfare and pandemic preparedness—issues that were at the top of everyone’s agenda in the wake of 9/11 and the brief anthrax scare. At the time, some very big investments were made into precisely those issues, especially into scientific research. We will now benefit from them. But in recent years, the subjects fell out of the news. Senators, among them the vaunted Republican moderate Susan Collins of Maine, knocked “pandemic preparedness” out of spending bills. New flu epidemics didn’t scare people enough. More recently, Trump eliminated the officials responsible for international health from the National Security Council because this kind of subject didn’t interest him—or very many other people in Washington, really.
As a nation, we are not good at long-term planning, and no wonder: Our political system insists that every president be allowed to appoint thousands of new officials, including the kinds of officials who think about pandemics. Why is that necessary? Why can’t expertise be allowed to accumulate at the highest levels of agencies such as the CDC? I’ve written before about the problem of discontinuity in foreign policy: New presidents arrive and think they can have a “reset” with other nations, as if other nations are going to forget everything that happened before their arrival—as if we can cheerfully start all relationships from scratch. But the same is true on health, the environment, and other policy issues. Of course there should be new Cabinet members every four or eight years. But should all their deputies change? And their deputies’ deputies? And their deputies’ deputies’ deputies? Because that’s often how it works right now.
All of this happens on top of all the other familiar pathologies: the profound polarization; the merger of politics and entertainment; the loss of faith in democratic institutions; the blind eyes turned to corruption, white-collar crime, and money laundering; the growth of inequality; the conversion of social media and a part of the news media into for-profit vectors of disinformation. These are all part of the deep background to this crisis too.
The question, of course, is whether this crisis will shock us enough to change our ways. The Japanese did eventually react to Commodore Perry’s squadron of ships with something more than fear. They stopped talking about themselves as the vertex of the Earth. They overhauled their education system. They adopted Western scientific methods, reorganized their state, and created a modern bureaucracy. This massive change, known as the Meiji Restoration, is what brought Japan, for better or for worse, into the modern world. Naturally, the old samurai-warrior class fought back against it, bitterly and angrily.
But by then the new threat was so obvious that enough people got it, enough people understood that a national mobilization was necessary, enough people understood that things could not go on that way indefinitely. Could it happen here, too?
Democratic presidential hopeful Sen. Bernie Sanders takes part in the 11th Democratic Party 2020 presidential debate in a CNN Washington Bureau studio in Washington, D.C., on March 15, 2020.
The final Democratic presidential debate of 2020 was a dispiriting affair for reasons that went far beyond the politics of it. The specter of COVID-19 lent a stark gloominess to the occasion, as did the seeming emptiness of the room itself: three CNN moderators, two men and the cameras. I never thought I’d miss a debate audience, but the energy was gone from that room, and the brightly lit set could not make up for it.
And then there’s this: “The Centers for Disease Control and Prevention recommended that events of 50 people or more not be held for about two months,” Bloomberg Newsreported on Sunday. “For the next eight weeks, organizers should cancel or postpone in-person events of that size throughout the U.S.”
Primaries are scheduled to be held on Tuesday in Arizona, Ohio, Illinois and Florida. These contests were set to be decisive before the CDC’s recommendation — if Joe Biden wins them all, his delegate lead over Bernie Sanders would become all but insurmountable — and may be all the more so now. These four primaries could be the last of the season. Georgia has postponed its primary, which was slated for next Tuesday, and Louisiana’s April 4 primary has likewise been delayed.
It’s quite simple: If we are listening to the CDC’s recommendations, the remaining primaries will probably be put on hold at some point, either until this thing burns itself out, or altogether depending on the circumstances. The primaries this Tuesday may happen, or they may not, but no one should be surprised if they are the last ones for a long while.
“Election dates are very, very important. We don’t want to be getting into the habit of messing around with them,” Sanders toldCNN’s Anderson Cooper in a post-debate interview. “I would hope that governors listen to the public health experts, and what they are saying is … ‘We don’t want gatherings of more than 50 people.’ I’m thinking about some of the elderly people sitting behind the desks registering people to enroll, that stuff. Does that make a lot of sense? I’m not sure that it does.”
A cancelled primary election season would be the worst of all possible outcomes, and not just because Joe Biden would basically become the Democratic nominee by default. We do elections in this country, because if we don’t, we have lost all semblance of democracy. That all-important sentiment falls to ashes in the face of the coronavirus, which has the potential to lay waste to the nation’s older and immunocompromised population if not contained.
Authorities not named Donald Trump have been warning us this situation would bring sweeping changes to our lives, and they haven’t been wrong. A shortened 2020 Democratic nomination process may soon become part of that change, so the ability of either candidate to increase their nomination chances felt blunted by the same circumstances that led them to debate each other in that bright, empty room.
Joe Biden is fortunate that Bernie Sanders was feeling conciliatory under the circumstances, because Biden lied, lied and lied throughout the evening.
Sanders was strong throughout, opening the evening with a broadside against Wall Street and the wealthy, who were taken care of by the Federal Reserve in fine style on Friday. The Fed conjured $1.5 trillion in magic money and dumped it into the banking system so businesses can still borrow without breaking themselves financially. By the end of the weekend, the interest rate had been cut to basically zero.
“Bottom line from an economic point of view,” said Sanders, “what we have got to say to the American people, if you lose your job, you will be made whole. You’re not going to lose income. If Trump can put, or the fed can put a trillion and a half into the banking system, we can protect the wages of every worker in America.”
Biden, for his part, came into the evening looking to survive without damaging himself too badly. In this, he had help from an unlikely source: his opponent. While Sanders repeatedly sought to hold Biden’s feet to the fire on various aspects of the former vice president’s voting record, it became clear early on that Sanders was not out for blood.
“I know your heart is in the right place,” Sanders said to Biden on more than one occasion, a rhetorical fig leaf intended to convey the sense that Trump is the main enemy, and these two presidential candidates share many areas of common ground. “We talk about the Green New Deal and all of these things in general terms,” said Sanders toward the end of the first hour, “but details make a difference.”
Joe Biden is fortunate that Bernie Sanders was feeling conciliatory under the circumstances, and more fortunate the CNN moderators appeared unwilling to do their jobs, because Biden lied, lied and lied again throughout the evening. When tasked to defend his serially gruesome legislative record, Biden sailed off into the land of self-serving fantasy so often that #LyinBiden and #LyingJoe were top trends on Twitter all night long.
Biden has been lying about his stance on Social Security for months now, but found a whole new gear last night. He lied straight into the camera about statements he has made and votes he has cast, as if he’d forgotten that the internet exists and such brazen bullshit artistry doesn’t fly so well anymore.
Biden was similarly slippery on his support of the bankruptcy bill, on the Hyde Amendment and reproductive rights, on his vote for the Iraq War, on the Defense of Marriage Act, and on any and all areas where his record fails to meet the standard Sanders set simply by being in the room. One of the two candidates last night spent the last 30 years being right on the signal issues of the day, and it showed.
“A time to rethink America,” indeed.
“The fact is that the idea that I in fact supported the things that you suggested is not accurate,” was a typical Biden response to Sanders throughout the evening. The CNN moderators didn’t bother trying to call Biden on his loose relationship with the truth, but Sanders persistently did so.
Biden’s most newsworthy moment of the evening came when he flatly declared that he would select a woman to serve as his vice president. “I commit that I’ll pick a woman to be vice president,” said Biden. “There are a number of women who are qualified to be president tomorrow, I would pick a woman to be my vice president.”
This was, among other things, Joe Biden paying a debt to Rep. Jim Clyburn, whose endorsement before the South Carolina primary resurrected Biden’s moribund campaign. Clyburn has made it clear that he wants Biden to select a woman for a running mate, and preferably a Black woman. Biden’s announcement last night was a “Yes, sir” telegraphed to the House majority whip via live television broadcast.
For Sanders, this debate was perhaps his last, best opportunity to make the case for his vision for the presidency as clearly as possible. As usual, he did not disappoint:
In this moment of economic uncertainty, in addition to the coronavirus, it is time to ask how we get to where we are, not only our lack of preparation for the virus, but how we end up with an economy, with so many about people are hurting at a time of massive income and wealth inequality. It is time to ask the question of where the power is in America. Who owns the media? Who owns the economy? Who owns the legislative process? Why do we give tax breaks to billionaires and not raise the minimum wage?
Why do we pump up the oil industry while a half a million people are homeless in America? This is the time to move aggressively, dealing with the coronavirus crisis, to deal with the economic fallout, but it’s also a time to rethink America, and create a country where we care about each other, rather than a nation of greed and corruption, which is what is taking place among the corporate elite.
“A time to rethink America,” indeed. A great many sacred cows — most especially capitalism and its deleterious effect on health care — are on their way to the coronavirus slaughterhouse. Whether or not we proceed with the remaining primaries, we will be other than what we are as a nation when we come out the far side of this. Bernie Sanders told us as much last night, just as he has for the full term of his public life. If and how we heed him, finally, will be up to us in the end.
The 1918 pandemic ravaged the remote city of Östersund. But its legacy is a city – and country – well-equipped to deal with 21st century challenges
Brian Melican
Wed 29 Aug 2018 07.15 BST Last modified on Mon 3 Feb 2020 12.47 GMT
Spanish flu reached Östersund a century ago. Photograph: Alamy
On 15 September 1918, a 12-year-old boy named Karl Karlsson who lived just outside Östersund, Sweden, wrote a short diary entry: “Two who died of Spanish flu buried today. A few snowflakes in the air.”
For all its brevity and matter-of-fact tone, Karlsson’s journal makes grim reading. It is 100 years since a particularly virulent strain of avian flu, known as the Spanish flu despite probably originating in America, ravaged the globe, killing somewhere between 50 million and 100 million people. While its effects were felt everywhere, it struck particularly hard in Östersund, earning the city the nickname “capital of the Spanish flu”.
“Looking back through contemporaneous accounts was quite creepy,” says Jim Hedlund at the city’s state archive. “As many people died in two months as generally died in a whole year. I even found out that three of my forbears were buried on the same day.”
There were three main reasons why the flu hit this remote city so hard: Östersund had speedy railway connections, several army regiments stationed in close quarters and a malnourished population living in cramped accommodation. As neutral Sweden kept its armed forces on high alert between 1914 and 1918, the garrison town’s population swelled from 9,000 to 13,000.
By 1917, when navvies poured in and construction started on an inland railway to the north, widespread food shortages had led to violent workers’ demonstrations and a near mutiny among the army units.
The city became a hotbed of political activism. Its small size put the unequal distribution of wealth in early industrial society under the microscope. While working-class families crowded into insalubrious accommodation, wealthy tourists from other parts of Sweden and further afield came for the fresh mountain air and restorative waters – as well as the excellent fishing and elk hunting (passionate angler Winston Churchill was a regular visitor).
“The catastrophic spread of the flu was in no small part down to the authorities’ bewilderment and often clumsy reactions” – Hans Jacobsson, historian
“Many of the demonstrators’ concerns seem strikingly modern,” says Hedlund, pointing to a copy of a political poster that reads: “Tourists out of our buildings in times of crisis. Butter, milk and potatoes for workers!”
It wasn’t just the urban proletariat demanding better accommodation. At Sweden’s first ever national convention of the indigenous Sami peoples held in Östersund in early 1918, delegates demanded an end to discriminatory policies that forced them to live in tents.
Social inequality in the city meant the Spanish flu hit all the harder.
As the epidemic raged in late August, when around 20 people were dying daily, the city’s bank director Carl Lignell withdrew funds from Stockholm without authorisation and requisitioned a school for use as a hospital (the city didn’t have one).
‘You can drop your kids off at kindergarten on the way to work and be out hiking or skiing by late afternoon.’ Photograph: Sergei Bobylev/TASS Advertisement
“If it hadn’t been for him, Östersund might quite literally have disappeared,” says Hedlund. For a brief period, Lignell worked like a benevolent dictator, quarantining suspected cases in their homes – and revealing the squalor in which they lived.
As his hastily convened medical team moved through Östersund, they found whole families crowded into wooden shacks, just a few streets away from the proud, stone-built civic structures. In some homes, sick children lay on the floor for want of beds.
The local newspaper Östersunds-Posten asked rhetorically: “Who would have thought that in our fine city there could be such awful destitution?”
People of all political convictions and stations in life started cooperating in a city otherwise riven by the class divisions of early industrial society. Östersunds-Posten itself moved from simply reporting on the epidemic to helping to organise relief, publishing calls for money, food and clothing, and opening its offices for use as storerooms. The state had proven itself inadequate, as historian Hans Jacobsson wrote: “The catastrophic spread of the Spanish flu in 1918 was in no small part down to the authorities’ bewilderment and often clumsy reactions.”
“After the epidemic, the state made tentative steps towards a cooperative approach to social reform” – Jim Hedlund, archivist
He cites the fact that Stockholm High Command refused to halt planned military exercises for weeks, despite the fact that regimental sickbays were overflowing. “What is interesting is that, after the epidemic, the state dropped investigations against Lignell and made tentative steps towards a cooperative approach to social reform. Issues such as poor nutrition and housing were on the political agenda,” says Hedlund. Anyone trying to date the inception of Sweden’s welfare state cannot overlook the events of autumn 1918.
One hundred years on, there are few better places than Östersund to see the effects of Sweden’s much-vaunted social model. The city is once again growing rapidly, but nothing could seem further away than epidemics and political radicalism. The left of centre Social Democrats have been in power in city hall since 1994, and council leader AnnSofie Andersson has made housing a priority – new developments are spacious, well-ordered and equipped with schools and playgrounds.
“There’s nothing that shows confidence like building stuff,” she says. “In fact, our local authority building partnership should, in my view, keep a small excess of flats in hand, because without a reserve people won’t move here.”
Östersund attracts a net inflow of people from southern Sweden. “It’s partly a quality of life issue,” says Andersson. “You can drop your kids off at kindergarten in the morning on the way to work and be out hiking or skiing by late afternoon.”
The city has recovered from the relocation of the Swedish armed forces fighter jet squadron in the 1990s by playing to its strengths: sports and tourism. A university now occupies the old barracks with a special focus on sports materials and technology. The airbase has become a thriving airport, handling half a million passengers a year.
Despite the net inflow of working-age people however, Östersund is facing a demographic challenge as baby boomers begin to retire. The shortages are being felt most acutely at the regional health authority, which occupies the Epidemisjukhus – the building hastily converted into wards during the Spanish flu by Carl Lignell. Clinical staff are proving hard to find and retain, and the region’s health service is underfunded. Some residents still suggest solving that lack of funding from central government “the Jämtland way”, like Lignell once did.
History doesn’t repeat itself identically, though. Sweden’s consensus-orientated political model now tends to defuse conflict even in proud cities with a liking for mavericks. One of Andersson’s strategies for dealing with the approaching lack of labour, for instance, is cooperating with local and national institutions to train up the young refugees the city has welcomed since 2015.
“School starts tomorrow – for the last time,” confides Karl Karlsson to his journal on 4 September 1918. “I leave in spring and it feels melancholy. I like farming, but I would still prefer to continue at school and study. But it’s impossible.” Ten days later, he notes that his family’s food stores are running low. “We’re almost out of flour and bread, the barley hasn’t dried yet, and we shan’t get any more rations, everything is being requisitioned.”
One hundred years later, a city – and a society – once unable to educate or even feed its youth is now one of the world’s wealthiest and fairest.




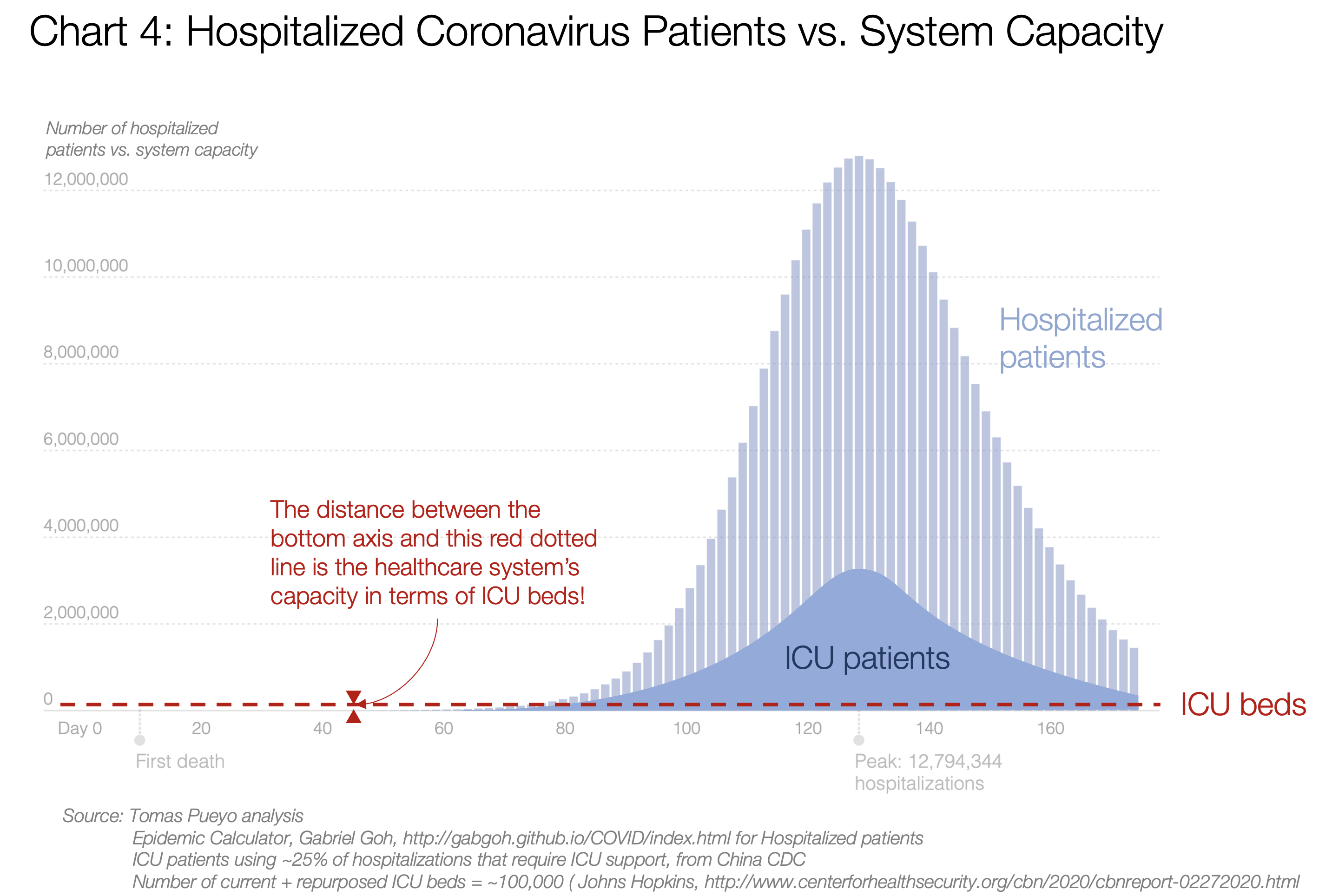

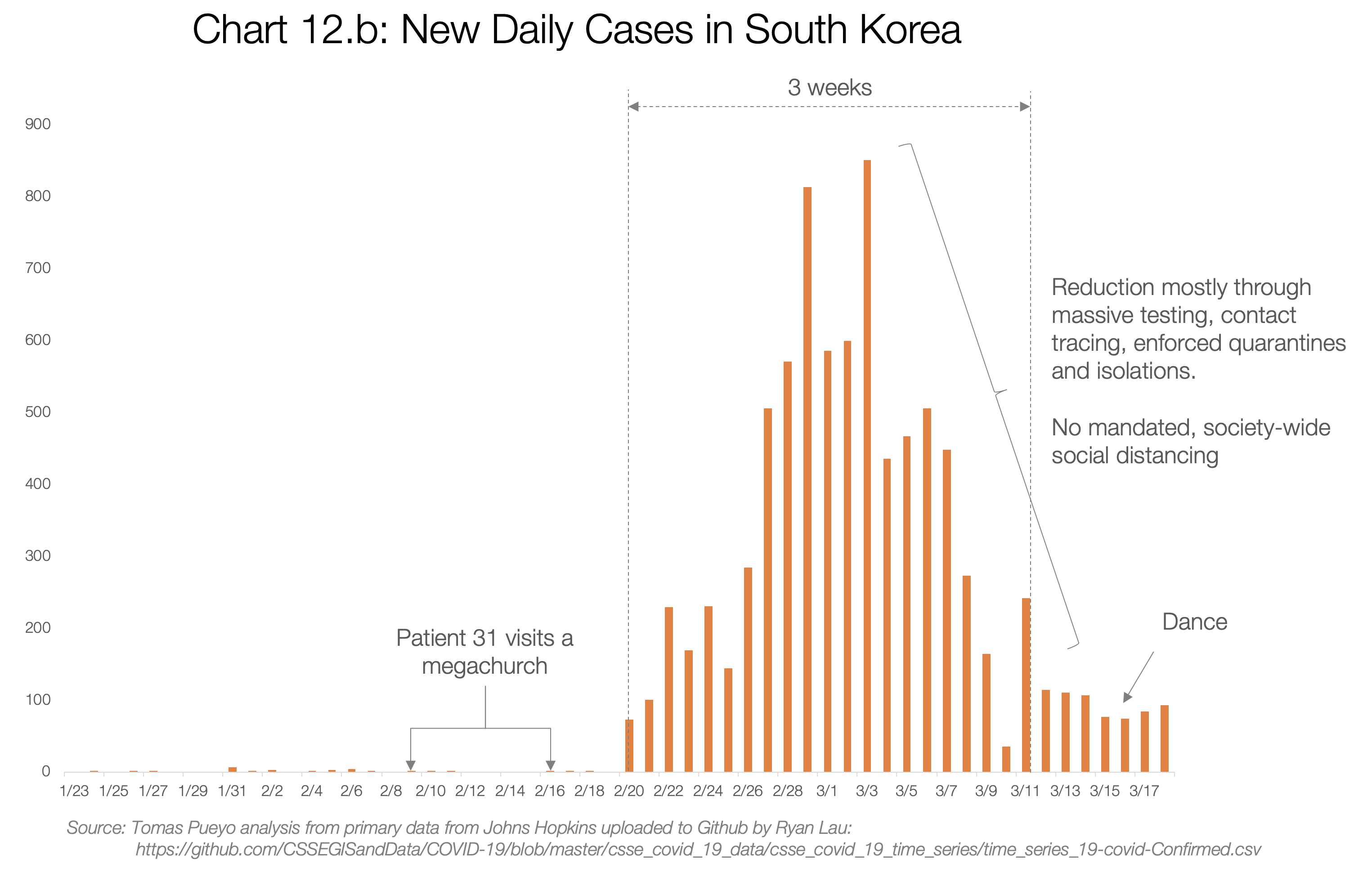
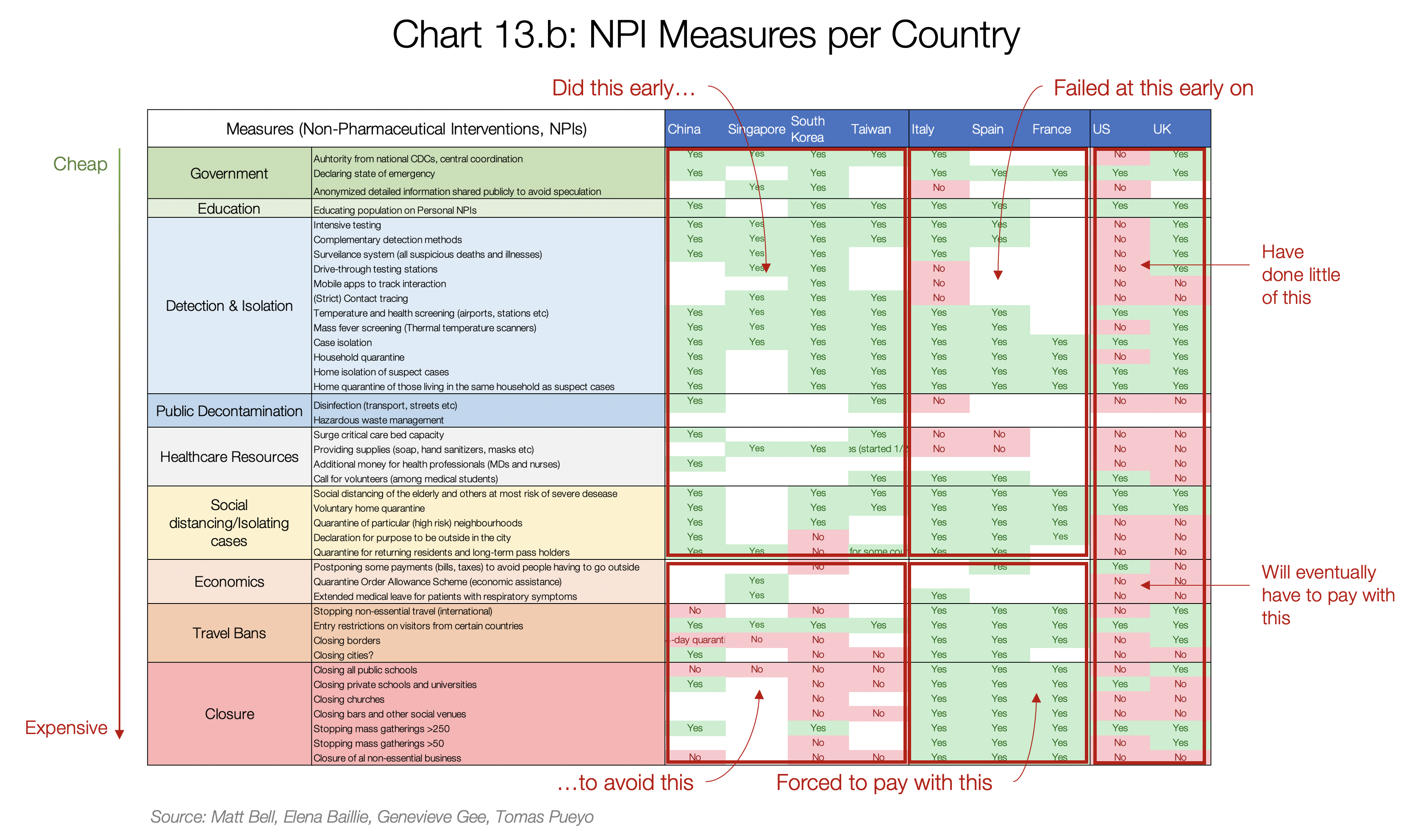

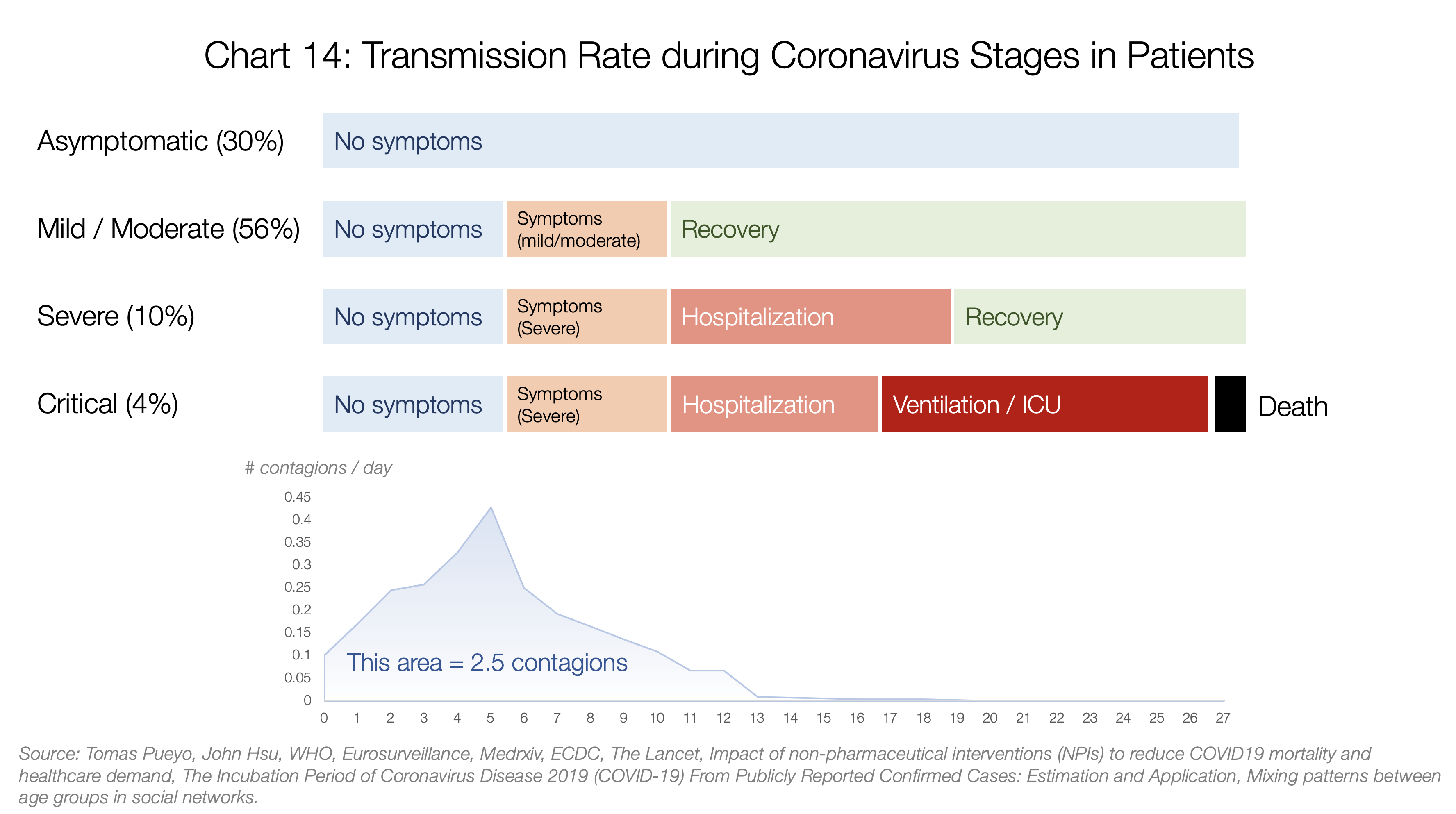
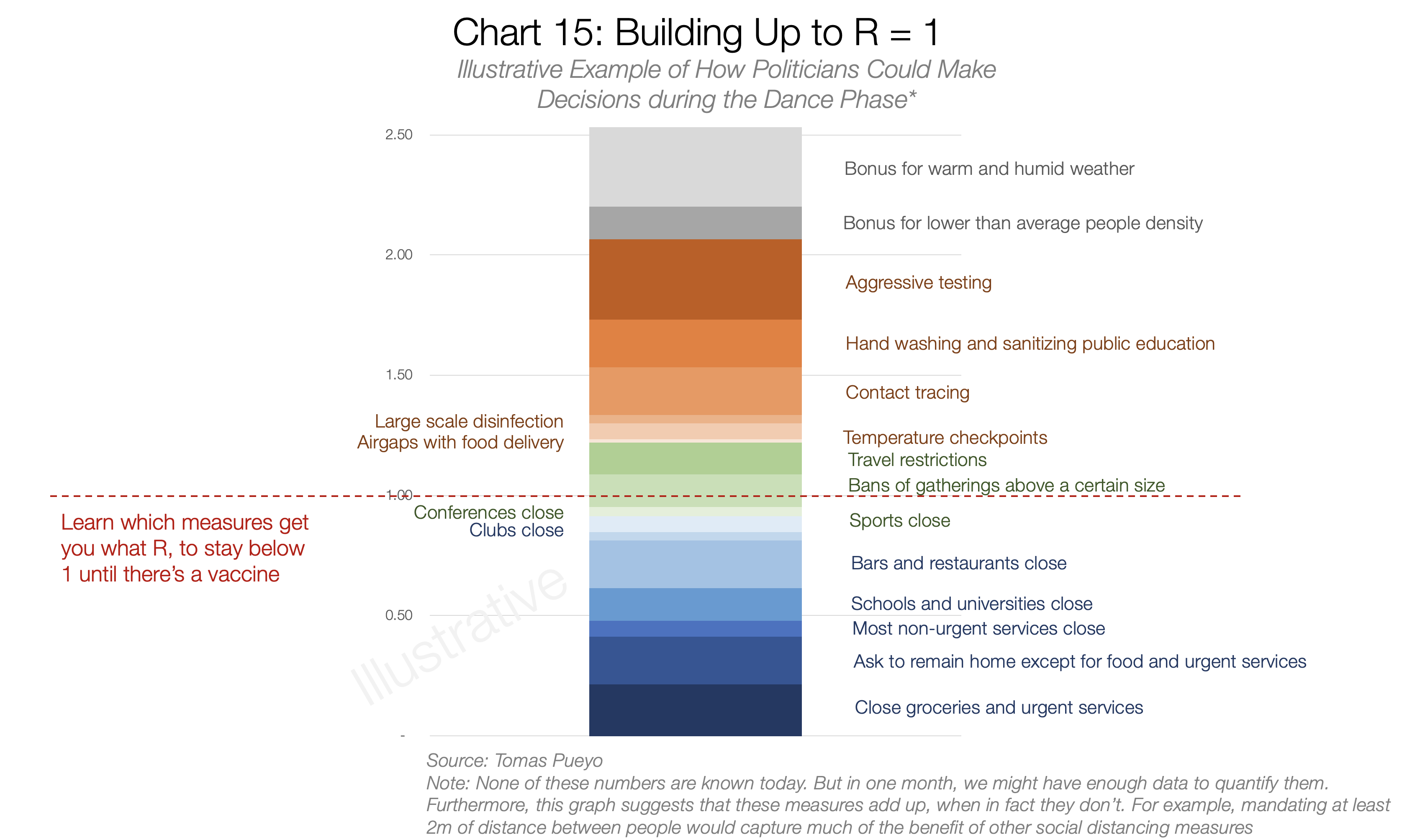






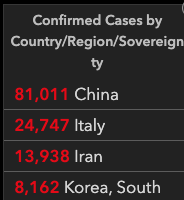




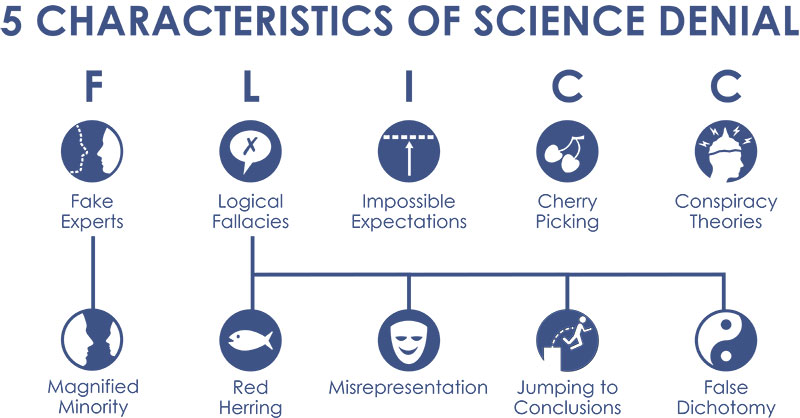



 Foto: Marcelo Casal Jr/Agência Brasil
Foto: Marcelo Casal Jr/Agência Brasil 











Você precisa fazer login para comentar.